Page 21 of 33
OP4.7 | Keratoplasty: Types and Indications — SDL Guide (Part 2)
Graft Rejection: Types, Signs and Emergency Management
Graft rejection is a T-lymphocyte-mediated immune response against donor corneal antigens, occurring in a sensitised host who has mounted a cellular immune response to donor HLA class I and class II antigens presented on donor stromal keratocytes and endothelial cells. The immunological basis is the same as solid organ transplant rejection — alloreactive host CD4+ and CD8+ T cells recognise the graft as foreign and mount a destructive immune attack — but the cornea's relative immune privilege (avascularity, absence of lymphatic drainage, anterior chamber-associated immune deviation) means that ungrafted corneas rarely undergo rejection in the way that vascularised organs do. Once a corneal graft is placed, however, host blood vessels grow into the wound and provide an afferent arc for sensitisation; once the host immune system is primed against donor antigens, subsequent rejection episodes become increasingly rapid. The risk of rejection is highest in vascularised host corneas (because pre-formed blood vessels provide immune access directly), regrafts (the host is already sensitised from prior graft antigens), and cases with pre-existing inflammation or uncontrolled glaucoma. The earliest post-operative period (the first year) carries the highest absolute risk, but — unlike many other transplant types — corneal graft rejection can occur at any time after surgery, including decades later, which is why post-keratoplasty steroid prophylaxis is maintained long-term rather than for a fixed post-operative period.
Provided image
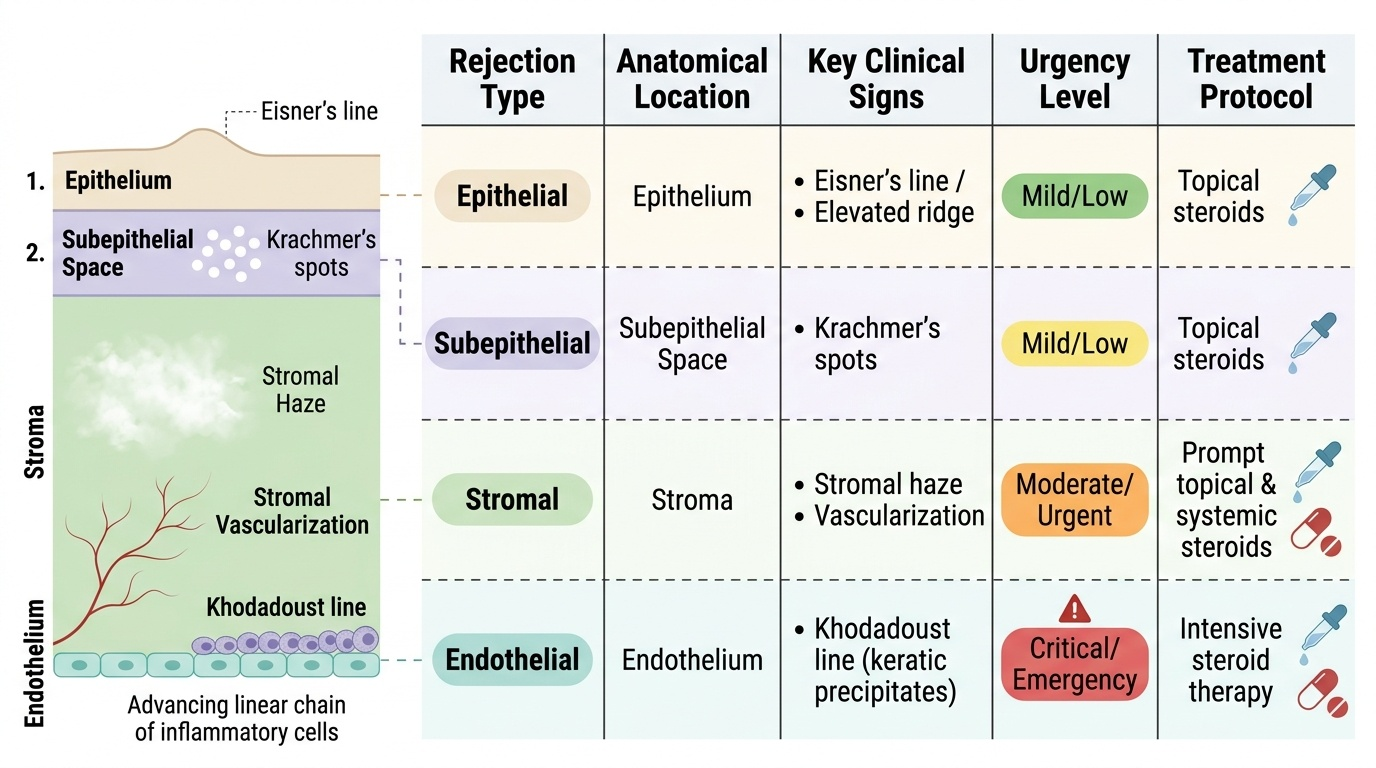
Four types of rejection, each targeting a different corneal layer:
- Epithelial rejection: A faint advancing line of elevated epithelium (Eisner's line) progresses across the donor epithelium. Usually benign and self-limiting; responds readily to topical steroids. Rare and mild.
