Page 16 of 22
OP1.5 | Amblyopia: Types, Prevention and Refractive Treatment — SDL Guide (Part 2)
Examination and Diagnosis: How to Identify Amblyopia Clinically
Amblyopia is a diagnosis of exclusion — the VA loss must not be fully explained by a structural cause. The clinical examination therefore has two objectives: to document the VA loss and to rule out an organic cause.
The key examination steps for suspected amblyopia are:
1. Visual acuity in each eye separately: using age-appropriate methods (Cardiff cards or Kay pictures for pre-verbal children; Snellen for children who know letters). The critical finding is an inter-eye VA asymmetry of 2 or more lines on the Snellen chart (one eye reads 6/9, the other 6/36 — a 2-line difference) OR any eye that cannot achieve 6/6 with optimal optical correction.
2. Pinhole test: if VA is reduced, the pinhole test is performed. In amblyopia, VA does NOT improve significantly with a pinhole — because the problem is cortical (not optical). Improvement with pinhole in a child suggests uncorrected refractive error that may respond to spectacles alone.
3. Cycloplegic refraction (mandatory in all children with asymmetric or subnormal VA): cycloplegia (cyclopentolate 1% for >1 year; atropine 1% for <1 year or very uncooperative patients) reveals the full refractive error, including latent hypermetropia and anisometropia. Without cycloplegia, anisometropic amblyopia will be systematically under-detected.
4. Cover/uncover test and alternate cover test: to detect strabismus (a constant squint = risk factor for strabismic amblyopia). The cover-uncover test reveals a manifest squint; the alternate cover test (disrupts binocular fusion) reveals a latent squint. Any constant unilateral squint requires urgent follow-up.
5. Red reflex examination: in neonates and infants, the red reflex (Brückner test with a direct ophthalmoscope) detects media opacities (congenital cataract → white/absent red reflex), corneal disease, or retinoblastoma (absent/white reflex — leukocoria). An absent or asymmetric red reflex in a neonate requires SAME-DAY ophthalmology referral.
6. Anterior segment and fundus examination: to exclude structural causes — cataract (slit lamp), retinal disease (fundoscopy — macular scar, optic atrophy).
SELF-CHECK
In a 3-year-old with suspected amblyopia, why is cycloplegic refraction (using atropine or cyclopentolate) essential, rather than simply measuring refraction with an autorefractor without cycloplegia?
A. Autorefractors give higher accuracy in adults but not in children
B. A 3-year-old's powerful accommodation can compensate for high hypermetropia, masking the full refractive error
C. Cycloplegia dilates the pupil so the examiner can see the fundus more clearly
D. Cycloplegia eliminates myopia so only hypermetropia is revealed
Reveal Answer
Answer: B. A 3-year-old's powerful accommodation can compensate for high hypermetropia, masking the full refractive error
A young child (especially under 8 years) has a powerful amplitude of accommodation — often 10–14 D — which can compensate for very large hypermetropic errors. Without cycloplegia, the ciliary muscle is actively contracting and the true hypermetropia is hidden ('latent hypermetropia'). A non-cycloplegic measurement in a child with +6.00 D of hypermetropia might show only +1.00 D. This means anisometropia and bilateral high hypermetropia — the leading causes of refractive amblyopia — would be under-detected or missed entirely. Cycloplegia paralyses the ciliary muscle, fully relaxing accommodation and revealing the true total refractive state.
