Page 17 of 27
OP3.6 | Conjunctival Foreign Body Removal in Simulation — SDL Guide
Learning Objectives
- Demonstrate the correct technique of conjunctival and subtarsal foreign body removal in a simulated environment
- Identify the clinical features that distinguish a simple conjunctival FB from a penetrating ocular injury requiring urgent referral
- Describe the significance of vertical linear corneal scratches as a sign of a subtarsal foreign body
- Outline the post-removal care and indications for specialist referral
INSTRUCTIONS
Ocular foreign bodies are one of the most common presentations to primary care and emergency departments. The vast majority are superficial conjunctival or subtarsal foreign bodies that can be safely removed by a trained MBBS doctor with basic equipment and topical local anaesthesia. However, the same scenario of 'something in the eye' can occasionally represent a penetrating ocular injury — which must NEVER be manipulated at primary care. The NMC OP3.6 competency requires you to demonstrate the removal technique in simulation and to distinguish safely manageable from referral-requiring cases.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 6: Diseases of Conjunctiva; Ch. 5: Corneal Disorders (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 8: Conjunctiva; Ch. 32: Injuries to the Eye (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 25-year-old construction worker is brought to your clinic at 11 AM with severe pain in the right eye since a piece of metal flew into it while he was grinding steel without protective goggles, approximately 30 minutes ago. The eye is red and watering profusely. He is asking you to 'remove whatever is in there.' You examine the eye — his VA is 6/6, the pupil is round and reactive, the cornea looks clear. On everting the upper eyelid, you see a small grey metallic fragment sitting on the palpebral conjunctiva. What do you do next? And what would make you stop and refer instead of proceeding?
WHY THIS MATTERS
Ocular foreign body is one of the most common occupational eye injuries globally and a frequent presentation at government health centres, casualty departments, and private general practice in India. Without proper protective eyewear — the most preventable aspect — it affects agricultural workers (dust, hay, wheat husks), industrial workers (metal fragments, welding sparks), mechanics (metal shavings), and construction workers (stone chips, cement splashes). The OP3.6 skill competency is designated at the SH (Skill in a simulated or supervised setting) level — you are expected to demonstrate the removal technique in your skills laboratory. A doctor who cannot remove a simple subtarsal foreign body is unable to provide basic eye care in a primary health setting, and a doctor who attempts removal of a penetrating foreign body can cause catastrophic loss of the eye.
RECALL
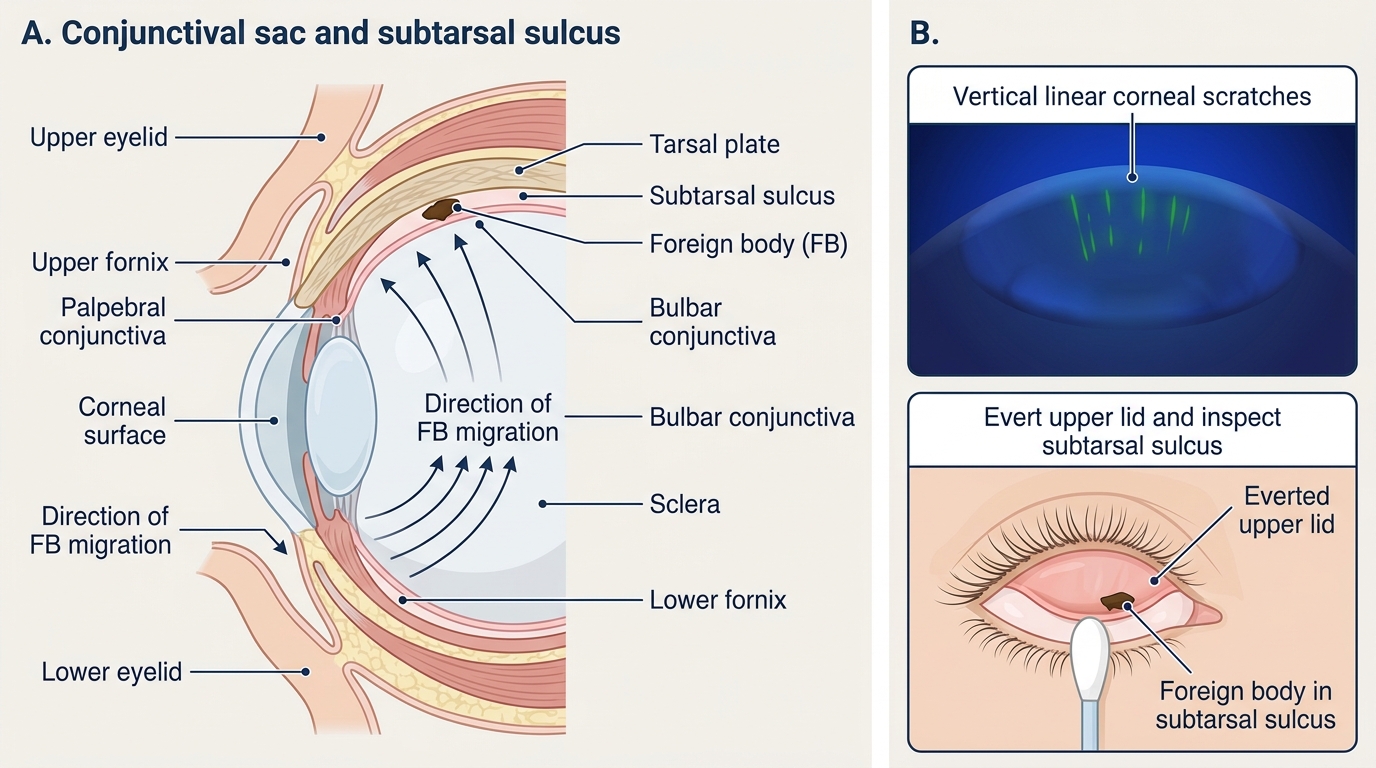
