Page 12 of 32
OP10.4 | Vitamin A Deficiency: Ocular Manifestations, Management and Referral — SDL Guide
Learning Objectives
- Describe the role of vitamin A in rhodopsin synthesis and mucosal epithelial integrity
- List the WHO stages of xerophthalmia in correct sequence (XN through XF) with their clinical findings
- Identify Bitot's spots correctly as a conjunctival (X1B) manifestation, not a corneal one
- Enumerate the systemic causes of vitamin A deficiency including dietary, malabsorptive, and precipitating factors
- State the WHO oral vitamin A treatment protocol and the doses by age group
- Specify which xerophthalmia stages require urgent ophthalmic referral
INSTRUCTIONS
Vitamin A deficiency remains the leading cause of preventable childhood blindness worldwide, and India still carries a significant burden despite national supplementation programmes. As a doctor, you need to recognise xerophthalmia in its early stages — when treatment prevents blindness — and refer urgently when corneal involvement threatens sight. This module covers the classification, examination findings, management, and prevention of vitamin A deficiency eye disease.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 5 (Conjunctiva) and Ch. 12 (Nutritional and metabolic disorders) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 7 (Nutritional and metabolic diseases of the eye) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A community health worker brings a 3-year-old girl to the primary health centre. The child's mother reports that the child cannot see in dim light and keeps bumping into objects after sunset. The child is thin and pale. On examination, you note dry, lusterless conjunctivae and a triangular foamy white deposit on the temporal side of each eye — visible as a white patch adjacent to the cornea. The corneas are clear and the child can see normally in daylight. The CHW asks: 'Is this serious? Do I need to send her to the district hospital?' What is the diagnosis? What is the stage? And what does this child need in the next 24 hours?
WHY THIS MATTERS
Vitamin A deficiency (VAD) is the leading cause of preventable childhood blindness in the world, responsible for an estimated 250,000 to 500,000 child blindings per year globally. India accounts for a disproportionate share of this burden. The disease is entirely preventable and largely reversible in early stages — but once keratomalacia (corneal melting) occurs, the damage is irreversible. Recognising xerophthalmia at the Bitot's spots stage (X1B) or even night blindness (XN) and initiating vitamin A supplementation immediately can prevent progression to corneal destruction. This is one of the few clinical situations where timely action by a first-contact provider directly prevents permanent blindness.
RECALL
Recall from your biochemistry and physiology learning that vitamin A (retinol) has two critical roles in the eye. First, it is the precursor of 11-cis retinal, which combines with the protein opsin to form rhodopsin — the visual pigment in rod photoreceptors responsible for dark-adapted (scotopic) vision. Depletion of vitamin A depletes rhodopsin and impairs rod function, causing the earliest symptom of deficiency: night blindness (nyctalopia). Second, vitamin A is essential for maintaining the normal mucosal epithelium of the conjunctiva and cornea by supporting goblet cell function. Goblet cells secrete mucin, which anchors the tear film to the ocular surface; without mucin, the tear film breaks up and the surface desiccates — leading to the dry, keratinised changes of xerophthalmia. Vitamin A is a fat-soluble vitamin absorbed in the small intestine and stored in the liver; deficiency occurs with inadequate dietary intake, fat malabsorption, or any condition that depletes liver stores (e.g. measles-associated hepatic damage).
Presentation: How Vitamin A Deficiency Comes to Attention
Vitamin A deficiency (VAD) comes to clinical attention through several different routes, all of which require prompt recognition. The most common early presentation in children is night blindness — parents notice that the child stumbles or becomes fearful in low light, cannot navigate after dark, and seems to lose vision at dusk while retaining normal daytime vision. In young infants who have not yet developed independent mobility, night blindness may be reported as excessive crying in the evening or apparent fear of dimly lit rooms. This symptom may predate any visible eye sign by weeks to months.
In the community setting, the presence of Bitot's spots — a distinctive white, foamy, triangular deposit on the temporal bulbar conjunctiva — is a clinical sign that brings the child to health facilities. Community health workers and anganwadi workers in India are trained to recognise this sign during nutritional surveys. In hospital settings, xerophthalmia is often encountered in severely malnourished children admitted for other reasons (severe acute malnutrition, measles, persistent diarrhoea), where it may coexist with multiple micronutrient deficiencies.
