Page 14 of 27
OP3.5 | Pterygium — SDL Guide
Learning Objectives
- Describe the aetiology, pathophysiology, and ocular features of pterygium
- Distinguish pterygium from pseudopterygium, pinguecula, and other conjunctival lesions
- Outline the indications for surgical management and describe the surgical options with their recurrence rates
- Identify Stocker's line as a pathognomonic feature of pterygium
INSTRUCTIONS
Pterygium is a common conjunctival condition in tropical and subtropical regions, including India, where prolonged UV-B exposure, dust, and outdoor work contribute to its prevalence. It presents as a visible fleshy triangular growth on the white of the eye and can reduce vision through corneal invasion or induced astigmatism. The NMC OP3.5 competency requires you to understand the full clinical picture — from its benign stable form to the progressive form requiring surgery — and to distinguish it from conditions that mimic its appearance, particularly pseudopterygium.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 6: Diseases of Conjunctiva (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 8: Diseases of the Conjunctiva (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 50-year-old agricultural labourer from coastal Tamil Nadu has noticed a 'growth on the white of his right eye' for the past 10 years. He says it has recently been covering more of his eye and his vision has gradually become 'blurry and distorted'. He also wears no glasses. On examination, his visual acuity is 6/18 in the right eye, pinhole does NOT improve it. You see a pink triangular fleshy tissue growing from the nasal conjunctiva across the limbus, and its tip is now only 2 mm away from the centre of his cornea. A faint brownish line runs across the cornea just ahead of the tissue's leading edge. What is this growth, what is causing the visual loss, and when should it be removed?
WHY THIS MATTERS
Pterygium is one of the most common ocular conditions encountered in general practice, especially in India's tropical states and among outdoor workers (farmers, fishermen, construction workers). It is not merely a cosmetic nuisance — as it advances onto the cornea, it can distort the corneal curvature (inducing irregular astigmatism that does not correct with pinhole) and ultimately cover the visual axis, causing irreversible corneal scarring. The OP3.5 competency asks you to understand the full clinical picture — distinguishing pterygium from pseudopterygium and other mimics, assessing when surgery is needed, and knowing why the recurrence rate after excision depends critically on surgical technique.
RECALL
Recall from your ophthalmology anatomy sessions that the limbus is the 3 mm transitional zone between the clear avascular cornea and the white vascular sclera. It contains the corneal limbal stem cells — the progenitor cells that maintain the corneal epithelial surface. These cells form a barrier that normally prevents conjunctival epithelium from migrating onto the corneal surface. From your histology module, recall that the conjunctival stroma contains fibrocytes and collagen — the same elements that are abnormally activated in pterygium. Also recall that UV-B radiation (wavelength 280–315 nm) damages DNA and triggers aberrant cellular proliferation — the same mechanism that underlies both skin melanoma and UV-related ocular disease.
The Fleshy Growth on the Eye — Clinical Presentation of Pterygium
Pterygium (Greek: pteryx = wing) is a wing-shaped fibrovascular growth of bulbar conjunctival tissue that extends across the limbus onto the corneal surface. It is almost invariably located on the nasal side of the eye — the nasal conjunctiva receives the maximum UV-B exposure (from light reflecting off the nasal bridge and the narrow angle between the lid margin and the eyeball). Temporal pterygium is much rarer. Bilateral pterygium in both nasal quadrants can occur.
The typical patient is a middle-aged or older person from a tropical or subtropical region with a history of prolonged outdoor UV exposure — agriculture, fishing, construction, or military service. In India, pterygium is particularly prevalent in coastal and dry-land farming populations. Men are more commonly affected than women, likely due to greater outdoor work exposure.
Clinical presentation:
- The patient notices a visible pinkish-red fleshy lesion on the white of the eye, often remarked upon by family members before symptoms appear.
- Redness and irritation — the vascularised body of the pterygium causes chronic conjunctival hyperaemia.
- Foreign body sensation — from disruption of the tear film by the tissue on the cornea.
- Visual disturbance — as the pterygium advances onto the cornea, it distorts the corneal curvature, inducing irregular astigmatism that causes blurring not correctable with pinhole. When the pterygium covers the visual axis, visual acuity is directly reduced.
- Restricted eye movement — large pterygium can limit abduction (as the nasal conjunctiva is tethered to the nasal fornix by the pterygium body).