Recall from your ophthalmic anatomy sessions that the conjunctival sac is a potential space formed between the palpebral conjunctiva (lining the inner eyelids) and the bulbar conjunctiva (on the scleral surface). The deepest recesses of this space are the superior and inferior fornices. The upper fornix extends 8–10 mm behind the upper lid margin. Under the upper eyelid, just above the tarsal plate margin, is the subtarsal sulcus — a shallow groove where the tarsal plate's inferior edge meets the conjunctiva. Foreign bodies frequently lodge in this subtarsal sulcus because the blinking motion sweeps particles from the bulbar surface up under the lid, where they get trapped in the groove. Every blink then drags the trapped particle across the corneal surface — producing the pathognomonic vertical linear scratches visible on fluorescein staining.
Why Conjunctival Foreign Bodies Are Common and Can Be Serious
Ocular foreign bodies represent a spectrum of injury from trivially discomforting to catastrophically blinding, and the critical skill for a primary-care clinician is to accurately locate the injury on this spectrum within the first two minutes of assessment. The vast majority of foreign bodies are superficial — they sit on the conjunctival surface or under the upper eyelid, have not breached the eye wall, and can be safely removed with basic equipment. However, a high-velocity metallic or glass fragment (from grinding, hammering, or explosions) can penetrate the eye wall, enter the anterior chamber or vitreous, and cause immediate or progressive damage to the lens, retina, and optic nerve. The risk of confusion between these two scenarios is real: both present as 'eye pain after something flew in.'
The epidemiology of ocular FBs in India reflects the occupational profile: metallic fragments from metalwork, sparks from welding, vegetative matter (husks, seeds) from agricultural work, sand and grit from construction, and cement splashes. Eyelashes (in trichiasis), insect parts, and dust are also common conjunctival irritants. In the vast majority of cases, the FB is non-magnetic, inert, and superficial. The two materials that demand urgent intervention even when superficial are iron (which oxidises to form a rust ring on the cornea) and copper (which is directly toxic to intraocular tissues via chalcosis).
Key clinical fact: the absence of protective eyewear during grinding or chipping work is the single strongest risk factor for penetrating FB injury, because the velocity of ejected particles during these activities is far higher than during hand work.
Anatomy of the Conjunctival Sac and Where FBs Lodge
Understanding where foreign bodies lodge requires a clear mental map of the conjunctival sac and the flow dynamics of the blinking mechanism.
The conjunctival sac is the potential space between the palpebral and bulbar conjunctival surfaces. It is closed anteriorly at the lid margins and opens at the palpebral aperture. Its deepest parts are the fornices — the superior fornix (extending approximately 8–10 mm posterior to the upper lid margin) and the inferior fornix (4–6 mm posterior to the lower lid margin).