More severe presentations — corneal xerosis (dry, hazy cornea) and keratomalacia (corneal softening and melting) — occur in the context of profound nutritional deprivation and are frequently precipitated by an acute illness, most classically measles. The measles virus causes temporary severe vitamin A depletion even in well-nourished children, and in a child already marginally deficient, measles can trigger rapid progression from early xerophthalmia to keratomalacia within days. This is why vitamin A supplementation on days 1 and 2 of hospital admission for measles is standard WHO policy. In India, children living in areas with high rates of protein-energy malnutrition and a rice-based, low-fat diet are at highest risk.
Pathophysiology: Why Vitamin A Deficiency Damages the Eye
The two pathways through which vitamin A deficiency damages the eye — rod photoreceptor dysfunction and ocular surface epithelial breakdown — explain the entire clinical progression of xerophthalmia from night blindness to corneal blindness.
Rhodopsin depletion and night blindness: In the rod photoreceptors, 11-cis retinal (derived from dietary retinol) binds to the protein opsin to form rhodopsin. When light strikes the retina, rhodopsin absorbs a photon and undergoes isomerisation (11-cis to all-trans retinal), generating a nerve impulse. The all-trans retinal is recycled back to 11-cis retinal in the retinal pigment epithelium — a process that requires an ongoing supply of retinol from the circulation. When vitamin A stores are depleted, this recycling fails, rhodopsin levels fall, and rod photoreceptor function deteriorates. Rods are responsible for low-light (scotopic) vision; cones, which mediate colour and high-acuity vision, are less affected in early deficiency because they are more resistant and require less retinoid. Thus the earliest and most characteristic symptom is night blindness — loss of scotopic vision while photopic (daytime) vision is relatively preserved.
Goblet cell depletion and ocular surface keratinisation: Vitamin A is essential for the differentiation of the conjunctival epithelium into mucin-secreting goblet cells. In its absence, the normal columnar mucous epithelium undergoes squamous metaplasia — the conjunctival and corneal epithelial cells become flattened, keratinised, and lose their ability to secrete mucin. Without mucin, the aqueous tear film does not adhere to the ocular surface, the tear film breaks up rapidly (reduced tear break-up time), and the ocular surface desiccates. This leads to the dry, rough, non-wettable conjunctiva and cornea of xerophthalmia (Greek: xeros = dry, ophthalmos = eye).
