Page 9 of 27
OP3.3 | Chronic Conjunctivitis and Trachoma — SDL Guide (Part 2)
The WHO Simplified Grading System for Trachoma
The WHO simplified grading system was developed to enable community health workers without slit-lamp access to grade trachoma using a 2.5× loupe and a torch. It replaces the older MacCallan classification (stages I–IV) in current public health practice, though the MacCallan system may still appear in older textbooks. There are five grades — each is a binary yes/no sign, and a person can have more than one grade simultaneously. Understanding the grading system requires appreciating why it was designed the way it was: each grade corresponds to a distinct pathological stage and a distinct intervention target. TF and TI identify active infection and flag communities for antibiotic mass drug administration. TS identifies cumulative fibrotic damage that no antibiotic can reverse. TT identifies the mechanical lash-on-cornea abrasion that only surgery can stop. CO identifies irreversible visual loss — the endpoint that the entire SAFE strategy exists to prevent. Memorising the thresholds without understanding this logic leads to superficial recall that fails under application pressure.
The five grades must be memorised precisely, as the thresholds are specific:
TF — Trachomatous Inflammation-Follicular:
- ≥5 follicles, each ≥0.5 mm in diameter, in the central zone of the upper tarsal conjunctiva.
- Represents active infection with lymphoid follicle formation.
- Found in children 1–9 years in endemic communities.
- The 'central zone' is the area covering the central two-thirds of the upper tarsal plate — follicles at the periphery are less specific.
TI — Trachomatous Inflammation-Intense:
- Intense inflammatory thickening of the upper tarsal conjunctiva obscuring MORE than half of the deep tarsal blood vessels.
- Represents a heavy chlamydial infection load with abundant neutrophilic and lymphocytic infiltration.
- The most infectious grade — patients with TI shed the most chlamydiae.
TS — Trachomatous Scarring:
- Presence of scarring (white fibrous lines, bands, or sheets) on the upper tarsal conjunctiva.
- Arlt's line — the pathognomonic horizontal white line — is the classic form of TS.
- Represents healed, fibrotic disease — not currently active infection necessarily.
TT — Trachomatous Trichiasis:
- At least one eyelash touching the eyeball, OR evidence of recent epilation (lash removal) to relieve the trichiasis.
- Causes repeated corneal abrasion — the immediate precursor to corneal opacity.
- Requires surgical correction.
CO — Corneal Opacity:
- Easily visible corneal opacity over the pupil — dense enough to obscure at least part of the pupil margin.
- Represents the irreversible visual loss endpoint.
- Once CO is present and the visual axis is affected, visual recovery is only possible with corneal transplant (penetrating keratoplasty).
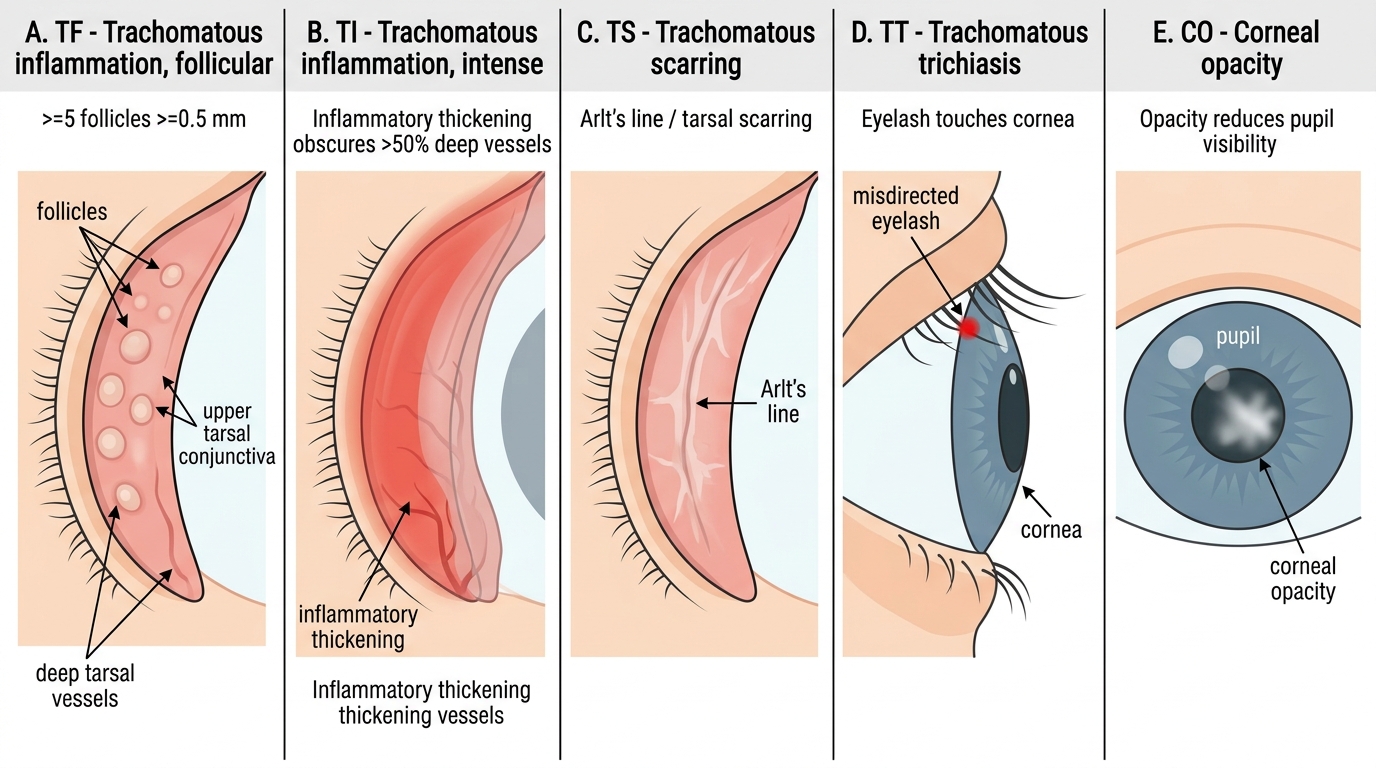
WHO Simplified Grading System for Trachoma
Examination technique:
