Page 20 of 32
OP10.6 | Ocular Injuries: Classification, Primary Management and Referral — SDL Guide
Learning Objectives
- Classify ocular injuries as closed globe, open globe, chemical burn, or radiation injury
- Describe the mechanism by which alkali burns cause deeper and more severe damage than acid burns
- State that immediate copious irrigation is the first priority for chemical ocular burns, preceding examination or referral
- Enumerate the examination steps and the 'do-nots' in managing an open globe injury
- List the clinical findings in blunt (closed globe) trauma including hyphaema, commotio retinae, and orbital blow-out fracture
- State the indications for urgent referral for each injury type
INSTRUCTIONS
Ocular injuries are a common cause of preventable visual impairment, particularly in industrial workers, agricultural workers, and children. As the first-contact doctor in a casualty or primary care setting, you may be the most important person in preventing permanent vision loss — the first 5–10 minutes of management of a chemical eye burn can determine whether the patient retains vision. This SDL covers the classification, recognition, first-line management, and referral decisions for all major categories of ocular injury.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 16 (Injuries to the eye) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 30 (Injuries to the eye) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM at the district hospital casualty. A 28-year-old construction worker rushes in with his hands over his eyes, screaming in pain. His co-worker explains that a bag of lime (calcium hydroxide — an alkali) burst and splashed into his face about 15 minutes ago. The casualty nurse starts to prepare to take the patient's history and vitals. You enter the room. What is the SINGLE most important first action? Hint: it is not taking the history, it is not calling the ophthalmologist, and it is not examining the eye. What is it?
WHY THIS MATTERS
Ocular trauma accounts for up to 3% of all emergency department visits and is a leading cause of monocular blindness in working-age adults in India. Chemical burns — particularly with alkali substances common in construction, agriculture, and domestic accidents — are ophthalmic emergencies where the first 60 seconds of management by ANY healthcare worker (including a nurse, a general physician, or even a bystander) determines the visual outcome. An open globe injury that is inappropriately squeezed or probed loses vitreous and lens contents, worsening the prognosis irreversibly. This SDL empowers you to act correctly in the first few minutes — and to refer appropriately for specialist care.
RECALL
Recall the anatomy of the anterior segment: the cornea is the transparent avascular anterior window of the eye, covered by the tear film and non-keratinised epithelium. The conjunctiva lines the inner eyelids and covers the anterior sclera — it contains goblet cells and blood vessels. The anterior chamber contains aqueous humour between the cornea and the lens/iris. The sclera is the tough fibrous outer coat of the eye. From chemistry, recall that alkalis (strong bases — NaOH, KOH, calcium hydroxide/lime, ammonia) react with fatty acids in cell membranes by saponification and with proteins by denaturation, producing a liquefactive, penetrating, spreading injury. Acids (sulphuric, hydrochloric) coagulate proteins — this coagulation creates a barrier of denatured protein that limits further penetration. The pH of neutral water is 7; physiological ocular pH is approximately 7.2–7.4.
Presentation: The Patient with an Injured Eye
The history of mechanism is the most important piece of information in managing an ocular injury, because the mechanism determines the injury type and the urgency of response. However, in chemical burns, do not let taking the history delay irrigation — start irrigation immediately and take the history while irrigating. The key history points for any ocular injury are: What happened? When? What substance was involved? What was the size, speed, and direction of impact? Was protective eyewear worn? Is there a foreign body sensation (suggests corneal/conjunctival foreign body)? What treatment, if any, has already been given?
The presenting complaints vary by injury type. Sudden severe pain and photophobia suggest corneal epithelial disruption — as in chemical burns (caustic pain), corneal foreign body, corneal abrasion, or photokeratitis (welder's flash). Gradual painless visual loss after blunt trauma suggests commotio retinae, vitreous haemorrhage, or retinal detachment — all of which may have a delayed presentation (the patient may not notice the vision loss until hours after the injury). A history of hammering metal on metal ('metallic foreign body' presentation) should immediately raise suspicion of an intraocular foreign body (IOFB) — these patients often have minimal pain and surprisingly good vision at presentation, because a tiny high-velocity IOFB enters the eye through a small self-sealing wound. Failure to take a careful history in this setting leads to missed IFOBs with devastating delayed consequences (siderosis from iron, chalcosis from copper).
Chemical splash to the eye is the most time-critical presentation. The patient may be hysterical, holding their eyes closed, refusing to open them due to pain and blepharospasm. Do not waste time — forcibly open the eyelids if necessary and start copious irrigation immediately. The substance matters: lime (calcium hydroxide), cement, oven cleaner, dishwasher detergent, and bleach are common alkalis in the Indian setting. Battery acid (sulphuric acid) is the most common acid injury.