Differential Diagnosis: Amblyopia vs Organic Visual Loss
The diagnosis of amblyopia requires careful exclusion of organic causes, because the treatment of amblyopia — occlusion of the fellow eye — would be dangerous if the vision loss was actually due to structural optic nerve or retinal disease. A child who has an optic nerve tumour causing VA loss in one eye should NOT have their only well-seeing eye patched. This makes the differential diagnosis not merely an academic exercise but a patient safety imperative. The clinical challenge is that amblyopia and organic disease can superficially resemble each other: both present with unilateral reduced VA in a child, VA that does not improve with a pinhole, and a structurally normal-appearing eye on casual inspection. The distinction requires a systematic examination that targets the specific clinical signs that separate cortical visual loss (amblyopia) from structural pathway disease. The single most powerful differentiating test is the assessment for a relative afferent pupillary defect — because amblyopia, regardless of its severity, never causes an RAPD. Understanding why this is the case — the pupillary light reflex depends on retinal and optic nerve integrity, not on cortical development — is as important as knowing the test itself. The distinguishing features are:
Features suggesting amblyopia:
- VA loss in one eye does NOT improve with pinhole OR with optimal spectacle correction
- VA loss is in the expected amblyogenic setting: anisometropia, strabismus, or history of media opacity
- The fundus, optic disc, and anterior segment are structurally normal
- Pupils: no relative afferent pupillary defect (RAPD) — an absent RAPD in the setting of unilateral reduced VA strongly suggests amblyopia rather than optic nerve disease
- No symptoms of organic disease (no pain, no distortion, no field loss)
Features that should prompt investigation for organic disease:
- Presence of a RAPD (afferent pupil defect) — this is the most important sign; a true RAPD indicates optic nerve or retinal disease, NOT amblyopia
- Pale optic disc (optic atrophy) on fundoscopy
- Macular scarring, pigmentary change, or haemorrhage
- The visual loss is progressive rather than stable
- The loss involves the fellow eye too
- The pattern of VA loss does not match the degree of anisometropia or the presence of strabismus
The RAPD is the key differentiating test: amblyopia does not cause an afferent pupil defect, no matter how severe the amblyopia. If a child with apparent amblyopia has an RAPD, investigate for optic nerve glioma, demyelination, or retinal pathology before patching the fellow eye.
CLINICAL PEARL
The crowding phenomenon in amblyopia: Children with amblyopia often read single isolated letters better than a line of letters on the Snellen chart — because adjacent letter contours interact (suppress each other in the amblyopic cortex), making row-reading harder than single-letter reading. This 'crowding' or 'separation difficulty' is not present in organic visual loss, where the patient consistently reads the same letters regardless of context. When a child reads the 6/6 single-letter acuity card but only 6/24 on the Snellen line, this pattern is virtually diagnostic of amblyopia. Conversely, a patient with organic macular disease reads individual letters consistently — the acuity is the same whether letters are isolated or in a line. This clinical distinction requires no special equipment — just two different card presentations — and is highly useful in clinic.
Prevention and Treatment: Optical Correction, Patching and Penalisation
Treatment of amblyopia is most effective when started early in the critical period, and the treatment urgency increases with the age of the child. The window of maximum neuroplasticity — before age 7 — is when the greatest improvement can be achieved. After age 10–12 years, treatment produces diminishing returns; after 14–17 years, treatment is generally not initiated as routine (though the critical period boundary is not absolute — some plasticity persists beyond age 7, and the PEDIG trials showed benefit in children up to 12 years).
