Page 18 of 32
OP10.5 | Enucleation, Evisceration and Exenteration Indications — SDL Guide (Part 3)
Decision Algorithm: Choosing Between Evisceration, Enucleation, and Exenteration
A practical decision framework prevents the most dangerous error — eviscerating an eye that harbours a tumour. The decision tree distils the preceding clinical knowledge into an actionable sequence that can be applied at the bedside or in a viva examination. The framework works by asking a series of binary questions that progressively narrow the procedure choice, moving from the most critical safety question (is there a tumour?) through anatomical extent (is the disease confined to the globe or has it spread?) to specific disease category (orbital primary or fungal invasion?). Each branch of the tree has a single correct procedure choice, and the reasoning is always mechanistic — not a memorised rule but a consequence of the anatomy of tumour spread and the extent of tissue each procedure removes. Internalising this reasoning, rather than memorising 'retinoblastoma = enucleation' without understanding why, provides the resilience to handle unusual presentations correctly: a student who understands that evisceration is dangerous in any intraocular tumour because scleral emissary canals allow tumour seeding will correctly refuse to eviscerate even an unusual intraocular tumour they have not seen before. The decision tree is essentially:
Provided image
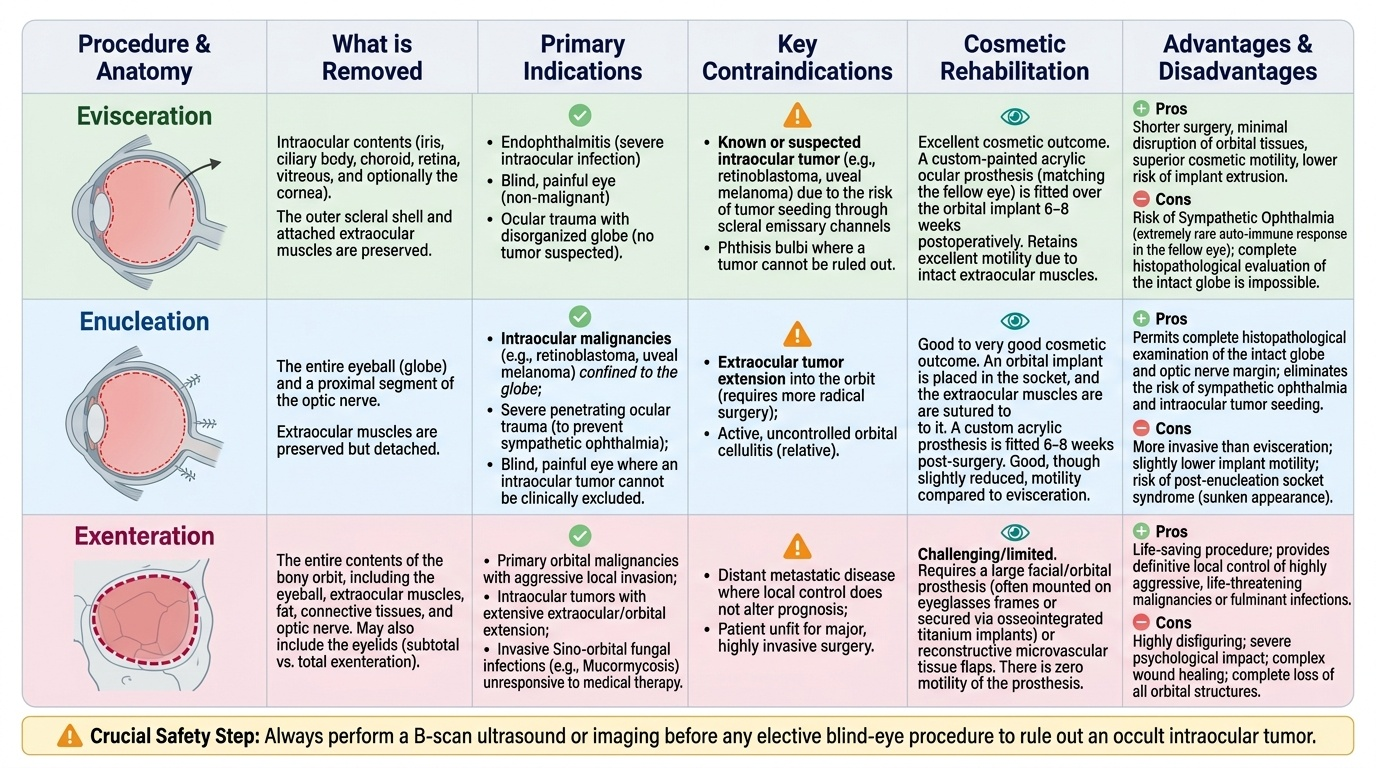
Step 1: Is an intraocular tumour present or suspected?
- If YES → Enucleation (NOT evisceration). B-scan before any procedure.
- If NO → Evisceration is acceptable for blind painful globe.
Step 2: Is the disease confined to the globe, or has it spread to the orbit?