Classification of Ocular Injuries: Closed vs Open Globe and Chemical Burns
The Birmingham Eye Trauma Terminology (BETT) system provides a standardised classification of mechanical ocular injuries based on whether the full thickness of the sclera and cornea (the wall of the eye) is breached. A clear, universally agreed classification matters enormously in ocular trauma because the management of a closed globe injury and an open globe injury are fundamentally different — and applying the wrong management to an open globe (for example, applying a pressure pad, squeezing the eyelids, or instilling eye drops) can catastrophically worsen the outcome by extruding intraocular contents through the wound. Before BETT was adopted, different hospitals and countries used inconsistent terminology, making it impossible to compare outcomes data or develop evidence-based protocols. The BETT system is now the international standard and its terminology is used in all major ophthalmology trauma registries, including the United States Eye Injury Registry and the Birmingham Eye Trauma Terminology Society database. Understanding the classification also structures your examination: for every injured eye, your first clinical question should be 'is this an open globe or a closed globe?' — because the answer to that question determines every subsequent management decision, from whether to apply a shield or a pad, to whether to perform tonometry, to whether to instil anaesthetic drops, to the urgency and nature of the specialist referral.
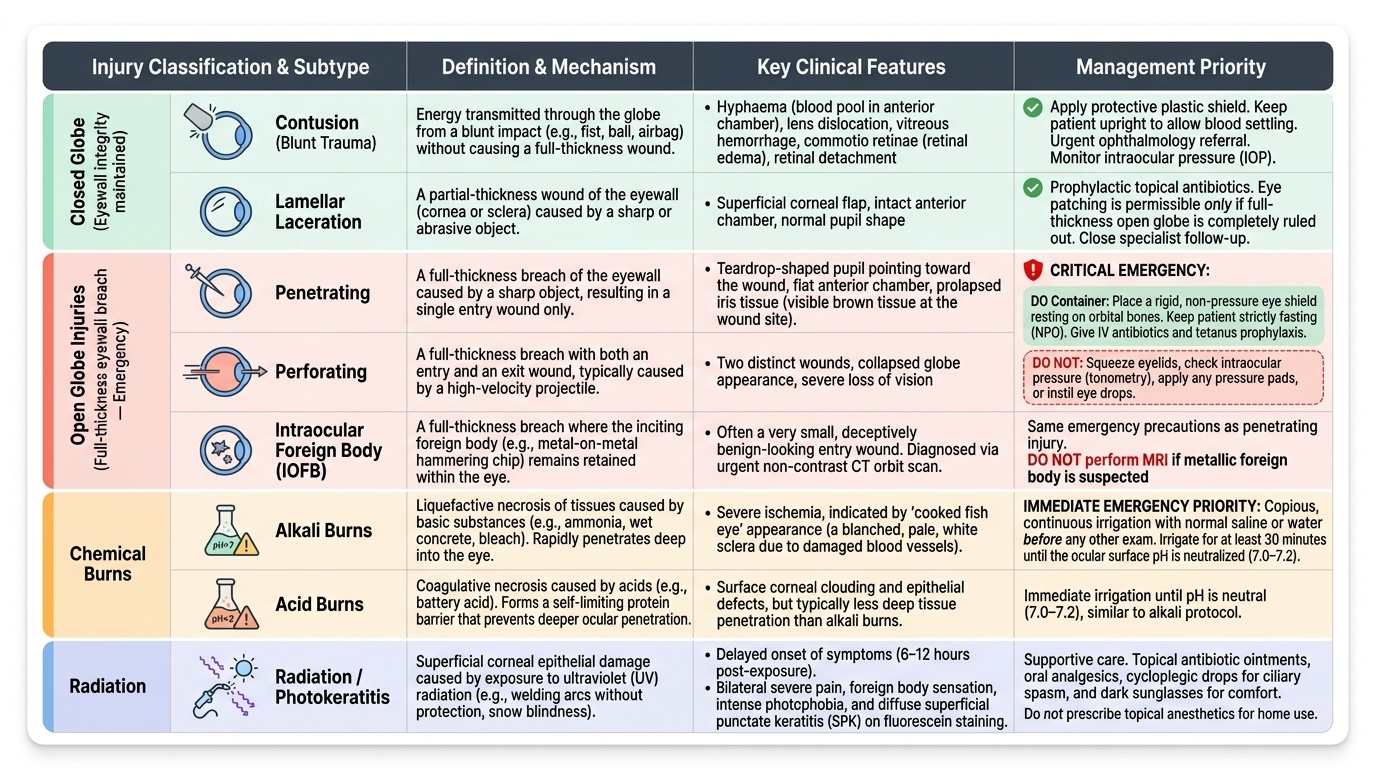
Provided image
Closed globe injuries: The eyewall integrity is maintained. The full thickness of the cornea and sclera is intact, but significant intraocular damage may occur. Two subtypes:
- Contusion (blunt trauma): Energy transmitted through the globe causes intraocular damage without any wound — hyphaema (blood in the anterior chamber), lens dislocation, vitreous haemorrhage, commotio retinae (retinal oedema), choroidal rupture, retinal detachment, or optic nerve injury.
