Page 11 of 33
OP4.4 | Corneal Opacity: Identification, Grading and Management — SDL Guide
Learning Objectives
- Identify corneal opacity on clinical examination and describe its location, size, and depth
- Differentiate the three grades of corneal opacity: nebula, macula, and leukoma
- Describe the pathophysiological basis of corneal scar opacity
- Enumerate the management modalities of corneal opacity and their indications
- Select the appropriate management based on depth, grade, location, and endothelial status
INSTRUCTIONS
A white spot on the cornea is one of the most common findings in an ophthalmology outpatient department, particularly in India where post-infective corneal scars are epidemic. Grading the opacity — nebula, macula, or leukoma — and assessing its depth and position relative to the visual axis are the two skills that determine management. This module builds those skills systematically.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old woman from rural Andhra Pradesh is brought to your clinic by her son. She has a prominent white opacity on her left cornea, visible from across the room. She says she had a 'bad eye infection' twenty years ago after getting a thorn in her eye — treated locally with 'antibiotic ointment' but it did not heal well. Her best-corrected visual acuity in the left eye is counting fingers at 1 metre. When you ask her why she waited twenty years, she says nobody told her anything could be done. Your task: characterise this opacity, assess whether her endothelium is healthy enough for surgery, and determine what can be offered.
WHY THIS MATTERS
Corneal opacity from post-infective scarring is the second leading cause of avoidable monocular blindness in India. Unlike cataract, which can be removed without destroying the lens architecture, corneal scarring replaces the precise collagen lattice of the stroma with irregular fibrous tissue that scatters light permanently. Yet this condition is now surgically treatable — keratoplasty has transformed the prognosis of corneal blindness in centres with eye banks. The ophthalmologist's role is to assess the opacity accurately and connect the patient to the right management, whether optical, laser, or surgical.
RECALL
From SDL 1: corneal transparency depends on the Maurice lattice — regular collagen fibril spacing creating destructive interference. Scar tissue replaces this with randomly arranged fibrous collagen, which scatters light constructively and appears white. From SDL 3: fungal and bacterial keratitis are the leading causes of post-infective corneal scars in India. Recall that the endothelium is assessed by specular microscopy and that a cell count below ~500 cells/mm² signals functional failure. Recall that the pinhole test improves refractive but not organic causes of visual impairment — a useful tool to distinguish opacity-related VA loss from refractive error.
Clinical Presentation and Identification of Corneal Opacity
Patients with corneal opacity present with visual impairment (proportional to the opacity's position and density), a visible white area in the eye noticed by themselves or others, and occasionally a cosmetically concerning appearance. The visual impairment depends critically on two factors: whether the opacity overlies the visual axis (the pupillary area), and how dense the opacity is. A dense peripheral leukoma may cause no visual symptoms at all; a faint central nebula may dramatically reduce corrected visual acuity even when the opacity appears small. This spatial relationship — position relative to the optical axis rather than absolute size — is the single most important determinant of visual consequence. A 1 mm opacity dead-centre on the pupillary axis blocks more functionally useful light than a 5 mm opacity at the periphery where no light normally enters the pupil. Additionally, even opacities that do not fully block the visual axis cause irregular astigmatism by distorting the anterior corneal surface, leading to ghost images, monocular diplopia, and glare — symptoms that are not captured by simple Snellen acuity measurement. Patients sometimes describe their vision as 'foggy' or 'dirty' through the affected eye even when acuity is relatively preserved. Understanding this symptom profile allows the clinician to elicit a complete history before examination.
Clinical identification requires a systematic slit-lamp examination:
1. Torch examination in good light: A leukoma is visible even with a torch. A nebula may only be apparent under focused illumination.
2. Slit-lamp with direct focal illumination: Move the slit beam through the opacity — note its anterior-posterior extent (depth in the stroma), whether it extends to the posterior corneal surface (involving Descemet's/endothelium), and whether the stroma surrounding the opacity is clear.
3. Retroillumination: Use light reflected from the iris or fundus — opacity appears dark against the orange-red reflex. Useful for subtle nebulae and assessing the transparency of the remainder of the cornea.
4. Note whether the iris is visible through the opacity: This is the bedside grading criterion — visible iris details = nebula or macula; iris invisible = leukoma.