The subtarsal sulcus is a groove running horizontally at the inferior margin of the upper tarsal plate, on the palpebral conjunctival surface of the upper lid. Because of its position, foreign bodies swept under the upper lid by the blinking action tend to be caught in this sulcus. Once lodged there, the FB is pressed against the corneal surface with every blink, producing characteristic vertical linear corneal scratches — fine parallel lines running vertically across the superior cornea, visible on fluorescein staining under cobalt-blue light. The pattern is vertical because the upper lid moves vertically (down and up) with each blink.
This vertical scratch pattern is the key indirect sign of a subtarsal foreign body when the patient cannot feel an FB directly but keeps reporting persistent irritation after the initial FB feeling. The finding of vertical linear corneal scratches on fluorescein staining should prompt immediate examination by upper lid eversion, even if the patient denies a history of FB entry.
Foreign bodies may also lodge on the bulbar conjunctiva (visible without lid eversion — usually seen directly) or, in more serious cases, become embedded in the corneal stroma (requiring specialist removal). Intraocular FBs penetrate the full thickness of the eye wall.
Subtarsal Foreign Body in the Conjunctival Sac
SELF-CHECK
A 19-year-old student has had a gritty, irritated right eye for 2 days after a strong dusty wind. Fluorescein staining under cobalt-blue light reveals multiple fine vertical parallel scratches on the superior cornea but no discrete corneal ulcer. No FB is visible on the bulbar conjunctiva. The most appropriate next step is:
A. Prescribe topical chloramphenicol for presumed bacterial keratitis
B. Evert the upper eyelid and examine the subtarsal sulcus for a foreign body
C. Refer immediately for suspected viral dendritic ulcer
D. Reassure and prescribe lubricant drops only
Reveal Answer
Answer: B. Evert the upper eyelid and examine the subtarsal sulcus for a foreign body
Vertical linear corneal scratches on fluorescein staining are the pathognomonic indirect sign of a subtarsal foreign body — caused by the trapped FB rubbing against the corneal epithelium with each blink. These scratches do NOT represent bacterial keratitis (which would show a focal ulcer with surrounding infiltrate) or viral dendritic disease (branching pattern). The correct response is to evert the upper eyelid and examine the subtarsal sulcus. Prescribing antibiotics without searching for the FB treats the effect (corneal damage) while the cause continues rubbing.
Assessment Before Removal: History, Examination, and Red Flags
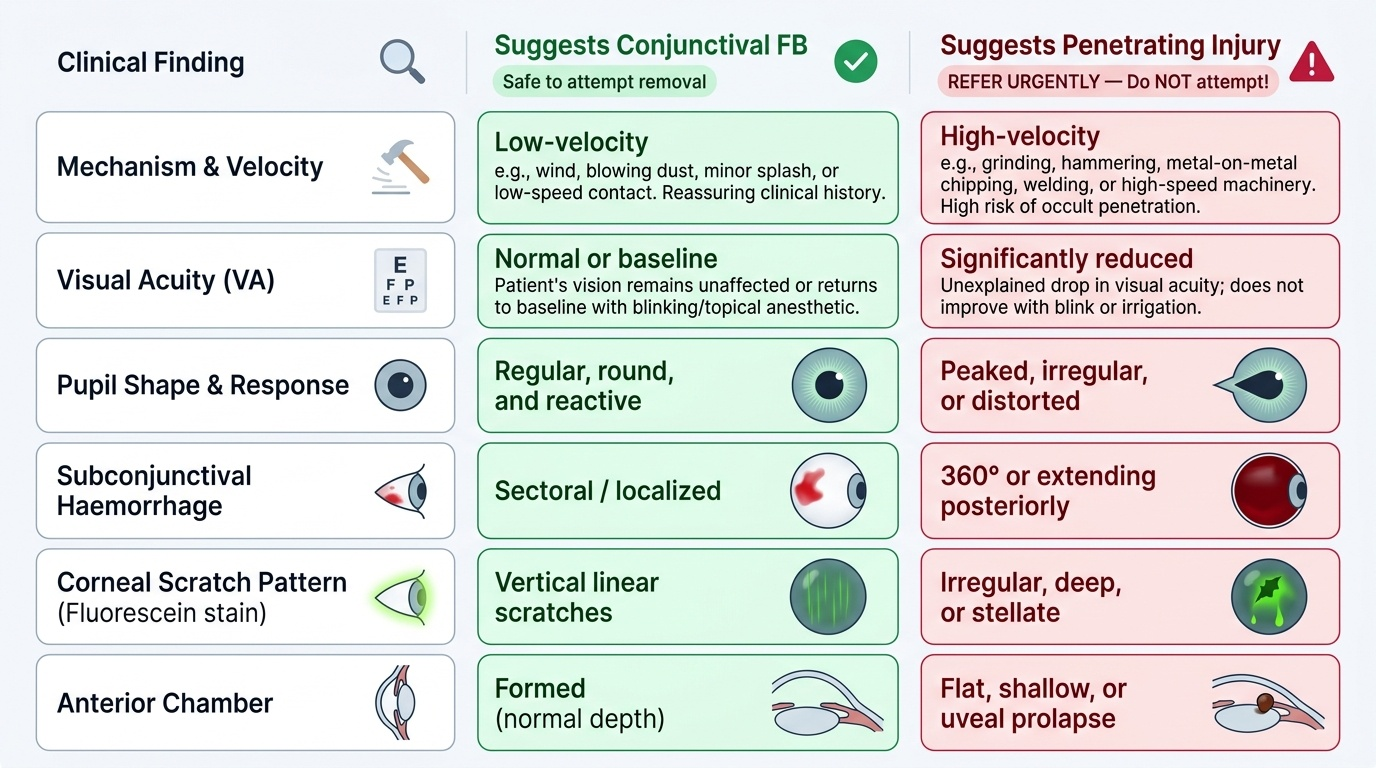