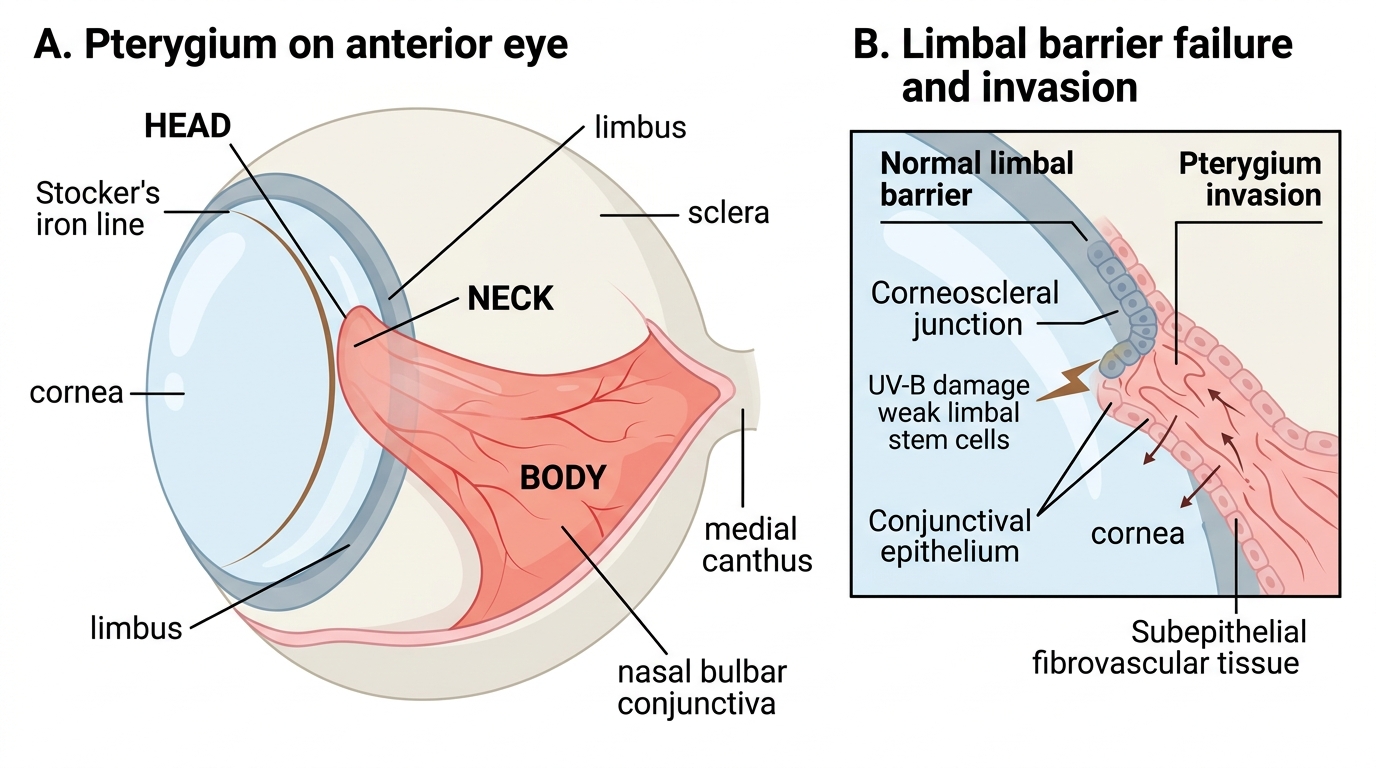
Pterygium: Anatomy and Limbal Invasion
Pathogenesis: UV Damage, Limbal Stem Cells, and Fibrovascular Invasion
The pathogenesis of pterygium is most coherently explained by the limbal stem cell failure hypothesis, supported by the observation that UV-B radiation is the dominant environmental risk factor and that pterygium tissue represents conjunctival (not corneal) epithelium that has breached the limbal barrier.
Normal limbal stem cells form a functional boundary at the corneoscleral junction that prevents conjunctival epithelium from invading the cornea. Chronic UV-B exposure damages the DNA of these limbal stem cells through oxidative stress and the formation of pyrimidine dimers, impairing their proliferative and barrier functions. Once the barrier is compromised, the conjunctival epithelium — with its subepithelial fibroblasts — begins to migrate centripetally onto the corneal surface. The clinical implication of this pathogenetic model is important: pterygium is a disease of limbal barrier failure driven by cumulative UV-B dose, not a simple inflammatory or neoplastic process. This is why UV-B protection (sunglasses with UV400 rating, wide-brimmed hats) is the only evidence-based preventive measure, and why recurrence after surgical excision is so common — if the UV-B exposure continues and the limbal stem cell dysfunction persists, the barrier will fail again and the tissue will regrow. The three components of the invading tissue are described below.
