Page 2 of 27
OP3.1 | Red Eye History Taking and Cause Framework — SDL Guide (Part 2)
Pattern Recognition: Matching History to Diagnosis
Once you have completed the systematic history, the pattern of symptoms points reliably towards a diagnostic group. The key discriminators are (1) discharge type, (2) pain severity, (3) photophobia, and (4) vision change. Mastering this pattern-matching step allows you to arrive at the correct differential before examining the eye — the examination then confirms, not discovers, the diagnosis. This cognitive skill — reading the history as a fingerprint of the underlying pathology — is what separates an experienced clinician from a junior who relies entirely on the slit-lamp. Each diagnostic group has a characteristic symptom fingerprint, and practising pattern recognition on representative cases until the pattern is automatic is the most efficient way to build clinical expertise. The table below formalises the patterns you need to internalise; study it initially with the 'Other history features' column covered, and practise predicting the diagnosis from discharge type, pain, photophobia, and vision change alone, before revealing the confirming details.
Provided image
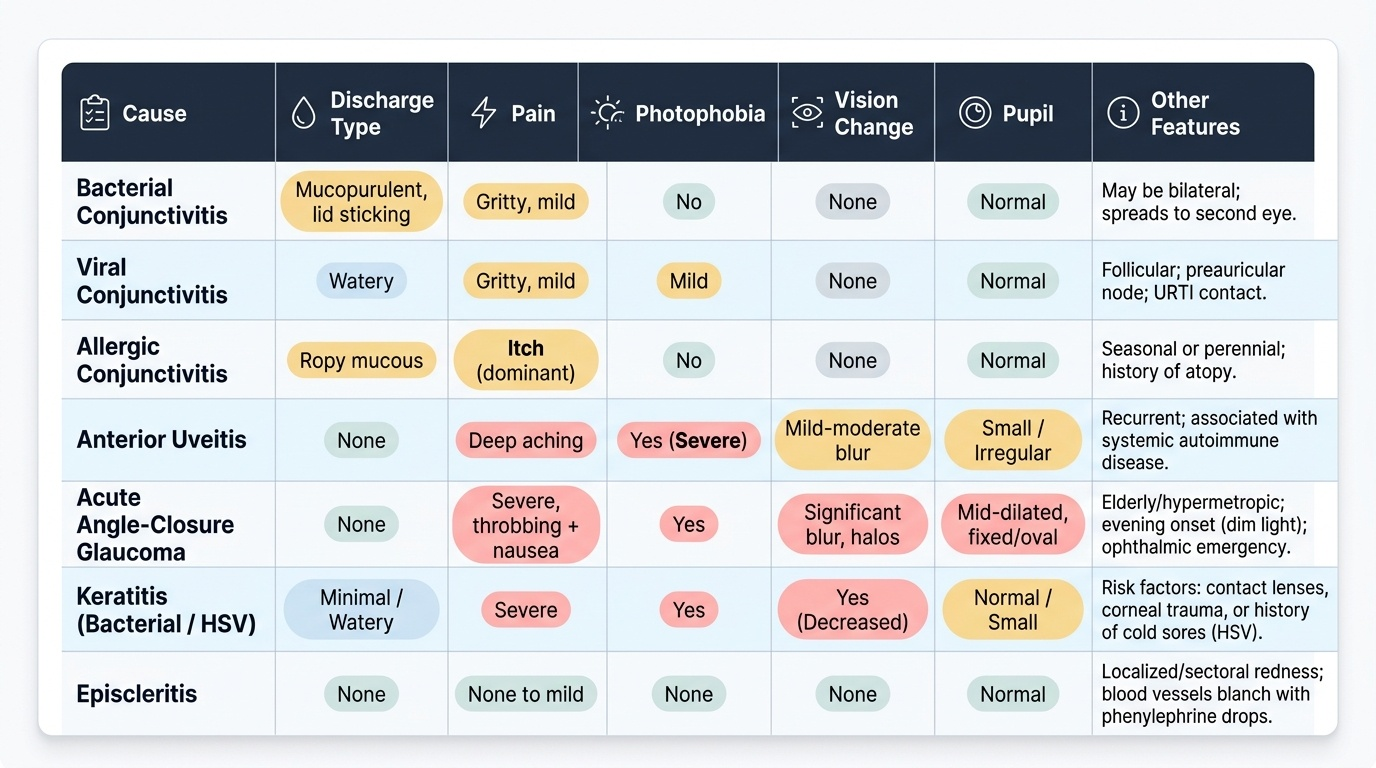
The matrix below integrates the most important causes with their characteristic history profiles. Study it until the pattern is automatic:
| Cause | Discharge | Pain | Photophobia | Vision change | Other history features |
|---|---|---|---|---|---|
| Bacterial conjunctivitis | Mucopurulent, lid sticking | Gritty, mild | No | None | May be bilateral; spreads to second eye |
| Viral conjunctivitis | Watery | Gritty | Mild | None | Follicular; preauricular node; URTI contact |
| Allergic conjunctivitis | Ropy mucous | Itch (dominant) | No | None | Seasonal or perennial; atopy |
| Anterior uveitis | None | Deep aching | Yes | Mild–moderate blur | Recurrent; systemic autoimmune disease |
| Acute angle-closure glaucoma | None | Severe, throbbing + nausea | Halos | Significant | Elderly/hypermetropic; evening onset (dim light) |
| Bacterial keratitis | Minimal | Severe | Yes | Yes | Contact lenses; corneal FB/trauma |
| Herpes simplex keratitis | Minimal/watery | Moderate | Yes | Yes | Recurrent; prior cold sores |
| Subconjunctival haemorrhage | None | None | No | None | Painless flat red patch; sneezing/straining |
| Scleritis | None | Severe, boring, nocturnal | Mild | No/mild | Systemic connective-tissue disease |
Two patterns demand immediate recognition:
1. The benign pattern: watery or mucopurulent discharge + gritty discomfort + no photophobia + normal vision = almost certainly conjunctivitis. Safe to treat at primary care level.
2. The dangerous pattern: any of pain (more than gritty) + photophobia + reduced vision + ciliary flush + corneal opacity = potentially sight-threatening, refer URGENTLY.
SELF-CHECK
A 28-year-old woman has had a unilateral red eye for 2 days with deep aching pain, photophobia, and slightly blurred vision. There is no discharge and she had a similar episode 18 months ago. The most important diagnosis to consider urgently is:
A. Acute bacterial conjunctivitis
B. Anterior uveitis (iritis)
C. Epidemic viral keratoconjunctivitis
D. Subconjunctival haemorrhage
Reveal Answer
Answer: B. Anterior uveitis (iritis)
Anterior uveitis (iritis) presents with unilateral red eye, deep aching pain, photophobia (from iris sphincter spasm), and mild reduction in vision. The absence of discharge, recurrent nature, and combination of pain + photophobia + vision change distinguish it sharply from conjunctivitis (no photophobia, normal vision, discharge present). Recurrent unilateral uveitis is often associated with HLA-B27 positive conditions (ankylosing spondylitis, IBD, psoriatic arthritis). This is a danger-sign pattern requiring urgent ophthalmology referral.
Danger Signs and the Referral Decision
The practical output of the history in a red-eye consultation is a binary decision: 'I can manage this here' or 'this patient needs urgent ophthalmology review.' The danger-sign framework operationalises this decision by providing a checklist of five clinical features any ONE of which should trigger referral. This framework is taught in the UK Royal College of Ophthalmologists guidelines, Khurana's Comprehensive Ophthalmology, and is the basis of the NMC OP3.1 competency. The reason a checklist approach is necessary is that each danger sign operates independently — a patient can have only one danger sign among an otherwise reassuring picture, and that single sign is sufficient to mandate urgent referral. The clinical trap is false reassurance from the overall benign appearance of the eye: a slightly red eye with clear discharge and what seems like mild grittiness can conceal early anterior uveitis if the examiner does not actively ask about photophobia and test visual acuity. Applying the danger-sign framework takes less than 60 seconds and can prevent a patient from going home with antibiotic drops when they need a slit-lamp examination within hours.
