Page 15 of 33
OP4.5 | Dry Eye Disease — SDL Guide (Part 2)
Clinical Investigations for Dry Eye
Dry eye investigations are designed to quantify tear production, assess tear film stability, and detect corneal surface damage from insufficient lubrication. No single test is sufficient — a combination is used in clinical practice.
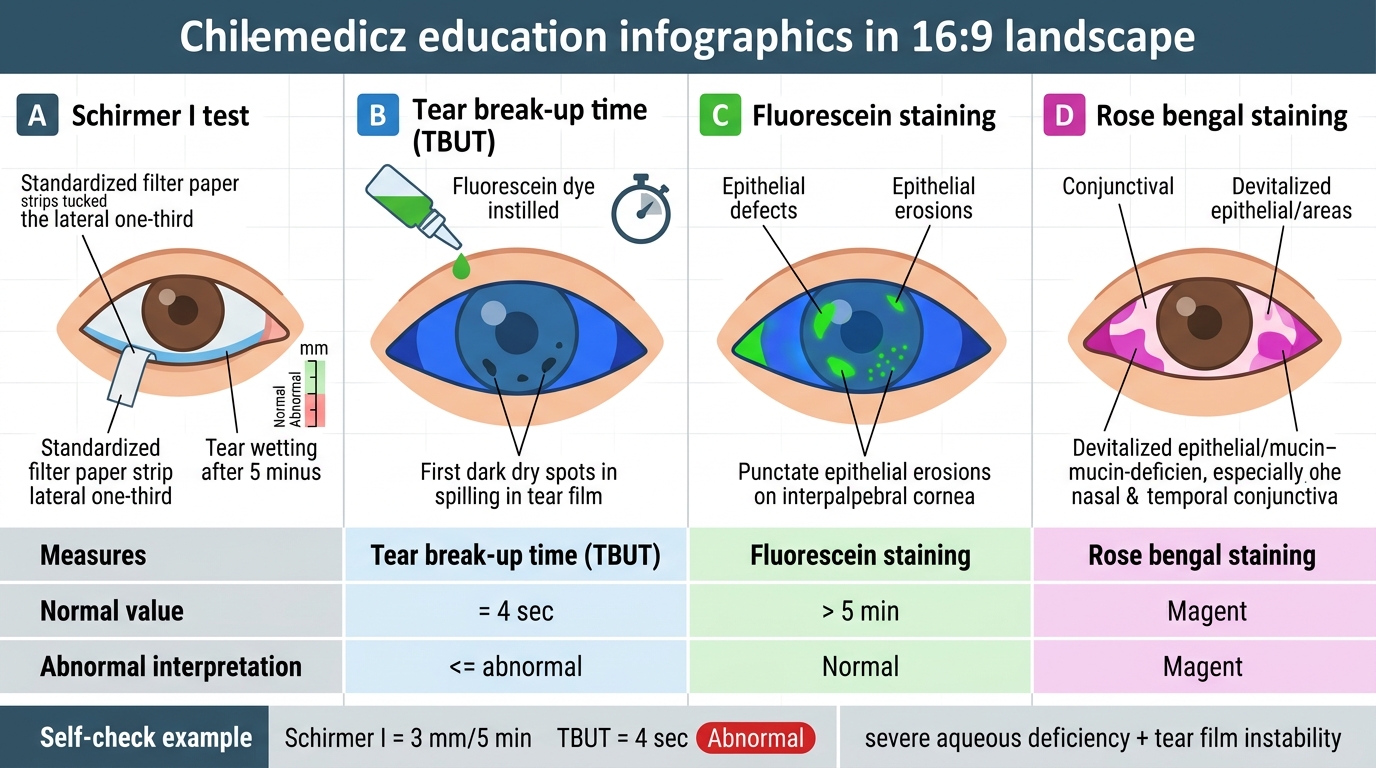
Schirmer's test measures the rate of aqueous tear secretion by placing a standardised strip of Whatman No. 41 filter paper (5 mm wide, 35 mm long) over the lower eyelid margin at the junction of the middle and lateral thirds. The strip is read at 5 minutes and the length of wetting measured in millimetres.
