Page 20 of 27
OP3.7 | Topical Ocular Medication Instillation and Patient Counselling — SDL Guide
Learning Objectives
- Demonstrate the correct technique of instillation of eye drops and eye ointments under supervision
- Explain the pharmacokinetic basis of nasolacrimal occlusion and its importance for reducing systemic side effects
- Counsel patients on the correct self-instillation technique, compliance with timing, storage, and not sharing eye drops
- State the specific systemic risks of topical timolol and topical corticosteroids and the counselling required
INSTRUCTIONS
Topical ophthalmic medications are the mainstay of treatment for the majority of eye conditions managed in primary and secondary care — conjunctivitis, glaucoma, uveitis, dry eye, and post-operative care all rely on patients instilling drops or ointments correctly at home. The problem is that most patients instil eye drops incorrectly: they touch the bottle tip to the eye, squeeze the drops directly onto the cornea (causing reflex blinking and loss), or fail to occlude the nasolacrimal duct — allowing systemic absorption that can cause serious adverse effects. The OP3.7 competency requires you to demonstrate the technique yourself AND to counsel patients on how to self-administer correctly.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 3: Pharmacology of Drugs used in Ophthalmology (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 6: Applied Pharmacology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 65-year-old retired teacher with primary open-angle glaucoma has been prescribed timolol 0.5% eye drops twice daily for the past six months. At a routine visit, his IOP is not adequately controlled. On reviewing with him, you discover that he has been instilling the drops correctly and on time. You ask him to demonstrate — and you observe that after instilling each drop, he immediately squeezes his eye tightly shut and blinks rapidly. He has not heard of nasolacrimal occlusion. His wife, who accompanies him, mentions he has been having 'breathing difficulties' that started three months ago and has been told he has 'some kind of new lung condition.' Could his eye drops be the cause — and could the problem be solved with a technique change rather than a change of drug?
WHY THIS MATTERS
The seemingly simple act of instilling an eye drop is one of the most frequently misperformed self-care tasks in medicine. Studies show that up to 70% of patients do not instil eye drops correctly — they contaminate the bottle tip, instil drops into the wrong place, blink them out immediately, or fail to apply nasolacrimal occlusion. The consequences range from therapeutic failure (the glaucoma progresses) to systemic harm (timolol-induced bronchospasm, steroid-induced adrenal suppression from high-dose preservative-free dexamethasone in a neonatal eye). The NMC OP3.7 competency requires you to demonstrate the technique under supervision and to counsel patients — because in many settings, the doctor who prescribes the eye drop is also the first person to demonstrate how to use it.
RECALL
Recall from your pharmacology module that the bioavailability of a topically applied drug depends on how much drug reaches the target tissue. For ophthalmic drops, the target is the intraocular tissues, reached by diffusion across the corneal epithelium. Only a fraction of each instilled drop reaches the intraocular compartment — most either overflows onto the cheek or is drained via the nasolacrimal duct into the nasopharynx, where it is absorbed through the highly vascular nasal mucosa directly into the systemic circulation, bypassing first-pass hepatic metabolism. This makes nasolacrimal absorption pharmacokinetically similar to intravenous delivery for some drugs — explaining why a 'local' eye drop can cause systemic cardiac or pulmonary effects. Also recall the anatomy of the lacrimal drainage system: the lacrimal puncta (one on each lid margin, at the medial end) drain into the lacrimal canaliculi, then the lacrimal sac, then the nasolacrimal duct into the inferior meatus of the nasal cavity.
Why Correct Drop Instillation Technique Matters
Eye drops appear simple — a small bottle, a liquid, and an eye. In practice, they represent a precision drug delivery system requiring correct technique to achieve therapeutic drug levels at the ocular target while minimising systemic exposure. Two consequences of incorrect technique are therapeutically important enough to be specifically tested at the MBBS level.
Consequence 1 — Therapeutic failure: When a patient blinks rapidly after instillation, squeezes the eye tightly (causing nasolacrimal pump activation), or places the drop directly onto the cornea (which triggers an immediate blink reflex and ejection of the drop), the drug is washed out of the conjunctival sac within seconds. The conjunctival sac can only hold approximately 7–10 microlitres of fluid; a standard eye drop contains 30–50 microlitres — meaning most of the drop volume overflows even with perfect technique. If technique is poor, essentially none of the drug is retained. A patient who 'takes their glaucoma drops every day' but blinks them away may have no better IOP control than if they took no drops at all.
Consequence 2 — Systemic side effects from nasolacrimal absorption: Drugs absorbed via the nasolacrimal duct bypass hepatic first-pass metabolism and enter the systemic circulation at near-intravenous concentrations. The two most clinically important examples are:
- Timolol eye drops (beta-blocker for glaucoma): systemic absorption can cause bradycardia, heart block, and — critically — bronchospasm in patients with asthma or COPD. This is why timolol eye drops are contraindicated in reactive airways disease, even though they are topical. The nasolacrimal occlusion technique reduces this systemic exposure by preventing the drug from entering the nasolacrimal drainage system.