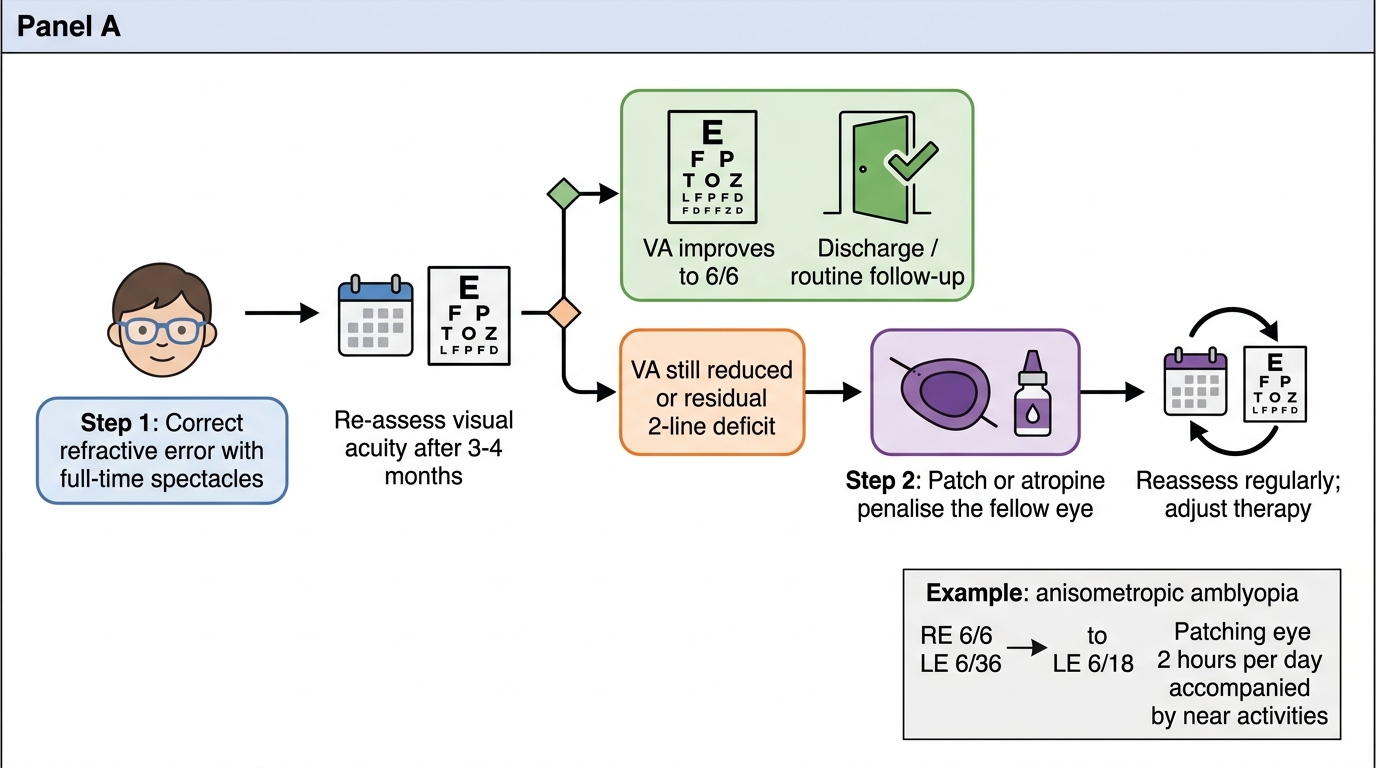
Treatment algorithm:
STEP 1 — Optical correction (mandatory, ALWAYS first):
The first and most important treatment step is correction of the underlying refractive error with appropriate spectacles (based on cycloplegic refraction). Many cases of anisometropic amblyopia — particularly mild-to-moderate forms in young children — improve dramatically with spectacle correction alone, without any patching. The mechanism: equalising the retinal image quality in both eyes allows normal visual cortical competition to resume. Full-time spectacle wear for 3–4 months is required before reassessing VA and deciding whether further treatment is needed. Prescribing spectacles and patching simultaneously as the first step is no longer recommended (because it prevents identifying cases that respond to spectacles alone).
STEP 2 — Occlusion therapy (patching) if VA remains reduced after spectacle correction:
The dominant (fellow) eye is patched, forcing the brain to use the amblyopic eye and stimulating cortical development. Patching can be done with:
- Adhesive occlusive patches (most effective; worn over the skin around the eye, not on the spectacle lens — children may 'peep' around a spectacle-mounted occluder)
- Bangerter foils (translucent foils on the spectacle lens; provide less dense penalisation; useful for mild amblyopia)
Patching duration: the PEDIG trials demonstrated that 2 hours per day of prescribed activities (near activities such as puzzles, reading, drawing that stimulate the amblyopic eye during patching) is as effective as 6 hours per day for moderate amblyopia (VA 6/24 to 6/36). For severe amblyopia (VA <6/60), full-time patching during waking hours is recommended initially.