Schirmer I test (performed WITHOUT topical anaesthesia): measures both basal (lacrimal gland resting secretion) and reflex (trigeminal-stimulated) secretion. Normal: ≥10 mm at 5 minutes. Borderline: 5–9 mm. Severely reduced: <5 mm (indicates significant aqueous deficiency). This is the most commonly used clinical test.
Schirmer II test (after topical anaesthesia, with nasal mucosal stimulation): selectively stimulates reflex secretion only, by introducing a nasal stimulus (cotton bud in the nostril). It is used to determine whether the patient has any residual reflex tear secretion capacity — useful in the investigation of Sjögren's syndrome.
Tear film break-up time (TBUT): Fluorescein is instilled into the lower fornix; the patient blinks once and then keeps the eye open. Under cobalt blue slit-lamp illumination, the observer watches the fluorescein-stained tear film for the first appearance of a dark spot or streak (a 'break' where the tear film has thinned and the epithelium is exposed). The time from the last blink to this first break is the TBUT. Normal: ≥10 seconds. Abnormal: <10 seconds (indicates tear film instability, typical of EDE/MGD). A very short TBUT (<5 sec) suggests significant lipid layer deficiency.
Fluorescein staining of the cornea: Rose bengal or fluorescein dye is instilled and the corneal surface examined under cobalt blue light. Fluorescein pools in epithelial defects. In DED, fine punctate staining is seen in the interpalpebral zone (the corneal area exposed between eyelids). The Oxford grading scheme grades from 0 (no staining) to V (very heavy staining). Lissamine green dye (analogous to rose bengal but less irritating) stains devitalised epithelial cells of the cornea and conjunctiva.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Dry Eye Investigations: Key Comparisons
SELF-CHECK
A patient with suspected dry eye undergoes the following tests: Schirmer I test = 3 mm at 5 minutes; TBUT = 4 seconds. Which of the following correctly interprets these results?
A. Schirmer I is borderline (3 mm is 5-9 mm range); TBUT is normal (≥10 sec)
B. Both tests are abnormal: Schirmer I <5 mm indicates severe aqueous deficiency; TBUT <10 sec indicates tear film instability
C. Schirmer I is normal (≥10 mm); TBUT is abnormal but not significant unless >15 seconds
D. Schirmer I of 3 mm is normal for elderly patients; only TBUT <5 sec is diagnostic of DED
Reveal Answer
Answer: B. Both tests are abnormal: Schirmer I <5 mm indicates severe aqueous deficiency; TBUT <10 sec indicates tear film instability
Schirmer I of 3 mm at 5 minutes is severely reduced (normal ≥10 mm; <5 mm = severe aqueous deficiency). TBUT of 4 seconds is markedly abnormal (normal ≥10 sec; <10 sec = unstable tear film). Together they indicate both aqueous-deficient and evaporative components of dry eye disease. There are no age-adjusted Schirmer norms that make 3 mm acceptable in an elderly patient — 3 mm is severely reduced at any adult age. The 5-9 mm range is 'borderline', and <5 mm is 'severe'; 3 mm falls in the severe range.