As keratinisation progresses and the cornea is affected, the corneal epithelium loses its clarity and transparency, the stroma softens, and — in the most severe stage — the cornea literally melts (keratomalacia), often progressing to perforation, prolapse of intraocular contents, and total blindness within hours. This final pathway is irreversible; prevention or early treatment is the only option.
WHO Classification: Stages of Xerophthalmia
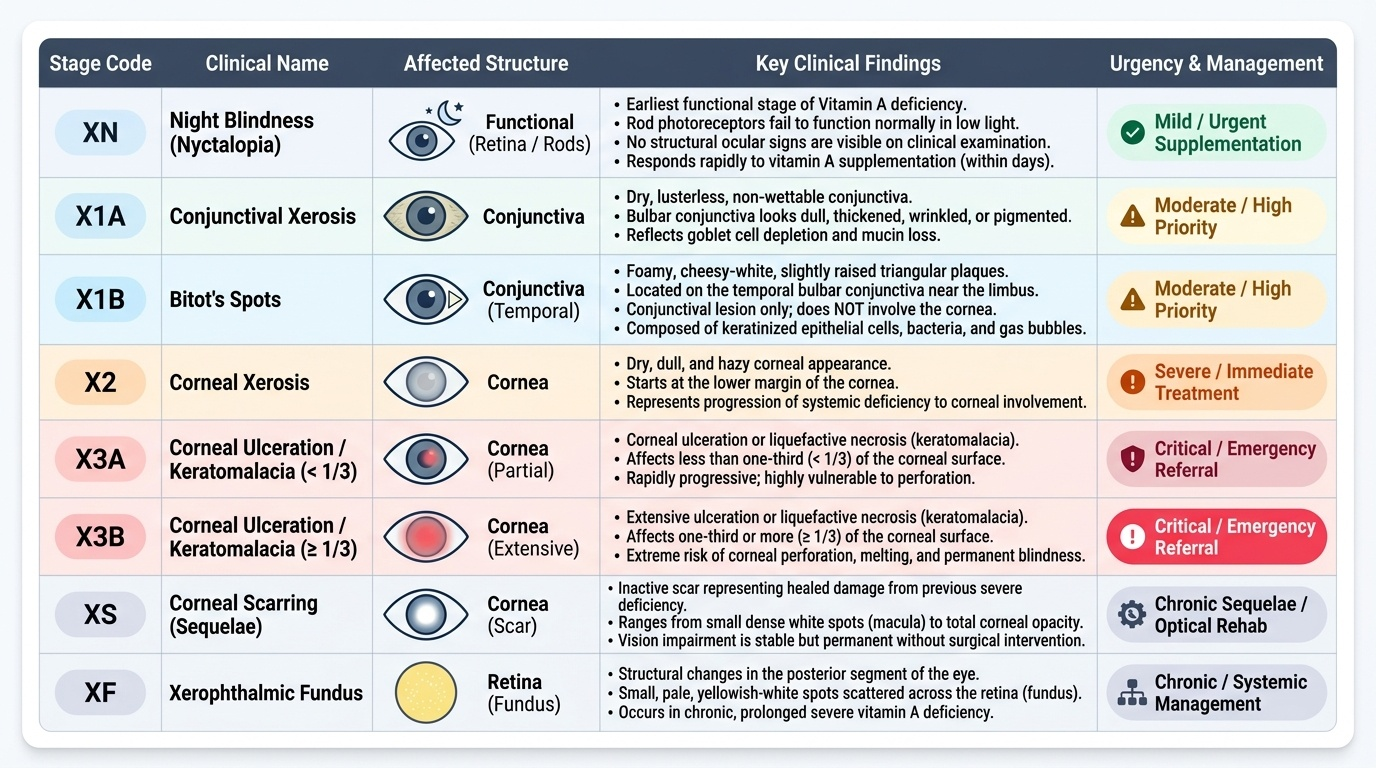
The WHO classification of xerophthalmia (1982, revised Sommer) provides a systematic staging system based on the anatomical site and severity of the lesion. The stages progress from pure functional impairment (night blindness) through conjunctival changes to corneal involvement of increasing severity, ending with the sequelae. The order must be memorised exactly — each stage indicates the degree of deficiency and guides management urgency.
Provided image
The stages in order are:
XN — Night blindness (nyctalopia): The earliest functional stage. Rod photoreceptors fail to function normally in low light. No structural ocular sign is visible on examination. The child cannot see in dim light. Responds rapidly to vitamin A supplementation (rhodopsin is regenerated within days).
X1A — Conjunctival xerosis: Dry, lusterless, non-wettable conjunctiva that lacks its normal glistening, moist appearance. The bulbar conjunctiva looks dull, somewhat thickened, and may have a wrinkled or pigmented appearance. The dryness reflects goblet cell depletion and mucin loss.
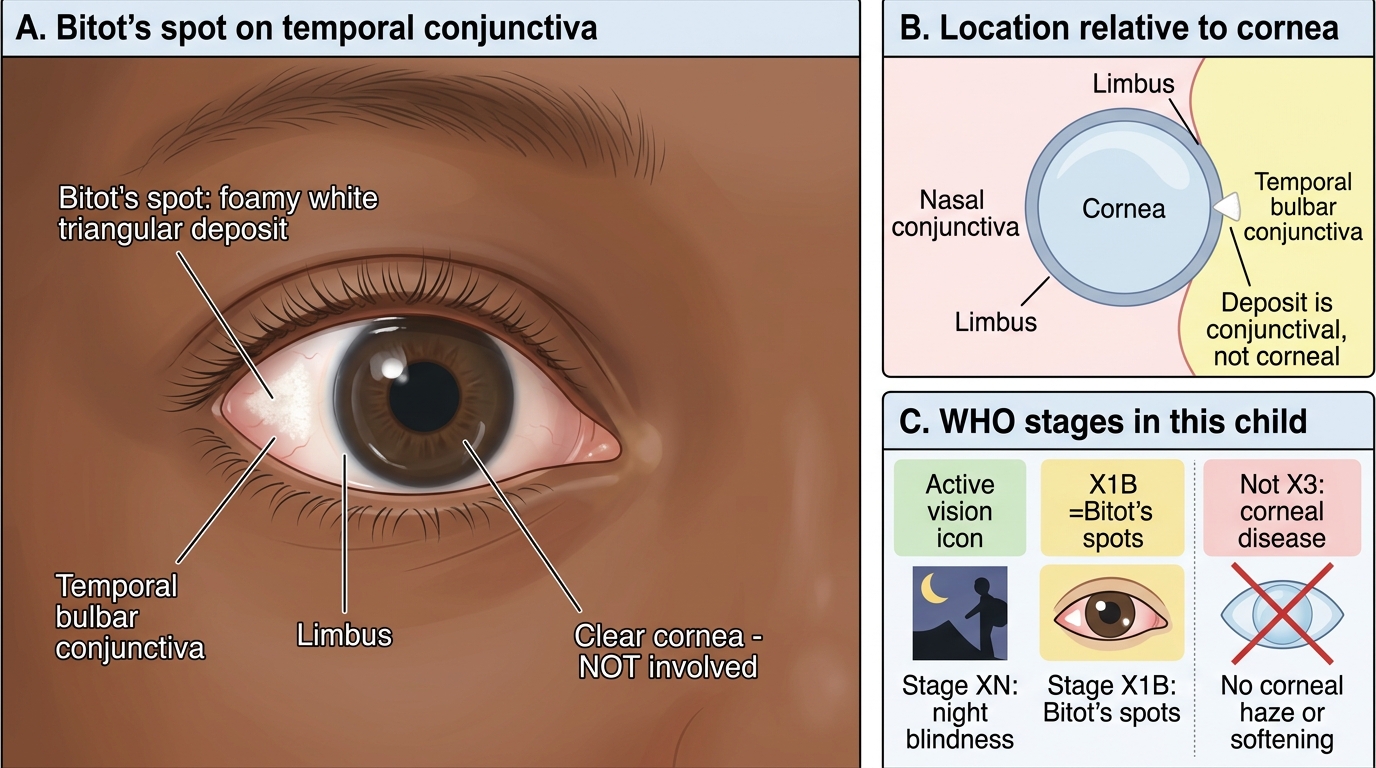
X1B — Bitot's spots (CONJUNCTIVAL lesion): Foamy, cheesy-white, slightly raised triangular plaques on the TEMPORAL bulbar conjunctiva adjacent to the limbus (the corneoscleral junction). Bitot's spots are a CONJUNCTIVAL lesion — they do NOT involve the cornea. They are composed of keratinised epithelial cells, bacteria (commonly Corynebacterium xerosis), and gas bubbles that give them their characteristic foamy appearance. They are pathognomonic of vitamin A deficiency in children in the appropriate demographic context (in adults, they may persist as inactive scarring after previous deficiency). They may also occur nasally, but temporal location is far more common. Bitot's spots do not cause permanent visual impairment on their own — but they are a marker of systemic deficiency severe enough to threaten the cornea.
