Page 16 of 32
OP10.5 | Enucleation, Evisceration and Exenteration Indications — SDL Guide
Learning Objectives
- Distinguish evisceration, enucleation, and exenteration by the anatomical extent of tissue removed
- List the indications for evisceration and its contraindications
- List the indications for enucleation, including the sympathetic ophthalmia prevention rule
- List the indications for exenteration, including orbital malignancy and mucormycosis
- Describe the investigation sequence before each procedure
- Explain the cosmetic rehabilitation options (ocular and orbital prosthesis) available to patients
INSTRUCTIONS
Enucleation, evisceration, and exenteration are surgical procedures that involve removal of the eye or orbital contents. While they are performed by specialists, every doctor must know when each is indicated — particularly because delaying enucleation in intraocular tumours, or evisceration in uncontrolled endophthalmitis, can cost a life (tumour metastasis) or cost the remaining eye (sympathetic ophthalmia). This SDL covers the key indications and the clinical decision logic.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 21 (Intraocular tumours) and Ch. 23 (Orbit) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 30 (Injuries) and Ch. 31 (Operations on the globe) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old child is brought to the eye clinic with a white pupillary reflex (leukocoria) in the right eye, noted by the parents in photographs. Examination reveals a large white retinal mass and the eye is blind. The paediatric oncologist confirms retinoblastoma on ultrasound and MRI — no extraocular extension. He recommends removing the eye. The parents ask: 'But can't you just do an operation and take out the tumour? Why must you remove the whole eye?' And separately, a 65-year-old diabetic presents with a painful red eye that has been blind for years — his orbit now bulges and the eye feels soft. The ophthalmologist says, 'We need to remove the eye contents.' Is this the same operation as the child's? What is the difference — and which procedure fits which patient?
WHY THIS MATTERS
Surgeries that remove the eye or its contents are among the most psychologically significant operations in ophthalmology. As a future physician, you will encounter three situations where these procedures are relevant: when an intraocular malignancy requires enucleation for cure; when an infected or painful blind eye requires evisceration; and when orbital malignancy or uncontrolled fungal infection requires exenteration as a life-saving measure. Understanding the indications — and the critical contraindications (such as not performing evisceration on a suspected tumour) — prevents error and guides timely referral.
RECALL
Recall the basic orbital anatomy: the eye (globe) sits within the bony orbit, enclosed in a fibrous capsule called Tenon's capsule. The six extraocular muscles attach to the globe through Tenon's fascia. The optic nerve runs posteriorly from the globe through the orbital fat to the optic canal. The eyelids form the anterior protection of the orbit. From immunology, recall that the eye is an immunologically privileged site — antigens sequestered in the uveal tissue normally do not encounter the systemic immune system. Penetrating trauma can expose these antigens, triggering an autoimmune response in the opposite (sympathising) eye — the basis of sympathetic ophthalmia, which is one of the key indications for enucleation within the critical time window.
Clinical Presentation: When Is Eye Removal Considered?
The clinical presentations that lead to consideration of eye removal procedures fall into three broad categories: blind painful eye, intraocular or orbital malignancy, and uncontrolled orbital infection. Recognising these presentations and knowing which procedure to recommend (or refer for) is the core clinical skill this SDL develops.
Blind painful eye (phthisis bulbi or chronic endophthalmitis): A phthisical eye is a blind, shrunken, disorganised globe that has undergone calcification and scarring from end-stage disease (trauma, infection, or vascular occlusion). Although the eye is no longer functional, it may cause chronic pain from traction on ciliary nerves, secondary to calcified deposits, or from raised or fluctuating intraocular pressure. Similarly, an eye that has undergone panophthalmitis (total purulent intraocular infection) may be left as a blind, painful, hypotonic globe. These eyes are candidates for surgical removal — specifically evisceration if no tumour is suspected.
Intraocular malignancy: The classic example is retinoblastoma in a young child — the leading intraocular malignancy of childhood. When retinoblastoma is advanced (occupying more than half the vitreous, with neovascular glaucoma or opaque media, and no visual potential — IIRC Group D or E), enucleation is the treatment of choice for the affected eye. Choroidal melanoma in adults is another intraocular malignancy that may require enucleation. These eyes MUST NOT be eviserated — removing only the intraocular contents and leaving the sclera risks leaving viable tumour cells in the scleral tissue or seeding them into the orbit.
Orbital malignancy or extensive orbital invasion: When a malignant tumour has extensively infiltrated the orbital contents and cannot be managed by any less radical approach, exenteration is considered. This includes orbital invasion by periocular squamous cell carcinoma, adenoid cystic carcinoma of the lacrimal gland, malignant melanoma of the conjunctiva extending into the orbit, and rhabdomyosarcoma not responsive to other modalities.