Evert the upper eyelid using a cotton bud or everted with thumb after asking the patient to look down. Examine with a 2.5× binocular loupe (or slit-lamp). Grade TF/TI/TS on the everted upper tarsal conjunctiva. Grade TT by looking at the lid margin in the open position. Grade CO by direct illumination of the cornea.
SELF-CHECK
In a community survey for trachoma control, you examine a 7-year-old child and find 6 follicles, each approximately 0.8 mm in diameter, on the central upper tarsal conjunctiva. The deep tarsal vessels are clearly visible through the conjunctiva. There is no scarring, trichiasis, or corneal opacity. What is the correct WHO grade?
A. TI — Trachomatous Inflammation-Intense
B. TF — Trachomatous Inflammation-Follicular
C. TS — Trachomatous Scarring
D. This child does not have trachoma — fewer than 10 follicles
Reveal Answer
Answer: B. TF — Trachomatous Inflammation-Follicular
TF is defined as ≥5 follicles each ≥0.5 mm on the central upper tarsal conjunctiva. This child has 6 follicles of 0.8 mm — which meets the TF criterion. TI requires the inflammation to obscure MORE than 50% of the deep tarsal vessels — they are visible here, so TI is absent. The threshold for TF is ≥5 follicles (not ≥10), which is a commonly tested fact. This child should receive azithromycin treatment and community-level intervention under the SAFE strategy.
Differential Diagnosis of Chronic Follicular Conjunctivitis
Trachoma must be distinguished from other conditions that produce a chronic follicular reaction on the palpebral conjunctiva. The differential matters clinically because the treatment differs significantly, and misdiagnosis — particularly confusing trachoma with a self-limiting viral folliculosis — can lead to disease progression and preventable blindness.
The main differentials are:
1. Chlamydial inclusion conjunctivitis (adult):
Caused by serotypes D-K; sexually transmitted; does NOT cause scarring; typically unilateral; associated with urogenital symptoms (cervicitis, urethritis); preauricular node present; resolves with systemic azithromycin without sequelae. Key difference from trachoma: NO Arlt's line, NO trichiasis, NOT in a rural endemic community.
2. Adenoviral EKC (chronic phase):
The subepithelial infiltrates of EKC persist for months and the follicular reaction can be mistaken for chronic conjunctivitis. However, EKC has a clear acute onset, is not associated with scarring, and does not cause trichiasis. There is usually a history of epidemic exposure or healthcare worker contact.
3. Toxic folliculosis:
Follicles induced by long-term preserved topical eye drops (especially apraclonidine, brimonidine, or preserved artificial tears). History of chronic topical medication use is diagnostic. Follicles are concentrated in the inferior fornix. Treatment is cessation of the causative drop.
4. Folliculosis of childhood:
A benign physiological state in children 5–15 years in which the conjunctiva naturally produces small follicles (especially inferior) with no inflammation, discharge, or scarring. These are NORMAL and do not require treatment. The distinction from trachoma (TF) is important: physiological folliculosis affects the inferior fornix predominantly; trachoma follicles must be ≥0.5 mm on the UPPER tarsal conjunctiva.