- Topical corticosteroids in infants and neonates: high-potency topical steroids (e.g., dexamethasone) used for post-operative inflammation or uveitis in neonates can be absorbed systemically in quantities sufficient to suppress the hypothalamic-pituitary-adrenal (HPA) axis — the same risk as systemic steroids.
These two consequences establish why instillation technique is a patient-safety issue, not merely a comfort issue.
The Conjunctival Sac: Anatomy and the Drop Volume Problem
Understanding the anatomy and physiology of the ocular surface pharmacokinetics explains why the instillation technique is designed the way it is. This understanding also prevents the common patient error of instilling multiple drops simultaneously thinking 'more is better.'
The conjunctival sac at rest contains approximately 7–10 microlitres (μL) of the basal tear film. A standard ophthalmic drop from a conventional bottle contains 30–50 μL per drop. This means that when a standard drop is instilled correctly into the lower fornix, it immediately overfills the available space — the excess (approximately 20–40 μL) overflows onto the eyelid and cheek, or is rapidly drained into the nasolacrimal system. Within 1–2 minutes, the conjunctival sac returns to its baseline tear volume through drainage and evaporation.
Key implications:
1. One drop is sufficient — instilling a second drop immediately after the first provides no additional therapeutic benefit (the first drop has already saturated the sac volume) and wastes medication. Some patients instil two or three drops per dose in the mistaken belief that more drops equal better effect.
2. Waiting ≥5 minutes between two different eye drops is mandatory when multiple medications are prescribed — otherwise the second drop immediately washes out the first before it can be absorbed. A patient prescribed timolol + travoprost (two antiglaucoma drops) must wait at least 5 minutes between the two.
3. Drop placement in the lower fornix — NOT directly onto the cornea — minimises the blink reflex. The cornea is the most densely innervated tissue in the body; a drop landing on the cornea triggers an immediate, forceful blink reflex that expels the drop. The lower fornix (the pocket formed by pulling down the lower lid) is a relatively insensitive area where the drop can pool without triggering blink.
The nasolacrimal drainage pathway exits via the lacrimal puncta at the medial canthus. Applying finger pressure at the medial canthus (nasolacrimal occlusion, NLO) for 1–2 minutes after drop instillation physically prevents drug from entering the nasolacrimal duct, maximising ocular retention and minimising systemic absorption. This is the single most important technique modification for high-risk medications (timolol, topical steroids).
SELF-CHECK
A 68-year-old man is prescribed timolol 0.5% eye drops twice daily for glaucoma. He has a history of mild asthma managed with a salbutamol inhaler. The most important counselling point before he starts the drops is:
A. Instil the drops directly onto the cornea to maximise absorption
B. Perform nasolacrimal occlusion for 1-2 minutes after each instillation and monitor for worsening breathing difficulty — timolol may be contraindicated in his asthma
C. Instil two drops per dose to ensure adequate drug levels
D. Apply eye ointment before the timolol drop to maximise retention
Reveal Answer
Answer: B. Perform nasolacrimal occlusion for 1-2 minutes after each instillation and monitor for worsening breathing difficulty — timolol may be contraindicated in his asthma
Timolol (a non-selective beta-blocker) is absorbed via the nasolacrimal duct into the systemic circulation, where it can cause bronchoconstriction in patients with reactive airways disease (asthma, COPD) by blocking beta-2 adrenoceptors in the bronchi — even though it is given as a topical eye drop. Nasolacrimal occlusion for 1-2 minutes after each instillation reduces systemic absorption and is the most important technique modification for this patient. However, the prescriber must also weigh whether timolol is appropriate at all given his asthma history — a selective beta-1 blocker (betaxolol) or a prostaglandin analogue (latanoprost) may be safer. Instilling drops onto the cornea, double-dosing, and using ointment first are all incorrect technique.
Step-by-Step Drop Instillation Technique
The correct technique for instilling eye drops should be practised in the skills laboratory until it is fluent enough to demonstrate to a patient. The steps below represent the evidence-based standard for correct topical drug delivery, as used in the skills assessment for OP3.7. The reason fluency matters as much as accuracy is that the counselling element of OP3.7 — demonstrating the technique to a patient and ensuring they can replicate it — requires the doctor to perform the procedure smoothly enough that each step is visible and naratable in real time. A student who can recite the seven steps but hesitates between them, or who inadvertently touches the bottle tip to the eyelid while trying to remember the next instruction, will not effectively teach the technique to the patient. Practise the procedure until the hand movements are automatic: the preparation steps (checking label, shaking suspensions, warming the bottle) should take no conscious effort, freeing your attention for the precise placement of the drop into the lower fornix pocket and the nasolacrimal occlusion manoeuvre that determines whether the technique is therapeutically sound.
Preparation:
1. Wash hands thoroughly with soap and water (or alcohol gel) before handling an eye drop bottle — contamination of the bottle tip with skin flora is a common cause of ocular infection in patients using long-term drops.