5. Record the position: Central (on visual axis), paracentral, or peripheral. Map the clock-hour position and approximate diameter in millimetres.
Additional important observations: vascularisation (vessels in or around the opacity suggest previous infection or inflammation), thinning (post-ulcer ectasia), and the state of the surrounding cornea (clear or itself involved).
Pathophysiology of Corneal Scar Formation
Understanding why corneal scars are white requires revisiting the Maurice lattice theory from SDL 1. Normal corneal transparency depends on the regular spacing of Type I collagen fibrils (~60 nm centre-to-centre) maintained by keratan sulphate proteoglycans. Any injury that penetrates into the stroma — whether from infection (bacterial or fungal ulcer), trauma, chemical burn, or surgery — triggers a wound-healing response that, unlike skin healing, cannot restore this precise architecture.
The sequence of corneal wound healing in the stroma is as follows: stromal keratocytes are activated to become myofibroblasts by TGF-β released from damaged epithelial cells. Myofibroblasts synthesise collagen rapidly, but in a disorganised, irregular arrangement rather than the precise orthogonal lattice of normal stroma. This irregular collagen arrangement destroys the destructive interference mechanism of the Maurice lattice — instead of cancelling, scattered light adds constructively, and the healed area appears white/opaque. Additionally, the scar tissue is vascularised during the healing phase (new vessels growing from the limbus to support the healing tissue), though these may partially regress. The scar also contains inflammatory cells, new collagen that differs in fibril diameter from normal stroma, and lacks the normal keratocyte density. The result is permanent opacity unless the scarred tissue is surgically removed and replaced with donor tissue.
The depth of the scar is determined by how deeply the insult penetrated: superficial infections affecting only the epithelium and Bowman's layer heal without permanent opacity (epithelium regenerates; Bowman's heals by superficial scar, sometimes with mild anterior stromal haze). Infections or trauma penetrating the middle or posterior stroma leave permanent dense leukoma. If Descemet's membrane and the endothelium are involved (e.g., perforating corneal ulcer, adherent leukoma), the endothelial pump is also impaired, adding corneal oedema to the opacity.
SELF-CHECK
A 35-year-old man has a corneal opacity following a resolved bacterial ulcer. On slit-lamp examination you can see iris details through the opacity but it is clearly visible without special illumination. What is the correct grade of this opacity?
A. Nebula — only visible in oblique illumination
B. Macula — visible in direct illumination, iris details still visible through it
C. Leukoma — dense white, iris details not visible
D. Adherent leukoma — iris adherent to the posterior corneal surface
Reveal Answer
Answer: B. Macula — visible in direct illumination, iris details still visible through it
A macula (from Latin for 'spot') is a moderately dense corneal opacity visible in direct illumination, but iris details remain visible through it. A nebula is so faint it requires oblique illumination to see. A leukoma is dense enough to obscure iris details completely. Adherent leukoma specifically involves iris-to-cornea adhesion, which is not described here.
Grading and Classification of Corneal Opacity
The traditional grading of corneal opacities into three density categories — nebula, macula, and leukoma — remains the standard clinical classification and is used universally in examination and practice. Each term derives from Latin and describes the visual appearance.