- Lamellar (partial-thickness) laceration: A wound that does not penetrate the full thickness of the eyewall — partial-thickness corneal laceration or scleral laceration.
Open globe injuries: The full thickness of the eyewall is breached. Two mechanisms:
- Penetrating injury: A single wound — entry only. A sharp object (knife, glass, metal fragment) enters the eye through the cornea or sclera.
- Perforating injury: Entry AND exit wounds — the object passes through the eye completely.
- Intraocular foreign body (IOFB): A retained object inside the globe following penetration. High-velocity metallic fragments (hammering metal on metal; grinding) are the classic cause. The entry wound may be small and self-sealing, making the injury easy to miss.
Chemical burns: Classified separately from mechanical injuries. The most important distinction is between alkali and acid, which differ fundamentally in their penetration depth and therefore severity.
Radiation injuries: Ultraviolet keratitis (photokeratitis — 'welder's flash' or 'snow blindness') from UV exposure causes delayed (6–8 hours post-exposure) severe ocular pain and photophobia; corneal epithelium is disrupted. Infrared radiation (glassblower's cataract) causes chronic lens opacification. Laser injuries affect the retina. Ionising radiation causes cataract, keratoconjunctivitis sicca, and retinal vascular occlusion.
Primary Examination of the Injured Eye
The examination of an injured eye must be adapted to the type of injury suspected. In a chemical burn, irrigation precedes examination. In all other injuries, a structured examination determines the injury type and guides management. A crucial concept: in a suspected open globe injury, certain examination manoeuvres are dangerous and must be AVOIDED. The reason that open globe examination requires such careful modification is mechanical: the intraocular pressure in a normal eye is maintained at 10–21 mmHg by the balance between aqueous production and drainage. When the eyewall is breached, this pressure gradient is abolished and the eye is in communication with atmospheric pressure. Any external force applied to the globe — the weight of an eyelid, the pressure of an examiner's fingers, the tip of an applanation tonometer, or even the patient squeezing their eyes shut in pain — can cause an acute rise in intraocular pressure that forces vitreous, iris, lens, and even retina through the wound opening. This extrusion of intraocular contents dramatically worsens the surgical and visual prognosis. It is for this reason that the first-contact management of any suspected open globe prioritises a rigid Fox shield (which rests on the orbital rim, not on the globe) over a pressure pad, and avoids any examination technique that requires contact with or compression of the globe. A seemingly thorough examination that inadvertently extrudes intraocular contents causes more harm than a brief, careful assessment that establishes the diagnosis and arranges safe transfer.
What to examine:
1. Visual acuity: Record acuity in each eye with the patient's best current correction. Even in an emergency, visual acuity at presentation is a medico-legal document and a prognostic baseline. A patient with light perception only after blunt trauma has a different prognosis from one with 6/12.
2. Pupil: Check for a direct and consensual response. An afferent pupillary defect (Marcus Gunn pupil — the swinging flashlight test) in the injured eye suggests significant posterior segment or optic nerve injury. A dilated fixed pupil in a traumatised eye may indicate iris sphincter rupture (from blunt trauma), posterior synechiae, or CN III palsy.
3. Anterior segment examination with a slit lamp or loupe + torch: Look for: corneal abrasion (fluorescein staining), corneal laceration or perforation, hyphaema (blood level in the anterior chamber), lens opacity or dislocation, foreign body (on the cornea, conjunctival fornices, or embedded in the stroma). Always evert the upper eyelid to sweep for subtarsal foreign bodies — the commonest cause of persistent foreign body sensation after apparently normal examination.
4. Seidel test (for open globe): A strip of fluorescein-impregnated paper applied to the suspected wound site: if aqueous leaks through the wound, the fluorescein is diluted and appears as a streaming green flow against the orange fluorescein background. A positive Seidel test = open globe.
5. Posterior segment: Dilated fundus examination for commotio retinae, vitreous haemorrhage, retinal tears, choroidal rupture, IOFB, or retinal detachment. If media is opaque (hyphaema, vitreous haemorrhage), B-scan ultrasound is used.
What NOT to do in a suspected open globe:
- Do NOT apply a pad or pressure dressing (increases intraocular pressure → extrudes vitreous and uveal contents).
- Do NOT instil any eye drops if the eye is perforated (toxic to intraocular structures).
- Do NOT attempt to remove an obviously impaled foreign body.
- Do NOT perform tonometry (the pressure probe can cause extrusion of contents).
- Instead: apply a Fox protective shield (rigid shield that rests on the orbital rim without touching the eye), keep the patient nil by mouth (for surgery), give IV antibiotics, tetanus prophylaxis, and arrange urgent ophthalmology referral for surgical repair.