X2 — Corneal xerosis: Now the cornea is involved. The cornea loses its normal mirror-like brilliance and becomes dry, hazy, and lusterless — with a ground-glass or orange-peel surface texture. This is the critical transition point — corneal involvement means the deficiency is severe enough to threaten permanent vision loss and warrants urgent referral and treatment.
X3A — Keratomalacia, less than 1/3 of the corneal area: Stromal softening and liquefactive necrosis involves LESS THAN one-third of the corneal area. The cornea appears soft, yellowish-white, and gelatinous. Progression to perforation is rapid without treatment.
X3B — Keratomalacia, 1/3 or more of the corneal area: Liquefactive necrosis involves ONE-THIRD OR MORE of the corneal area. This is the most devastating stage — it often progresses within hours to complete corneal destruction, perforation, endophthalmitis, and phthisis bulbi. Vision loss is catastrophic and usually total. EMERGENCY referral to tertiary ophthalmology.
XS — Corneal scar: Healed stage after previous keratomalacia. The cornea shows leucoma (dense white opacity), adherent leucoma, or phthisis (shrunken, non-functional globe). This stage is the permanent sequela of untreated severe xerophthalmia.
XF — Xerophthalmic fundus: Pale, mottled fundus due to photoreceptor (rod and cone) dysfunction from prolonged vitamin A deficiency. A relatively rare finding; associated with electroretinographic changes. May partially reverse with treatment.
Bitot's Spots: WHO Stage X1B
SELF-CHECK
A 4-year-old child has foamy white deposits on the temporal conjunctiva of both eyes but the corneas are clear and glistening. The child reports difficulty seeing at dusk. Which WHO xerophthalmia stages are present?
A. X1A and X2
B. X1B and XN
C. X2 and X3A
D. X1B and X2
Reveal Answer
Answer: B. X1B and XN
The foamy white deposits on the TEMPORAL CONJUNCTIVA are Bitot's spots — WHO stage X1B. The night blindness is stage XN. Clear corneas confirm there is NO corneal involvement (X2 would show corneal haze; X3 would show softening). This child has XN + X1B, which are both conjunctival/functional stages. The corneas are not yet involved, but urgent vitamin A supplementation is needed to prevent progression to corneal disease.