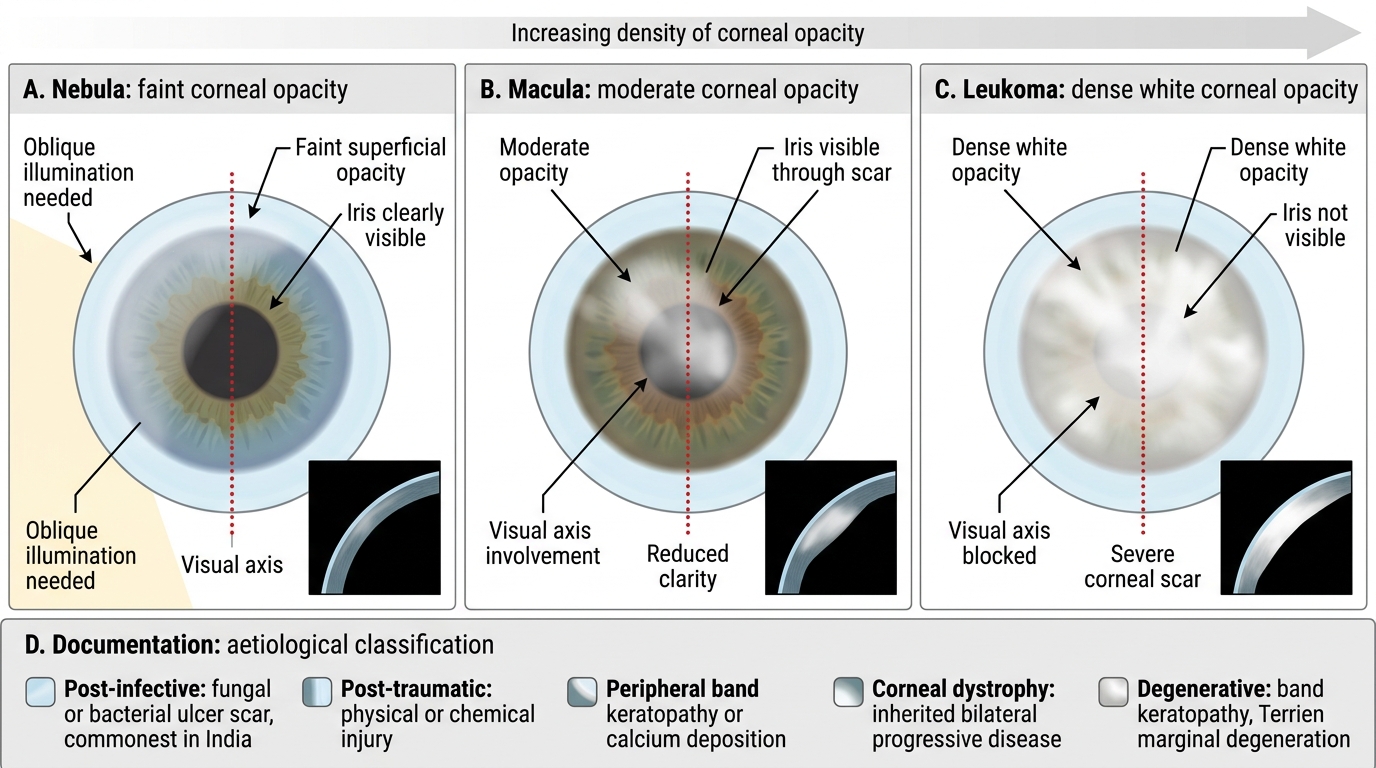
Nebula (Latin: cloud) is the least dense grade. It appears as a faint, greyish haze that is often invisible to the naked eye and requires oblique illumination or slit-lamp to be identified. The iris and its details are clearly visible through a nebula. Most superficial nebulae result from healed epithelial or mild Bowman's layer disease. They may cause subtle visual disturbance (irregular astigmatism) but rarely significant VA reduction. In young children, even a faint central nebula can cause meridional amblyopia — an important reason to identify and manage corneal opacities in children early.
Macula (Latin: spot) is moderately dense. It is visible with a torch in good illumination, and the iris is discernible through it — but iris details (crypts, collarette) are difficult to make out. It represents deeper stromal involvement — typically mid-stromal scar. A central macula causes significant VA reduction; a peripheral macula may be visually asymptomatic.
Leukoma (Greek: white) is the densest grade — a dense white opacity through which the iris cannot be seen. It indicates deep stromal involvement, often extending to or through Descemet's membrane. It may be associated with thinning of the cornea at the scarred area. A central leukoma on the visual axis typically reduces VA to CF (counting fingers) or HM (hand movements) at the affected eye.
Adherent leukoma (leukoma adherens) is a specific variant in which the iris has become adherent to the posterior surface of the dense corneal scar, typically following corneal perforation (where the iris plugged the perforation and healed adherent to it). On examination, the iris appears distorted and pulled towards the opacity (corectopia — displaced pupil). This is a complex situation for keratoplasty because the iris adhesion must be managed during surgery.
Grades of Corneal Opacity: Nebula, Macula and Leukoma
Classification by aetiology (for documentation):
- Post-infective: fungal or bacterial ulcer scar — commonest in India
- Post-traumatic: physical or chemical trauma
- Peripheral band keratopathy or calcium deposition: systemic or local causes
- Corneal dystrophy: inherited bilateral progressive disease (Fuchs', lattice, granular, macular dystrophies)
- Degenerative: band keratopathy, Terrien's marginal degeneration