Management of Dry Eye Disease
Management of DED follows a stepwise approach based on disease severity and identified mechanism. The 2017 TFOS DEWS II guidelines recommend a four-step escalation ladder. The fundamental principle underlying this escalation approach is that dry eye disease is not a single pathological entity but a spectrum: the mildest end involves transient aqueous insufficiency or instability that responds to simple lubrication and environmental change, while the severe end involves irreversible lacrimal gland destruction (as in Sjögren's syndrome or Stevens-Johnson syndrome sequelae) that requires biological or surgical intervention. Matching the treatment to the mechanism — aqueous-deficient versus evaporative — is as important as matching it to the severity level. Prescribing aqueous lubricants alone to a patient whose primary problem is meibomian gland dysfunction will fail to address the lipid deficiency causing rapid evaporation; conversely, prescribing warm compresses to a patient with primary Sjögren's-related aqueous deficiency is insufficient. A second key principle is that chronic inflammatory DED — evident from conjunctival hyperaemia, goblet cell loss on impression cytology, and high tear MMP-9 — requires anti-inflammatory therapy (cyclosporine or corticosteroids) in addition to lubricants, not instead of them. Without addressing the inflammatory cycle, lubricants provide only temporary symptomatic relief while the lacrimal gland dysfunction continues to worsen.
Step 1 (Mild to Moderate DED):
- Artificial tears / lubricants: The mainstay of initial management. Options include carboxymethylcellulose (CMC) 0.5%, sodium hyaluronate, carbomer gels (longer retention), lipid-containing emulsion drops (for MGD/EDE). Preservative-free formulations are essential for patients using drops more than 4 times daily — preservatives (especially benzalkonium chloride) are toxic to the corneal epithelium with frequent use.
- Environmental modification: Humidifier in dry offices, reduce AC direct airflow towards the face, reduce screen time, take regular blink breaks.
- Dietary omega-3 fatty acid supplementation: Evidence supports modest benefit (1–2 g/day); reduces meibomian lipid viscosity, reduces inflammatory cytokines.
- Treat underlying lid disease: For MGD/blepharitis — warm compresses (melts inspissated meibum) + lid scrubs/hygiene + topical azithromycin or doxycycline (reduces meibomian lipase activity).
Step 2 (Moderate DED not responding to Step 1):
- Topical cyclosporine 0.05% (Restasis): An immunomodulatory agent that reduces T-cell-mediated inflammation in the lacrimal gland and conjunctiva. It does not sting or suppress systemic immunity. Effect develops over 3–6 months of use. Indicated for moderate-severe DED with evidence of inflammatory component.
- Topical lifitegrast 5% (Xiidra): A lymphocyte function-associated antigen-1 (LFA-1) antagonist; reduces T-cell migration into the ocular surface. Approved for DED in several countries.
- Short-term topical corticosteroids: Loteprednol or fluorometholone — for acute flares of inflammatory DED; not for long-term use due to glaucoma and cataract risk.
- Punctal occlusion: Silicone punctal plugs inserted into the lacrimal puncta to reduce tear drainage and retain the limited aqueous in the tear lake. Useful when artificial tears provide inadequate relief. Reversible (plugs can be removed).
Step 3 (Severe or refractory DED):
- Autologous serum eye drops: Patient's own serum (diluted 20% in normal saline) contains growth factors (EGF, TGF-β, vitamin A) that support epithelial healing; used in severe Sjögren's or neurotrophic cases where lubricants and cyclosporine are insufficient.
- Scleral contact lenses: Large-diameter rigid lenses that vault over the cornea and maintain a fluid reservoir, providing continuous corneal hydration — particularly effective in Stevens-Johnson syndrome aftermath and severe Sjögren's.
- Moisture chamber spectacles: Side shields that trap humid air around the eye, reducing evaporative loss.
- Tarsorrhaphy: Surgical partial closure of the eyelid margins — reduces evaporative surface and protects the cornea in severe lagophthalmos or neurotrophic dry eye.
Step 4 (Severe with corneal complications — scarring, filaments, persistent epithelial defects):
- Amniotic membrane transplantation for persistent epithelial defects.
- Keratoplasty for corneal scarring from DED complications (rare).