Uncontrolled orbital mucormycosis: In immunocompromised patients (uncontrolled diabetes mellitus, haematological malignancy on immunosuppression), mucormycosis (caused by the fungus Rhizopus or Mucor) can invade the orbit aggressively, spread along blood vessel walls, and track intracranially. When antifungal therapy (IV amphotericin B) and surgical debridement are insufficient to control the spread, emergency exenteration is performed as a life-saving measure to prevent fatal intracranial extension.
Prevention of sympathetic ophthalmia: Following a severe penetrating injury to one eye that leaves it blind and disorganised, enucleation of the injured eye within 10–14 days prevents the development of sympathetic ophthalmia in the fellow (sympathising) eye.
Anatomy and Pathophysiology: What Each Procedure Removes
The three procedures differ fundamentally in the anatomical extent of tissue removed. Understanding this is the key to understanding the indications — each procedure is matched to the clinical requirement: the minimum necessary sacrifice to achieve the surgical goal.
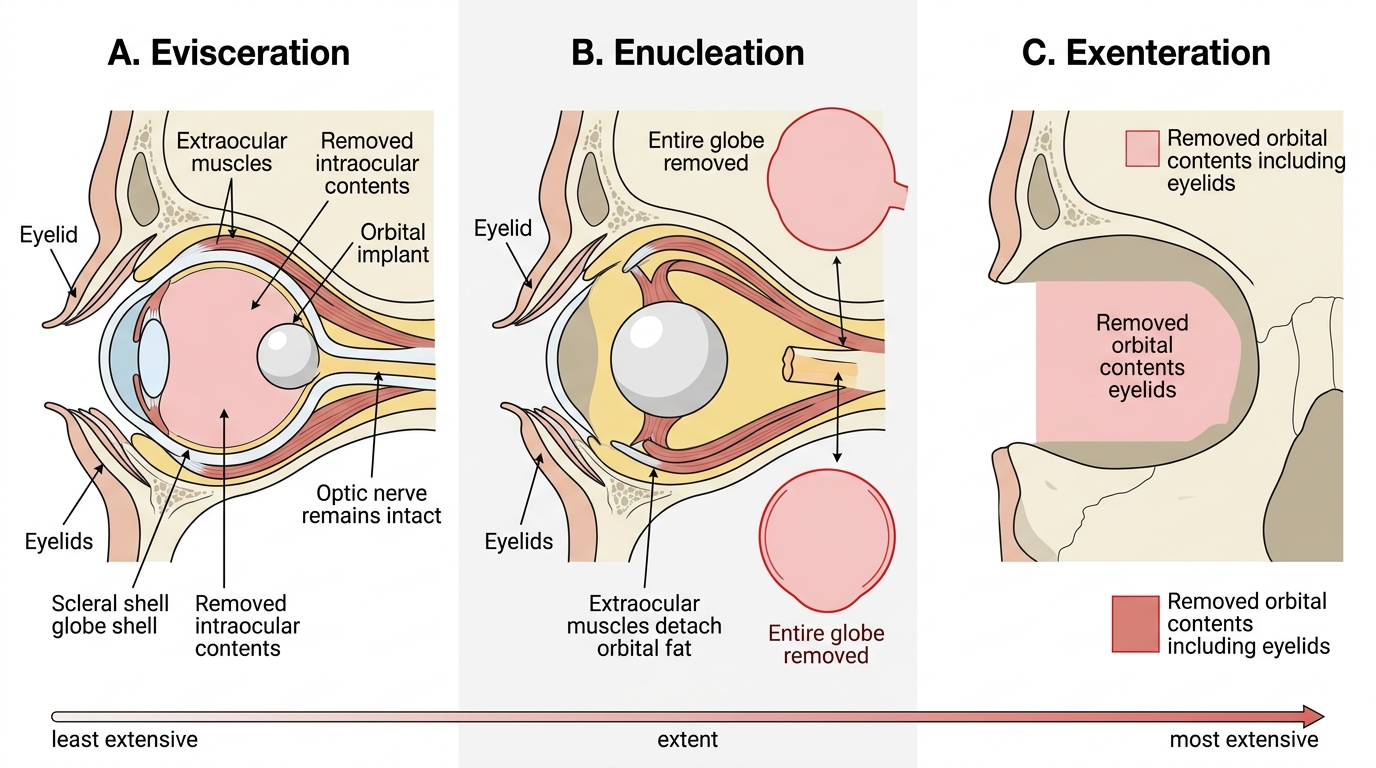
Evisceration removes the INTRAOCULAR CONTENTS — the uveal tract (iris, ciliary body, choroid), retina, lens, and vitreous humour — while leaving the scleral shell, the optic nerve (still attached to the sclera), and Tenon's capsule intact. A spherical orbital implant (typically hydroxyapatite or acrylic) is placed inside the empty scleral shell to maintain orbital volume. Because the sclera, optic nerve, and extraocular muscles are preserved, the resultant socket has some degree of residual motility, and the cosmetic result (with a custom-fitted ocular prosthesis over the implant) is often superior to enucleation. Additionally, proprioceptive fibres in the ciliary nerves may remain partially functional, giving the patient a vague proprioceptive sensation from the socket.