The migrating tissue has several components:
1. Abnormally active fibroblasts — which lay down disorganised extracellular matrix (fibronectin, tenascin, matrix metalloproteinases). The expression of matrix metalloproteinases (particularly MMP-2 and MMP-9) by pterygium fibroblasts is responsible for the dissolution of Bowman's layer (the acellular zone beneath the corneal epithelium) as the pterygium head advances.
2. Vascular component — the pterygium body is richly vascularised (hence its pink-red colour), fed by dilated conjunctival vessels from the body and neck that branch to supply the advancing head.
3. Inflammatory cell infiltration — mast cells, lymphocytes, and macrophages are present in the pterygium stroma; UV-B induces the production of pro-inflammatory cytokines (VEGF, TGF-β) that sustain the fibrovascular proliferation.
Other risk factors that compound UV-B exposure: dusty environments (chronic ocular surface irritation), dry climates, low altitude (higher UV levels at equatorial latitudes), lack of UV-protective eyewear.
Stocker's line: At the leading edge of the pterygium head, a brownish horizontal line of iron (haemosiderin) deposits in the corneal epithelium — the Stocker's line — is pathognomonic of pterygium. It forms from tear-film iron deposits at the epithelial margin of the pterygium-cornea interface and is best seen under slit-lamp examination with a yellow filter.
SELF-CHECK
A patient with a pterygium on the nasal side of his right eye has a faint brownish horizontal line visible on the cornea just ahead of the pterygium's advancing tip. This line is called:
A. Hudson-Stähli line
B. Stocker's line
C. Arlt's line
D. Fleischer ring
Reveal Answer
Answer: B. Stocker's line
Stocker's line is the iron (haemosiderin) deposit in the corneal epithelium at the leading edge of the pterygium head — it is pathognomonic of pterygium. The Hudson-Stähli line is a horizontal iron deposit in the lower corneal epithelium in normal ageing. Arlt's line is the tarsal scar of trachoma. The Fleischer ring is a ring of iron deposits at the base of the cone in keratoconus. Each is an iron deposit at a different location for a different reason — the location and context identify them.
Examining and Grading a Pterygium
Clinical examination of a pterygium requires documentation of four parameters that determine the management decision: the anatomy of the pterygium components, the extent of corneal involvement, the visual acuity, and the activity (progressive vs stationary). This structured approach prevents the common clinical error of simply noting 'pterygium present' without quantifying the key variables that inform the decision to observe versus refer for surgery. The single most clinically critical measurement is the distance of the pterygium head from the pupillary margin — a pterygium that has reached within 2–3 mm of the pupil will threaten the visual axis within months in an active growing pterygium, while one 5–6 mm away in a stationary thin pterygium may be safely watched for years. Documentation of these parameters at each visit also allows detection of progression by serial comparison, which is the only reliable way to identify an active pterygium in an otherwise quiet eye.
Anatomy — three parts of a pterygium:
- Head (cap): The most advanced part, sitting on the cornea; the apex of the triangular wing. Examine the cornea immediately ahead of the head for Stocker's line.
- Neck: The narrowest part at the limbus, where the corneal and conjunctival portions meet.
- Body: The broad triangular conjunctival portion; shows the vascular pattern; may have dilated 'feeder vessels' from the conjunctiva.
Grading by corneal extent:
The most clinically important measurement is how far the head has advanced onto the cornea, measured in millimetres from the limbus:
- Grade 1 (T1): thin, transparent — only slightly overlapping the cornea, able to see corneal vessels through the tissue.
- Grade 2 (T2): intermediate — partially obscuring the corneal surface.
- Grade 3 (T3): thick, opaque — completely obscuring the corneal vessels beneath; near the visual axis.
Surgery is generally indicated when the pterygium approaches within 2–3 mm of the pupillary margin or has reached Grade 3.
Visual acuity and refraction:
Test VA in both eyes. If VA is reduced and the pterygium overlies the cornea, try to determine whether the reduction is from induced astigmatism (the pterygium flattens the corneal curvature in the horizontal meridian as it invades) or from direct visual-axis coverage. Importantly, pterygium-induced astigmatism does NOT improve with pinhole (because it is corneal distortion, not simple refractive error).
Activity assessment:
Signs of an active (progressive) pterygium: prominent vascularity of the body, thick head, Stocker's line close behind the head (indicating recent advance). A stationary pterygium is avascular, thin, and translucent.