Before any attempt at FB removal, a systematic assessment identifies whether this is a safe primary-care procedure or a referral case. The assessment takes approximately 2–3 minutes and must not be skipped, even when the patient is in pain and requesting immediate removal. The reason this two-to-three-minute investment is non-negotiable is that the consequences of skipping it are asymmetric: the cost of over-caution (referring a simple conjunctival FB that you could have removed) is a small inconvenience to the patient; the cost of under-caution (attempting removal of a penetrating ocular injury) is catastrophic and irreversible. A clinician who applies pressure to an eye with an unsuspected rupture — even with gentle cotton-bud manipulation — risks expelling intraocular contents through the wound, converting a surgically repairable penetrating injury into a devastated globe. The assessment framework below is designed to be completed systematically and quickly, and each element corresponds directly to a specific red-flag sign that changes the management from 'remove here' to 'refer immediately.' Do not shortcut any step under time pressure.
Provided image
History — three critical questions:
1. Mechanism and velocity: 'What were you doing when this happened?' — grinding, hammering, chipping, welding, wind, or a blow? High-velocity metallic fragments from grinding or hammering carry the highest risk of penetration; low-velocity dust or wind is reassuring.
2. Material: metal, glass, wood, vegetable matter? Wood and vegetable matter carry infection risk (fungi). Metal carries rust-ring risk.
3. Time since injury: Corneal epithelium starts regenerating within hours — prolonged delay may mean the FB has become embedded.
Examination — standard sequence:
1. Visual acuity (both eyes) — reduced VA in the affected eye is a red flag for serious injury.
2. Inspect the lids and periorbita — lacerations, ecchymosis.
3. Inspect the conjunctiva and sclera — look for full-thickness laceration, subconjunctival haemorrhage extending to the posterior limit (which can mask scleral rupture).
4. Inspect the cornea — clarity, any visible wound track, keratomalacia.
5. Examine the pupil — regular vs irregular or peaked (pointing toward a penetrating wound).
6. Fluorescein staining — apply 1 drop of fluorescein; look under cobalt-blue torch light for green-staining epithelial defects; the Seidel test (streaming of fluorescein from a wound indicating aqueous outflow) is positive in a perforating wound.
7. Evert the upper eyelid — look for the FB in the subtarsal sulcus.
Red flags — refer immediately, do NOT attempt removal:
- Reduced VA.
- Peaked or irregular pupil.
- Visible uveal tissue (iris or ciliary body) prolapsing through a wound.
- Subconjunctival haemorrhage extending to the posterior limit (haemorrhage all the way back, suggesting posterior rupture).
- 360° chemosis with a flat anterior chamber.
- Seidel test positive.
- History of high-velocity injury (grinding, hammering).
- FB suspected to be intraocular — refer for X-ray of orbit or B-scan ultrasound.
If ANY red flag is present: pad the eye without applying pressure, give analgesia, and arrange immediate ophthalmology transfer.