The five danger signs — remembered by the mnemonic PPPCC — are:
1. Pain — not gritty discomfort but true ocular pain or headache around the eye, especially if severe or throbbing.
2. Photophobia — pain on exposure to bright light, indicating corneal or uveal inflammation.
3. Pupil abnormality — fixed mid-dilated pupil (acute angle-closure — oval, fixed, mid-dilated); small irregular pupil with posterior synechiae (uveitis).
4. Change in vision (VA reduced) — any reduction from the patient's baseline, even partial. Test with pinhole: if pinhole improves VA, the blur is refractive; if VA is reduced AND pinhole does NOT improve it, the cause is likely organic (corneal oedema, vitritis).
5. Corneal opacity or ciliary flush — corneal clouding, ulcer, or the characteristic circumcorneal violet injection of deep inflammation.
A patient with none of these five signs is highly unlikely to have a sight-threatening diagnosis. A patient with any one sign should not leave your hands without either a same-day ophthalmology review or, if that is unavailable, clear instructions to return immediately if symptoms worsen.
Special caution for acute angle-closure glaucoma: the classic presentation is a middle-aged or elderly hypermetropic (long-sighted) patient who develops sudden severe pain in one eye, typically in the evening when pupils are naturally dilated and the already-narrow angle closes completely. There may be vomiting and bradycardia from the vagal response to severe pain. This is an ocular emergency — every minute without treatment risks further ganglion-cell death. Treatment is IV acetazolamide + topical pilocarpine (to constrict the pupil and open the angle) + IV mannitol if pressure is very high, followed by laser peripheral iridotomy once the attack is broken.
For OP3.1, you are NOT expected to initiate this treatment yourself at SH level — but you ARE expected to recognise the presentation and arrange emergency referral within minutes.
CLINICAL PEARL
The gritty-eye trap: Patients with anterior uveitis sometimes describe their pain as 'gritty' or 'like something in my eye' in the early stages, because the corneal nerve irritation from ciliary spasm can mimic a foreign body sensation. The discriminating feature is photophobia — true conjunctivitis does not cause photophobia. Ask directly: 'Does bright light bother your eye? Do you want to close it in the light?' An affirmative answer with a red eye is anterior uveitis until proven otherwise.
Applied Practice: History-Taking in Simulated Scenarios
Competency in history taking is built through repeated practice on structured scenarios. The three archetypes below represent the most important diagnostic groups and are commonly used in OSCE examinations. Work through each using the template from the previous section; do not jump to diagnosis until you have completed every step. The purpose of working through scripted scenarios before the skills laboratory is to internalise the decision tree so that the history-taking process becomes automatic under examination pressure. In a real clinical or OSCE setting, the time pressure and the patient's distress can cause premature closure — the tendency to accept the first plausible diagnosis that fits a few features, without systematically checking for danger signs. The three scenarios below are chosen because each represents a different referral decision: reassure and treat, urgent same-day referral, and emergency call immediately. Practise not just taking the history but explicitly naming the danger signs present or absent, and stating your referral decision aloud — this mirrors exactly what an examiner expects.
Scenario 1 — The reassurance case (bacterial conjunctivitis):
A 22-year-old college student presents with both eyes red for 2 days. He woke up this morning with his eyelids stuck together. There is yellow discharge from both eyes. No pain beyond mild grittiness. No photophobia. Vision is normal after blinking. No contact lenses. Roommate had a similar episode last week.
- Pattern: bilateral, mucopurulent discharge, lid sticking, no photophobia, normal vision, contact history.
- Danger signs: none.
- Decision: bacterial conjunctivitis, primary care management appropriate. Topical antibiotic (chloramphenicol or ciprofloxacin), hygiene counselling, review if not improving in 7 days.