STEP 2 alternative — Atropine penalisation:
Atropine 1% drops instilled in the fellow (dominant) eye once daily (or even just on weekends — the PEDIG weekend-dose study showed equivalence to daily dosing for moderate amblyopia) blur that eye's near vision by paralysing accommodation. This forces the child to use the amblyopic eye for near vision. Advantages: no compliance issues with the patch (children often resist patching); easier for families. Disadvantages: the fellow eye retains some distance vision (atropine only blurs near), so the penalisation is less dense — most effective for moderate, not severe, amblyopia.
Monitoring: VA is reassessed every 6–12 weeks during treatment. Treatment continues until VA in the amblyopic eye reaches its best achievable level (stable for 2 consecutive visits) or until the child's age makes further response unlikely. Over-patching (occlusion amblyopia in the fellow eye) is a rare complication of excessive, unsupervised patching — periodic fellow-eye VA checks prevent this.
Treatment Algorithm for Amblyopia
SELF-CHECK
An 8-year-old is diagnosed with anisometropic amblyopia: RE 6/6, LE 6/36 with cycloplegic refraction showing LE +4.50 D. After 4 months of full-time spectacle wear, VA improves to LE 6/18. There is still a residual 2-line deficit. What is the MOST appropriate next step?
A. Continue spectacles alone for another 12 months — VA may continue to improve spontaneously
B. Initiate patching of the dominant (right) eye for 2 hours per day with near activities
C. Refer for surgical correction of the anisometropia
D. Discharge — VA of 6/18 is functionally adequate for a child
Reveal Answer
Answer: B. Initiate patching of the dominant (right) eye for 2 hours per day with near activities
After an adequate trial of optical correction (spectacles) alone, the residual VA deficit in the amblyopic eye — at this age still within the treatable critical period — warrants occlusion therapy. The PEDIG trials demonstrated that 2 hours per day of patching with engaging near activities (puzzles, reading, drawing) is as effective as 6 hours/day for moderate amblyopia. The DOMINANT (right) eye is patched to force use of the amblyopic eye. Option A is incorrect because the initial spectacle-response period is over (4 months is adequate); further improvement with spectacles alone is unlikely. Surgical correction treats refractive error but not the cortical amblyopia. VA of 6/18 is NOT adequate — the goal is 6/6 or as close as possible.
Self-Assessment: Applying Amblyopia Knowledge Clinically
Use these scenarios to test your ability to apply — not merely recall — the clinical principles of amblyopia diagnosis and management. Work through each before consulting your notes.
Scenario 1: A 5-year-old girl is brought by her mother, who noticed the child squinting the left eye inward when looking at the television. VA: RE 6/6, LE 6/48. The cover test reveals a constant left esotropia. Pinhole: LE remains 6/48. Cycloplegic refraction: RE +1.50 D, LE +1.75 D — nearly symmetric. Fundoscopy and anterior segment are normal. (a) What type of amblyopia is this, and why? (b) Is the anisometropia sufficient to explain the amblyopia? (c) What is the first treatment step? (d) When, if ever, would you consider surgical correction of the esotropia?
Scenario 2: A 6-year-old boy has VA 6/6 RE, 6/60 LE. The left VA does not improve with pinhole or with optimal spectacle correction (+4.50 D LE, +1.00 D RE). Fundoscopy: left optic disc appears slightly pale. The swinging flashlight test reveals a left RAPD. (a) Does the RAPD change the diagnosis from amblyopia? Explain why. (b) What organic diagnoses should now be considered? (c) Should you patch the right eye at this stage? What is the risk of doing so without further investigation?
Scenario 3: Preethi from the hook is now being followed up. After 4 months of full-time spectacle wear (LE +4.50 D), LE VA improved from 6/60 to 6/24. She is now 8 years old. (a) Is optical correction alone sufficient at this point? (b) Describe the next treatment step, including the specific PEDIG-based dosing recommendation. (c) What is the risk of over-patching, and how do you prevent it? (d) What is the realistic prognosis for achieving 6/6 in the left eye at her current age?
Review your answers against the treatment algorithm section. Any uncertainty about the RAPD distinction or the PEDIG dosing evidence indicates material to revisit before your clinical posting.