2. Check the label: drug name, concentration, which eye (right/left/both), frequency.
3. If the bottle contains a suspension (identifiable by the label instruction 'SHAKE BEFORE USE' or by the visible white sediment — e.g., prednisolone acetate 1%), shake gently for 5–10 seconds before use.
4. Warm the bottle slightly by holding it in the palm for 30–60 seconds — cold drops trigger a more pronounced blink reflex.
Positioning:
5. Tilt the head backward (lying supine is ideal for self-instillation; seated with head tilted back is acceptable).
6. Look upward.
Drop instillation:
7. With the non-dominant hand, gently pull down the lower eyelid using a clean finger to create a pocket (lower fornix).
8. Hold the bottle between the thumb and index finger of the dominant hand, tip pointing downward, approximately 1–2 cm above the eye — do not let the bottle tip touch the eye, eyelashes, or eyelid (contamination risk).
9. Squeeze gently to release ONE drop into the lower fornix pocket — aim for the pocket, not the cornea.
10. Close the eye gently — do NOT squeeze tightly (tight closure activates the lacrimal pump, rapidly draining the drop) and do NOT blink repeatedly.
Nasolacrimal occlusion:
11. Press the index finger gently on the inner corner of the eye (the medial canthus, at the lacrimal punctum) immediately after closing the eye — this occludes the punctum and prevents drainage.
12. Maintain gentle pressure for 1–2 minutes.
13. Keep the eye gently closed during this time.
After instillation:
14. Gently wipe away any overflow from the cheek with a clean tissue.
15. Do not rub the eye.
16. Replace the bottle cap immediately without touching the tip.
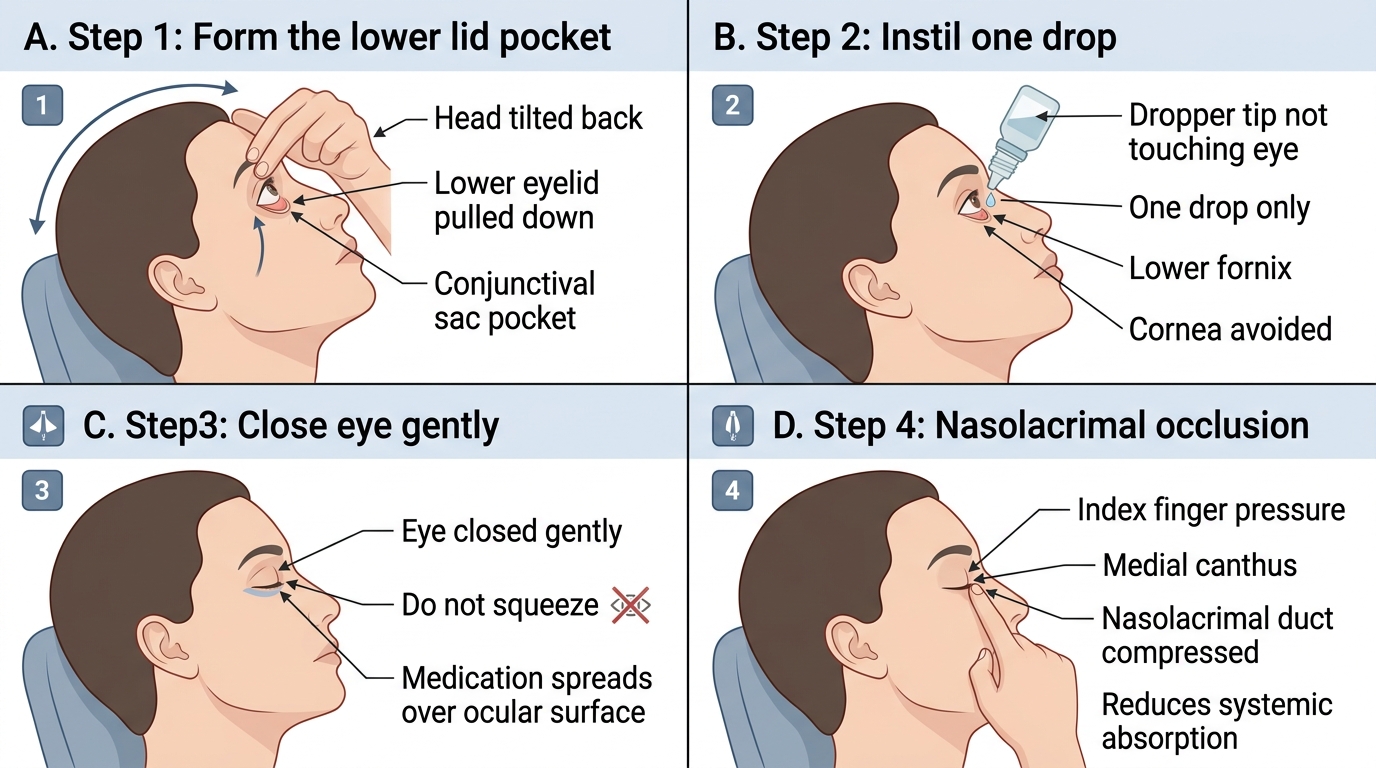
Correct Eye Drop Instillation Technique