CLINICAL PEARL
Paradoxical reflex tearing — a patient who 'cries constantly' — is often dry eye. The gritty or burning sensation from an unstable tear film triggers lacrimal reflex secretion, which is aqueous-rich but unstable. The correct clinical response is NOT to reassure the patient that they 'can't be dry if they're tearing' — it is to perform TBUT and Schirmer's. The hook patient's TBUT of 6 seconds confirms evaporative DED; her Schirmer's of 14 mm confirms normal aqueous production. The diagnosis is evaporative dry eye from meibomian gland dysfunction — managed with warm compresses and lid hygiene, not simply more aqueous lubricants.
Clinical Decision-Making in Dry Eye
The management of DED is mechanism-matched. The clinical decision pathway starts with identifying whether the primary mechanism is aqueous deficiency, evaporative, or mixed.
A low Schirmer's test (<10 mm, particularly <5 mm) with a normal TBUT suggests aqueous-deficient DED → investigate for Sjögren's (anti-Ro/SSA, anti-La/SSB, salivary gland function), review all medications for secretion suppressors, and consider cyclosporine 0.05% as anti-inflammatory treatment.
A low TBUT (<10 sec) with near-normal Schirmer's test suggests evaporative DED from MGD → examine meibomian gland orifices on slit-lamp (capped, irregular, thickened with white obstructed meibum), warm compresses, lid hygiene, topical azithromycin, omega-3.
Both low Schirmer's AND low TBUT → mixed mechanism; both approaches required.
The severity of corneal staining (Oxford grading) guides escalation. A patient with grade III/IV punctate keratitis is a candidate for cyclosporine and possibly punctal occlusion, even if their symptoms have not yet escalated.
Special scenarios:
- Sjögren's syndrome with severe ADDE: cyclosporine + preservative-free lubricants + punctal occlusion + autologous serum if refractory. Rheumatology co-management for systemic disease.
- Lagophthalmos (facial nerve palsy): tape eyelids shut at night, moisture chamber spectacles, lubricating ointment at bedtime, consider tarsorrhaphy if corneal exposure is threatening vision.
- Medication-induced DED: Review and if possible discontinue the offending agent (antihistamine, antidepressant, beta-blocker). Substitute with DED-safe alternatives where clinically possible.
Self-Assessment: Dry Eye Disease
Consolidate your understanding with these scenarios.
Scenario 1: A 60-year-old woman with rheumatoid arthritis on methotrexate presents with burning and gritty eyes for 2 years. Schirmer I = 4 mm bilaterally. TBUT = 11 seconds. Rose bengal stains the conjunctiva moderately. Anti-Ro antibodies are positive. What is the classification of her DED and the management priorities? Answer: Aqueous-deficient DED (ADDE), secondary Sjögren's syndrome (in context of RA + positive anti-Ro). TBUT is normal, confirming primarily aqueous deficiency rather than evaporative. Management: preservative-free artificial tears frequently, topical cyclosporine 0.05%, punctal occlusion if inadequate response, ophthalmology + rheumatology co-management.
Scenario 2: A 35-year-old software engineer presents with burning eyes worsening after 4-hour screen sessions. TBUT = 5 sec. Schirmer I = 15 mm. Slit-lamp shows inspissated, irregular meibomian gland orifices and flaky debris at the lid margins. What is the classification and management? Answer: Evaporative DED from MGD/blepharitis. Normal aqueous production (Schirmer 15 mm), unstable tear film (TBUT 5 sec). Management: warm compresses daily (2 mins, lid massage), lid scrubs, topical azithromycin 1% ointment at lid margin, oral omega-3, advise 20-20-20 rule for screen use (every 20 minutes, look 20 feet away for 20 seconds to normalise blink rate).
Scenario 3: Name all three layers of the tear film, their secreting source, and what happens to the tear film when each layer is deficient. Check: Lipid (meibomian glands) → deficient: rapid evaporation (EDE). Aqueous (main lacrimal + accessory glands) → deficient: insufficient volume (ADDE). Mucin (goblet cells) → deficient: aqueous doesn't spread uniformly, localised drying despite normal aqueous output (mucin-deficient DED).