Enucleation removes the ENTIRE GLOBE — cornea, sclera, and all intraocular contents — by dividing the extraocular muscles from the globe, dividing the optic nerve, and removing the globe with its contained contents. A spherical orbital implant is placed in Tenon's capsule, and the extraocular muscles are reattached to the implant to restore socket motility. An ocular prosthesis (custom-made acrylic shell) is then fitted over the implant 6–8 weeks postoperatively. Because the sclera is removed along with the globe, there is no risk of leaving viable tumour tissue in a scleral remnant.
Exenteration removes the ENTIRE ORBITAL CONTENTS — the globe, all six extraocular muscles, orbital fat, lacrimal gland, and in most cases the eyelids (total exenteration) or at least the conjunctival lining. Periosteum may or may not be sacrificed depending on bony involvement. The resulting orbital cavity is large and requires reconstruction with a split-skin graft, temporalis muscle flap, or radial forearm flap. Cosmetic rehabilitation with an orbital prosthesis (often adhesive or held by osseointegrated implants) provides some degree of social acceptability but is far more conspicuous than an ocular prosthesis after enucleation.
Surgical Extent: Evisceration vs Enucleation vs Exenteration
Evisceration: Indications and Contraindications
Evisceration is the preferred procedure when the goal is removal of a blind, painful globe while preserving as much orbital tissue as possible for cosmetic and socket rehabilitation purposes. Understanding why evisceration is preferred over enucleation for benign blind painful eyes — when no tumour is present — requires appreciating the anatomical consequences of each operation. In evisceration, the scleral shell, the attached extraocular muscles, and the optic nerve all remain in the orbit. The spherical implant placed inside the scleral shell is therefore surrounded by the patient's own fibrovascular tissue, which grows into porous implants (hydroxyapatite) and allows the implant to integrate rather than migrate. Because the extraocular muscles remain attached to the sclera, they continue to transmit movement to the implant and ultimately to the overlying ocular prosthesis — producing a prosthetic eye that moves naturally in synchrony with the fellow eye, which is the gold standard of cosmetic rehabilitation. In contrast, enucleation removes the sclera and requires the muscles to be reattached to the implant directly, which achieves reasonable but generally slightly inferior motility. Additionally, the ciliary nerves in the sclera may retain some proprioceptive function, giving the patient a vague awareness of the socket position — contributing to comfort and patient satisfaction. However, the scleral remnant is a liability when a tumour might be present, which is why the absolute contraindication to evisceration is a suspected or confirmed intraocular malignancy. The key advantages are: better socket motility (sclera, muscles, and optic nerve preserved); reduced operative time; potentially lower risk of orbital fat atrophy compared to enucleation. The disadvantage is that the sclera and optic nerve remain in the orbit.
Indications for evisceration:
1. Blind painful eye from end-stage uveitis, phthisis bulbi, absolute glaucoma, or chronic retinal detachment — where no tumour is suspected.
2. Acute bacterial endophthalmitis — when the infection is overwhelming, the eye is perforated or destroyed, and the source of pain and infection must be eliminated. (Note: if the infection is suspected to have spread to the orbit, enucleation may be preferred over evisceration.)
3. Cosmetic improvement in a phthisical eye where the shrunken globe is disfiguring and uncomfortable.
Absolute contraindication for evisceration:
- Suspected or confirmed intraocular tumour: Retinoblastoma, choroidal melanoma, or any malignancy. Evisceration leaves the scleral shell in the orbit. Tumour cells may permeate through emissary canals in the sclera into the orbital tissue — evisceration can seed the orbit with malignant cells and dramatically worsen the prognosis. If any suspicion of intraocular malignancy exists, perform enucleation, not evisceration. A preoperative ultrasound B-scan to exclude a solid intraocular mass is mandatory before proceeding with evisceration.