- Confined to globe → Enucleation.
- Orbital invasion (soft tissue, muscles, bone) → Exenteration required.
Step 3: Is this an orbital primary tumour or fungal invasion?
- Orbital malignancy (primary or invasive) → Exenteration ± adjuvant therapy.
- Mucormycosis not responding to antifungals → Emergency exenteration.
Cosmetic rehabilitation: After evisceration or enucleation, a custom-fitted ocular prosthesis (a painted acrylic shell matching the colour and appearance of the fellow eye) is fitted 6–8 weeks postoperatively. Modern prosthetics are highly realistic and can be matched precisely. Patients can swim, shower, and sleep with the prosthesis in place. After exenteration, an orbital prosthesis (adhesive or magnetically retained) covers the orbital socket; these are more conspicuous but acceptable to many patients.
Sympathetic ophthalmia prevention timing: The most important management rule is that after a penetrating injury that destroys one eye, if the injured eye has no visual potential, enucleation should be performed within 10–14 days of the injury. Once sympathetic ophthalmia has developed in the fellow eye, enucleation no longer cures the condition — it may reduce the inflammatory stimulus but systemic corticosteroids and/or immunosuppressants are required. The safe window for preventive enucleation is approximately the first two weeks.
CLINICAL PEARL
The B-scan before evisceration rule: Never perform evisceration without first doing a B-scan ultrasound of the eye to exclude an intraocular solid mass. A phthisical eye that is soft, shrunken, and opaque may contain a choroidal melanoma that has outgrown its blood supply and appears clinically as a 'burnt-out' blind eye. If you eviscerate such an eye, you leave viable melanoma cells in the scleral shell and seed them into the orbit. Enucleation in this scenario could have been curative. The B-scan takes 5 minutes and costs almost nothing — skip it only in an obvious perforated eye with no media to examine, and even then document your reasoning.
Self-Assessment: Indications Review
Work through these scenarios and confirm the correct procedure and key reasoning before your OSCE or viva. The five scenarios below are drawn directly from the pattern of questions asked in MBBS ophthalmology professional examinations across Indian universities and reflect the clinical situations that general physicians and district hospital doctors are most likely to encounter. For each scenario, your answer should state not only the correct procedure but also the primary reasoning that justifies it — examiners at the MBBS level specifically reward candidates who explain why a procedure is correct or contraindicated, not merely which procedure to choose. The most frequently failed scenario is the retinoblastoma question: students who have not consolidated the 'evisceration is absolutely contraindicated in intraocular tumour' rule sometimes hedge with 'evisceration or enucleation depending on the surgeon's preference' — this answer is incorrect and potentially dangerous. The second most failed scenario is the sympathetic ophthalmia timing question: students know enucleation is indicated but cannot state the 10–14 day window, which is the critical prognostic detail. Work through each scenario, state your answer, and check it against the key reasoning provided.
- A 6-year-old with confirmed retinoblastoma (IIRC Group E) in the right eye, no extraocular spread on MRI. → Enucleation (evisceration contraindicated — intraocular tumour).
- A 70-year-old with a blind, painful right eye from a phthisical globe after a remote retinal detachment. B-scan shows no solid intraocular mass, only calcified deposits. → Evisceration (no tumour; blind painful eye).
- A 60-year-old diabetic in a DKA with a black necrotic palate, proptosis, and failed 72 hours of IV amphotericin B. → Emergency exenteration (orbital mucormycosis with failing antifungal therapy; life-saving).
- A 35-year-old sustains a penetrating injury to the left eye in a road accident — the eye is totally destroyed, with no light perception. Three days post-injury. → Enucleation within 10–14 days to prevent sympathetic ophthalmia in the right eye.
- A 50-year-old has a large conjunctival melanoma that on MRI has invaded the orbital fat. → Exenteration (orbital invasion by malignancy).
SELF-CHECK
A 40-year-old sustains a severe penetrating injury to the left eye, leaving it totally blind and disorganised. It is now day 8 post-injury. The right eye is currently normal. What is the indication and timing for surgical removal of the left eye to protect the right eye?
A. No surgical indication — the right eye is normal; observe the left eye
B. Evisceration now — removes infected tissue and prevents uveitis
C. Enucleation of the left eye within 10–14 days of the injury — to prevent sympathetic ophthalmia in the right eye
D. Enucleation only after sympathetic ophthalmia develops in the right eye
Reveal Answer
Answer: C. Enucleation of the left eye within 10–14 days of the injury — to prevent sympathetic ophthalmia in the right eye
Enucleation of the injured (exciting) eye within 10–14 days of a severe penetrating injury is the accepted window for preventing sympathetic ophthalmia in the fellow (sympathising) eye. Day 8 is within this window — enucleation should be performed. Once sympathetic ophthalmia has established itself in the right eye, enucleation of the left eye no longer cures it. Evisceration is not the procedure of choice here because it is important to remove the source of uveal antigen (the globe) completely via enucleation, and the clinical status of the injured eye cannot exclude an intraocular tumour without histology.