5. Molluscum contagiosum blepharoconjunctivitis:
Perl-white umbilicated nodules on the eyelid margin produce a chronic ipsilateral follicular conjunctivitis. The conjunctivitis resolves when the lid nodule is excised. Examination of the lid margin is diagnostic.
| Feature | Trachoma | Inclusion | Folliculosis (physiological) | Molluscum |
|---|---|---|---|---|
| Location of follicles | Upper tarsal | Lower fornix | Lower fornix | Lower fornix |
| Scarring (TS/Arlt's line) | Yes | No | No | No |
| Endemic setting | Yes | No | No | No |
| Lid nodule | No | No | No | Yes (margin) |
| Systemic Cx treatment | Yes | Yes | No | No (lid surgery) |
CLINICAL PEARL
Herbert's pits are pathognomonic of trachoma — even in a patient who no longer has active trachoma. These small depressions at the upper limbus represent the scars of healed limbal follicles (follicles at the corneal margin, which are not seen in other follicular conjunctivitides). When you examine a middle-aged patient with reduced vision and a clear cornea and someone asks 'was this trachoma?' — look at the limbus for Herbert's pits. Their presence tells you the diagnosis even decades after the active disease has resolved.
Management and the SAFE Strategy
Trachoma management operates at two levels: the individual patient (who may have active disease, trichiasis, or both) and the community (where control requires breaking the transmission cycle). The WHO SAFE strategy provides a comprehensive framework that addresses both levels and is the current international standard for trachoma elimination programmes, including India's NPCBVI initiatives.
Provided image
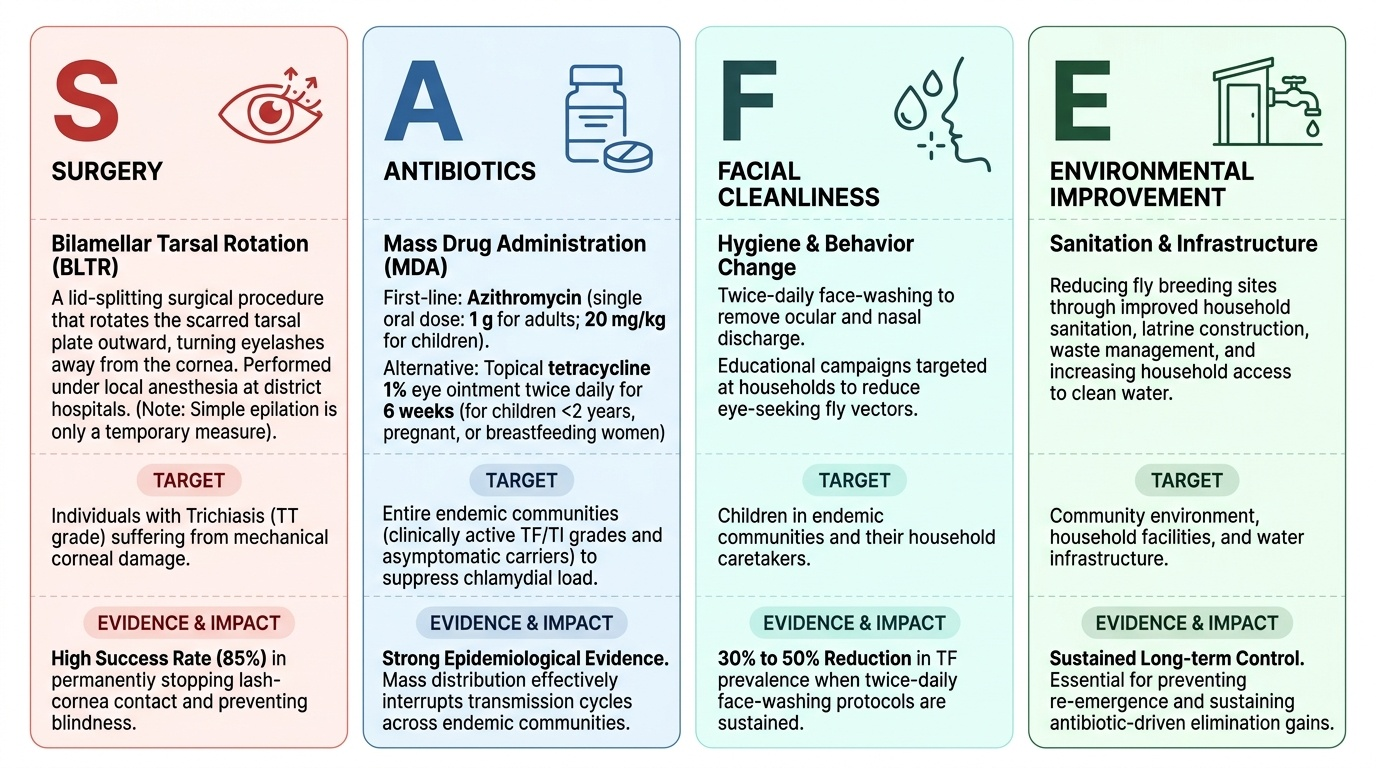
SAFE = Surgery, Antibiotics, Facial cleanliness, Environmental improvement.
