Page 5 of 22
OP1.2 | Refractive Errors: Classification and Correction — SDL Guide
Learning Objectives
- Define refractive error and explain the concept of emmetropia and ametropia
- Classify myopia, hypermetropia, astigmatism and presbyopia with their subtypes
- Explain the optical basis of each refractive error and its far point
- Describe the methods of correction (spectacles, contact lenses) for each type
- Identify the complications of pathological (high) myopia
- Outline the public health significance of refractive errors in India
INSTRUCTIONS
Refractive errors are the most prevalent cause of visual impairment worldwide, and also one of the most readily correctable. A large proportion of the patients that a general practitioner or ophthalmologist encounters present with blurring of vision due to simple refractive errors — myopia, hypermetropia, astigmatism, or presbyopia. Understanding the optics, classification, and correction of these conditions is foundational to clinical ophthalmology practice and to the National Programme for Control of Blindness and Visual Impairment (NPCBVI), which counts uncorrected refractive error as a major preventable cause of vision loss.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch 3-4. (textbook)
- Parsons J, Duke-Elder S. Diseases of the Eye, 22nd ed. Elsevier, 2011. Ch 4-6. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan, a 19-year-old first-year MBBS student, is seated in the back row but cannot read the projected slides clearly. He squints constantly, which temporarily sharpens his vision. His near vision is perfect — he can read textbooks without difficulty. His optometrist measures −4.00 D in both eyes. In the same clinic, Prof. Krishnaswamy, a 52-year-old physician, holds his mobile phone at arm's length to read a WhatsApp message. His distance vision remains crystal clear, but reading has become progressively difficult since his mid-forties. He now uses +2.00 D reading glasses. Both men have refractive errors — but of opposite types, with opposite optical solutions, and arising from entirely different mechanisms.
WHY THIS MATTERS
Uncorrected refractive errors are the leading cause of visual impairment globally and the second most common cause of blindness worldwide after cataract (WHO, 2019). In India, the National Programme for Control of Blindness and Visual Impairment (NPCBVI) has specifically targeted refractive error correction — free spectacle distribution, school screening programmes, and vision centres — because correcting a refractive error with a simple lens costs a fraction of what blindness costs society. As a future physician, you will be the first point of contact for patients with visual blurring, and recognising that a patient's problem is refractive (and not a sign of retinal disease, glaucoma, or cataract) is a core diagnostic skill. The pinhole test — one of the simplest instruments in medicine — is your bedside separator (covered in OP1.3).
RECALL
From OP1.1 (visual optics), recall: the emmetropic eye brings parallel light to a precise focus on the retina with accommodation fully relaxed — far point at infinity; total refracting power ~60 D (cornea ~43 D + lens ~17–20 D); the crystalline lens is the variable component, altered by the ciliary muscle through accommodation. From Year-1 physics: a concave (minus) lens diverges light, moving the focal point backward; a convex (plus) lens converges light, moving the focal point forward. These physical principles directly explain why each refractive error is corrected by the lens type it is.
Clinical Presentation: How Patients with Refractive Errors Present
Refractive errors are among the most common reasons a patient visits a clinic — yet their presentations are easily misread, especially in children who cannot articulate visual difficulty. Each type of refractive error produces a characteristic clinical story that the physician can recognise before any instrument is placed in front of the eye.
The myopic patient typically presents in adolescence or young adulthood with the complaint that distant objects are blurred while near vision remains clear. They may squint habitually — screwing up the eyelids to create a pinhole effect — which transiently sharpens distant vision. They may have headaches from the effort of squinting, and they consistently prefer to sit near the front of the classroom or close to the television screen. A child who cannot see the whiteboard but reads textbooks effortlessly is myopic until proven otherwise.
The hypermetropic patient's presentation is less intuitive. Mild-to-moderate hypermetropia in a young patient is often clinically silent because accommodation compensates fully for the error — the patient may have 6/6 unaided vision in both eyes yet still have a significant refractive error. The presenting complaint is frequently asthenopia: frontal headache, eye strain, or blurring of print after prolonged near work, because the ciliary muscle is working continuously to overcome the hypermetropia. In children, high hypermetropia presents as convergent squint (accommodative esotropia) — the excessive accommodative drive required for clear vision also drives excessive convergence, turning the eye inward.
Astigmatic patients describe blurring at all distances, often with monocular diplopia (ghost images), and frequently tilt or rotate their head to find a clearer meridian. Presbyopic patients present with the classic history of gradually holding reading material at arm's length, needing brighter light to read, and experiencing difficulty with fine print — typically from the mid-forties onward. Understanding these presentations as clinical patterns — before reaching for the trial frame — is the starting point for all refractive assessment.