Scenario 2 — The urgent referral (anterior uveitis):
A 34-year-old man with known ankylosing spondylitis presents with right eye redness, deep aching pain, and sensitivity to light since yesterday. His vision is 'slightly misty'. No discharge. This is his third episode in two years, always in the right eye.
- Pattern: unilateral, no discharge, deep pain, photophobia, mild vision reduction, recurrent, systemic autoimmune disease.
- Danger signs present: pain + photophobia + vision change.
- Decision: anterior uveitis likely — urgent same-day ophthalmology referral. Do not prescribe antibiotics.
Scenario 3 — The emergency (acute angle-closure glaucoma):
A 62-year-old woman presents to A&E at 9 PM with severe right-sided headache and right eye pain for 3 hours, vomiting twice. She says she can see 'coloured rings' around the overhead light. The eye is red. She is hypermetropic (+4 dioptres on her spectacle prescription).
- Pattern: sudden severe pain, halos around lights, vomiting, hypermetropia, evening onset.
- Danger signs present: severe pain + vision change (halos) + likely corneal oedema.
- Decision: acute angle-closure glaucoma — ocular emergency. Call ophthalmologist immediately. Do not give dilating drops. Document the time of onset and examination findings.
In your skills laboratory, practise transitioning between these three scripts fluently. An examiner will expect you to reach the correct referral decision within 5–7 minutes of starting the history.
SELF-CHECK
Using pinhole in a patient with a red eye and reduced visual acuity — if the pinhole significantly improves the VA, this most likely indicates:
A. The blur is due to corneal oedema from raised IOP
B. The blur is due to a refractive error and the red eye cause is unlikely to be serious
C. The patient has a vitreous haemorrhage
D. The patient has a retinal detachment
Reveal Answer
Answer: B. The blur is due to a refractive error and the red eye cause is unlikely to be serious
The pinhole eliminates peripheral light rays and effectively corrects refractive blur regardless of spectacle correction. If VA improves significantly with pinhole, the blur is predominantly from a refractive cause (e.g. uncorrected myopia) and the red eye itself is unlikely to be causing the visual change — favouring a more benign diagnosis. If VA does NOT improve with pinhole, the blur has an organic cause (corneal oedema, pupillary miosis from uveitis, vitreous pathology, macular disease) and the red eye is more likely to be serious. This is the diagnostic value of the pinhole test in the red-eye consultation.
Self-Assessment
Having worked through the history template, the cause framework, and the three simulated scenarios, assess your own competency against the OP3.1 standard. A final-year MBBS student should be able to: (1) recite the five danger signs without hesitation; (2) name at least three causes in each anatomical compartment; (3) take a complete ophthalmic history in a simulated patient within 5–7 minutes; (4) correctly classify a presented scenario as 'reassure and treat' or 'urgent referral'; (5) identify the one scenario where a wrong decision has life-blinding consequences (acute angle-closure glaucoma). Self-assessment at this stage is a metacognitive checkpoint — not just 'do I know the facts' but 'can I apply them reliably under the time and ambiguity pressure of a real consultation?' The self-test questions below are designed to probe application rather than recall: they present clinical patterns and ask for a clinical decision, mirroring the format of the OP3.1 OSCE station. If you find you can answer the recall questions fluently but hesitate on the decision questions, your preparation gap is at the integration level — return to the pattern-recognition and danger-sign sections and practise the decision tree again before your skills laboratory session.
For self-testing, try the following:
- Given: watery discharge, follicular reaction, preauricular lymph node, URTI 5 days ago — what is the most likely diagnosis?
- Given: unilateral, severe pain, halos, vomiting, fixed mid-dilated pupil, hypermetrope — what is your immediate action?
- Given: bilateral, ropy mucous discharge, intense itching, seasonal onset — what additional questions confirm your diagnosis?
If you cannot answer all three confidently, re-read the Pattern Recognition section before your skills laboratory session.