S — Surgery (for Trichiasis = TT grade):
Once trichiasis has developed, the mechanical damage to the cornea continues with every blink until the eyelid position is corrected. The procedure of choice is bilamellar tarsal rotation (BLTR) — a lid-splitting procedure that rotates the scarred tarsal plate outward, turning the lashes away from the cornea. This can be performed under local anaesthesia at the district hospital level and is highly effective (>85% success in stopping lash-cornea contact). Simple epilation (pulling out the offending lashes) is only a temporary measure as lashes regrow, often more aberrantly.
A — Antibiotics (for active disease = TF/TI grades):
The antibiotic of choice is azithromycin (single oral dose: 1 g for adults; 20 mg/kg for children, maximum 1 g). It is given as mass drug administration (MDA) to entire endemic communities (not just clinically affected individuals) to suppress the community chlamydial load and interrupt transmission. Topical tetracycline 1% eye ointment twice daily for 6 weeks is the alternative for children under 2 years, pregnant, or breastfeeding women (azithromycin is generally avoided in this group). Individual treatment: azithromycin is given for confirmed TF/TI in a child or adult.
F — Facial cleanliness:
Regular face-washing in children, particularly washing away the ocular discharge that attracts flies, dramatically reduces transmission. Nasal discharge is also a major source of chlamydiae. Programmes that promote twice-daily face-washing have been shown to reduce TF prevalence by 30–50% in endemic communities.
E — Environmental improvement:
Reducing fly density (through improved sanitation, latrine construction, waste management), increasing access to clean water, and reducing overcrowding address the root environmental determinants of trachoma transmission. These interventions sustain the antibiotic programme's gains and are essential for achieving the WHO elimination target.
Complications and their management:
- Dry eye from goblet cell loss (TS stage) → lubricant eye drops.
- Corneal opacity (CO stage) → penetrating keratoplasty if in the visual axis, though access is limited in endemic settings.
- Secondary bacterial infection in the scarred conjunctiva → topical antibiotics for acute flares.
SELF-CHECK
A 6-year-old boy in a trachoma-endemic village has been diagnosed with TF (active follicular trachoma). His two younger siblings and mother appear unaffected. The correct management under the WHO SAFE strategy is:
A. Treat only the affected child with oral azithromycin and reassure the family
B. Mass drug administration (azithromycin) to the entire community plus face-washing and environmental improvement
C. Topical tetracycline for the child only, for 6 weeks
D. Surgery for the child and topical antibiotics for the family
Reveal Answer
Answer: B. Mass drug administration (azithromycin) to the entire community plus face-washing and environmental improvement
The SAFE strategy addresses trachoma at the community level, not just the individual. Even when only one child appears to have TF, the community prevalence in endemic areas is high and many individuals have subclinical infection. The recommended response is mass drug administration (azithromycin to the entire community of appropriate age) combined with face-washing promotion and environmental improvement to break the transmission cycle. Treating only the individual child while leaving the reservoir intact will result in rapid reinfection. Surgery is only relevant when trichiasis (TT) is present.
Self-Assessment
Review your mastery of the OP3.3 competency requirements. You should be able to enumerate the causes of chronic conjunctivitis in four categories (infective, immunological, toxic, degenerative) and name the specific aetiologic agent for each; describe the progression of trachoma from follicular inflammation to corneal blindness through the cicatricial mechanism; apply the WHO five-sign grading system accurately — remembering the specific threshold for TF (≥5 follicles, ≥0.5 mm, upper tarsal), the threshold for TI (>50% deep vessels obscured), and what Arlt's line represents (TS); distinguish trachoma follicles (upper tarsal, ≥0.5 mm) from the physiological folliculosis of childhood (inferior fornix, smaller, no inflammation); and recall the SAFE acronym with its specific components including the correct antibiotic (azithromycin 1 g single dose) and surgery type (bilamellar tarsal rotation).
Key facts for revision:
- Trachoma serotypes: A, B, Ba, C (not D-K which cause inclusion conjunctivitis)
- TF threshold: ≥5 follicles each ≥0.5 mm on the upper tarsal conjunctiva
- Pathognomonic signs: Arlt's line (TS) and Herbert's pits (limbal scars)
- Blinding mechanism: follicles → scarring → entropion → trichiasis → corneal abrasion → opacity
- SAFE: Surgery (BLTR), Antibiotics (azithromycin MDA), Facial cleanliness, Environmental improvement