Myopia: Definition, Types, Pathophysiology and Complications
Myopia (short-sightedness, near-sightedness) is the most prevalent refractive error globally and is increasing rapidly in prevalence — particularly in East Asian and urban populations, where rates of up to 80–90% in young adults have been reported in some cities. Its defining optical characteristic is that parallel light from infinity, after refraction through the unaccommodated myopic eye, converges to a focal point ANTERIOR to the retina, producing a blurred retinal image for distant objects. The far point of a myopic eye is at a finite distance in front of the eye (e.g. for −4.00 D myopia, the far point is at 25 cm). Because the far point is real and in front of the eye, myopic patients see near objects clearly — the divergent light from a near source converges naturally on the retina, sometimes without any accommodation. This explains the classic clinical presentation: clear near vision, blurred distance vision. The degree of myopia directly predicts the distance of clear vision: a −2.00 D myope sees clearly up to 50 cm, a −4.00 D myope up to 25 cm, a −10.00 D myope up to 10 cm. Understanding this relationship between dioptre value and far point distance is foundational to both the clinical assessment and the correction of myopia.
Classification by cause:
- Axial myopia (commonest): the axial length of the eye (normal ~23–24 mm) is increased, while the refracting power is normal. For every 1 mm increase in axial length, myopia increases by approximately 3 D. This is the type that progresses through childhood and adolescence.
- Refractive myopia: the axial length is normal, but the refracting power is excessive — due to a steeply curved cornea, an overaccommodated (spastic) ciliary muscle (pseudomyopia, reversible with cycloplegia), or a dense nuclear cataract (index myopia, due to increased refractive index of the sclerotic lens nucleus).
Classification by degree:
• Low myopia: up to −3.00 D
• Moderate myopia: −3.00 to −6.00 D
• High (pathological) myopia: greater than −6.00 D (axial length typically >26 mm)
Pathological (degenerative) myopia is an important diagnosis because the excessive axial length stretches the retina and choroid, leading to:
- Posterior staphyloma (outpouching of the posterior sclera)
- Lattice degeneration → retinal tears → rhegmatogenous retinal detachment (a sight-threatening emergency)
- Fuchs' spot (Forster-Fuchs): dark macular pigmentary lesion from subretinal choroidal neovascularisation
- Glaucoma risk: increased axial length is associated with open-angle glaucoma
- Cataract: nuclear sclerosis occurs earlier
Correction: myopia is corrected with a concave (diverging, minus) lens, which moves the focal point back to the retina.
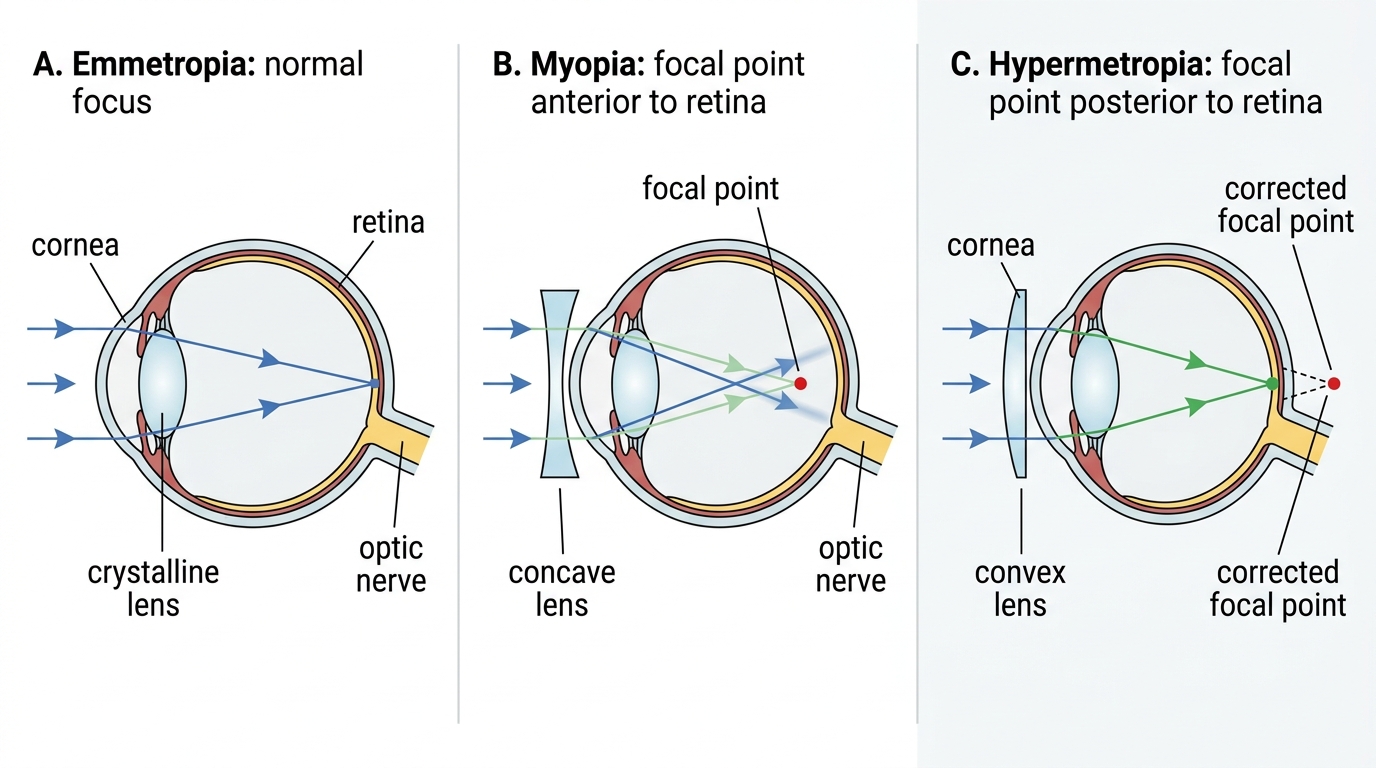
Optics of Emmetropia, Myopia, and Hypermetropia
SELF-CHECK
A 14-year-old girl has difficulty reading the blackboard. Examination reveals: distance VA 6/60 in both eyes, near VA N6 (normal), and VA improves to 6/6 with a −3.00 D lens. Which of the following BEST describes the optical basis of her condition?
A. The focal point of parallel light falls posterior to the retina
B. The focal point of parallel light falls anterior to the retina
C. Different meridians of the cornea have different refracting powers
D. The amplitude of accommodation has declined due to lens hardening
Reveal Answer
Answer: B. The focal point of parallel light falls anterior to the retina
In myopia, parallel light (from distant objects) converges to a focal point ANTERIOR to the retina when accommodation is relaxed — this is what blurs distance vision. Near objects produce divergent light, which the myopic eye can bring to focus naturally at the retina (or with minimal accommodation), hence near vision is preserved. A minus (concave) lens corrects this by diverging the light so that the focal point moves back to the retina. Option A describes hypermetropia; C describes astigmatism; D describes presbyopia.
Hypermetropia: Definition, Classification and Clinical Features
Hypermetropia (long-sightedness, hyperopia, far-sightedness) is the refractive condition in which parallel light from infinity would, if unimpeded, focus at a point POSTERIOR to the retina in the unaccommodated eye. The far point of a hypermetropic eye is a virtual point behind the eye — at a negative distance. This is the fundamental optical distinction from myopia: in myopia the focal point is in front of the retina (too much power or too long an eye); in hypermetropia the focal point would be behind the retina (too little power or too short an eye). In contrast to myopia, the hypermetropic patient can often compensate for the error by using their accommodation (ciliary muscle contraction, which steepens the lens and adds refracting power), but this compensation comes at the cost of sustained accommodative effort and fatigue (asthenopia). The younger and more accommodatively powerful the patient, the greater the degree of hypermetropia that can be held latent — invisible even on non-cycloplegic refraction — while the older patient or one with high hypermetropia cannot compensate fully and presents with frank blurring. This interplay between accommodation and hypermetropia is unique to this refractive error and has major clinical consequences for diagnosis and prescription.
Classification by cause:
• Axial hypermetropia (commonest): reduced axial length (shorter than normal ~23 mm eye)
• Refractive hypermetropia: reduced refracting power — flat cornea, aphakia (absent lens — maximum hypermetropia, ~+10–14 D), or paralysis of accommodation
Classification by degree:
• Low: up to +2.00 D
• Moderate: +2.00 to +5.00 D
• High: >+5.00 D
Latent vs Manifest hypermetropia: A young patient with active accommodation can hold some hypermetropia latent — the ciliary muscle constantly contracts to compensate, and the eye appears emmetropic on non-cycloplegic refraction. The total hypermetropia = latent (corrected by accommodation, revealed only with cycloplegia) + manifest hypermetropia (cannot be overcome by accommodation — present on standard refraction). This distinction matters clinically: prescribing only for manifest hypermetropia may under-correct the patient, particularly in children where cycloplegic refraction (with atropine or cyclopentolate) is essential.
Clinical features: Unlike myopic patients (who often present with distance blur), hypermetropic patients — especially younger individuals — may have normal or near-normal visual acuity because accommodation compensates. They present with asthenopia (eye strain, frontal headaches, blurring after prolonged near work), convergent squint (esotropia) in children (because the excessive accommodative effort drives accommodative convergence), and in older patients or high hypermetropes, frank distance blur as accommodation becomes inadequate.
Correction: hypermetropia is corrected with a convex (converging, plus) lens.