- Subepithelial rejection (Krachmer's spots): Multiple fine subepithelial infiltrates scattered across the graft, resembling the subepithelial infiltrates of adenoviral keratoconjunctivitis. Respond well to topical steroids.
- Stromal rejection: Diffuse haze within the donor stroma, occasionally with stromal vascularisation. Requires prompt topical and sometimes systemic steroid therapy.
- Endothelial rejection: The most serious form. An advancing line of endothelial keratic precipitates — the Khodadoust line (after Ahmed Khodadoust who described it in 1968) — sweeps across the donor endothelium from the periphery toward the centre. As the line advances, the endothelium behind it is being destroyed, and the stroma behind the line becomes oedematous. If the Khodadoust line reaches the central endothelium, enough endothelial cells are lost to cause irreversible graft failure.
The RSVP mnemonic for graft rejection warning symptoms: Redness, Sensitivity (photophobia), Vision decrease, Pain. Every keratoplasty patient must be taught to present immediately if any of these symptoms occur — endothelial rejection is reversible if treated early but irreversible once graft failure occurs.
Emergency management of endothelial rejection: Topical prednisolone 1% (or dexamethasone 0.1%) every hour (intensive regimen) is the standard treatment, combined with oral prednisolone 1 mg/kg/day in severe cases. The earlier treatment is initiated, the higher the chance of saving the graft. Treatment is continued intensively for days to weeks, then tapered once the Khodadoust line begins to recede and the graft clears.
SELF-CHECK
A 55-year-old woman who underwent penetrating keratoplasty 3 years ago presents with sudden onset pain, redness, and blurred vision in the grafted eye for 2 days. On slit-lamp she has diffuse graft oedema and a line of endothelial keratic precipitates advancing from the periphery toward the centre of the donor button. What is this sign called and what is the IMMEDIATE management?
A. Krachmer's spots — treat with topical lubricants; not urgent
B. Khodadoust line (endothelial rejection) — start topical prednisolone 1% every hour immediately; add oral steroids in severe cases
C. Eisner's line (epithelial rejection) — observe only; most cases resolve spontaneously
D. Corneal ulcer — start topical antibiotics urgently
Reveal Answer
Answer: B. Khodadoust line (endothelial rejection) — start topical prednisolone 1% every hour immediately; add oral steroids in severe cases
The Khodadoust line is the pathognomonic sign of endothelial rejection — a line of endothelial keratic precipitates advancing across the donor endothelium, with stromal oedema behind it. This is a medical emergency: endothelial cells behind the advancing line are being destroyed, and once sufficient endothelium is lost, the graft will fail irreversibly. Immediate treatment with intensive topical prednisolone 1% every hour (plus systemic steroids if severe) is required. Krachmer's spots are subepithelial rejection (less urgent); Eisner's line is epithelial rejection (usually benign). A corneal ulcer would show fluorescein staining of an epithelial defect, not a line of keratic precipitates.
Post-Keratoplasty Complications and Outcomes
Keratoplasty carries a range of short and long-term complications that the surgeon must anticipate and the patient must understand before consenting to surgery.
Intraoperative complications: Suprachoroidal haemorrhage (expulsive haemorrhage) — the most feared intraoperative complication of any open-globe surgery; the choroidal vessels bleed massively as intraocular pressure drops suddenly on opening the eye. Prevention: good IOP control before surgery; management = close the wound immediately.
Early postoperative complications: Wound leak (Seidel test positive), primary graft failure (endothelium already non-functional before transplant, or mechanical damage during surgery), shallow anterior chamber, elevated IOP (from viscoelastic retention), and hyphema.
Intermediate complications (weeks to months): Post-keratoplasty astigmatism — the suture placement and wound healing induce irregular astigmatism, often 3–5 dioptres or more. This is the most common visual complication of PK. Management: selective suture removal (cutting tight sutures to redistribute tension), rigid contact lenses (neutralise irregular astigmatism), or refractive surgery (LASIK, PRK, or excimer laser on a clear stable graft). Graft rejection (described above).
Long-term complications: Late endothelial failure — gradual progressive endothelial cell loss over years, even without overt rejection episodes, eventually leading to graft oedema and failure. Secondary glaucoma — elevated IOP from peripheral anterior synechiae, steroid-induced glaucoma, or angle damage. Requires careful IOP monitoring and treatment. Recurrence of original disease — dystrophies (lattice, granular) can recur in the graft.
Outcomes data: For avascular keratoconus (the best-prognosis indication) — 5-year graft survival approximately 90%. For post-infective leukoma with vascularised cornea — 5-year survival approximately 50–60% (lower due to rejection risk from vessels). For regrafts — progressively lower survival with each subsequent operation.
CLINICAL PEARL
Teach every keratoplasty patient the RSVP mnemonic: Redness, Sensitivity (photophobia), Vision decrease, Pain — any one of these symptoms in the grafted eye is a rejection alarm and requires same-day review. A patient who presents within 24–48 hours of endothelial rejection onset has a very high chance of saving the graft with intensive steroids. A patient who waits 2 weeks thinking 'it will settle on its own' usually presents with an irreversibly failed opaque graft. RSVP is the patient safety tool that saves corneal grafts.
Clinical Decision-Making: Selecting the Keratoplasty Type
Selecting the appropriate keratoplasty procedure requires integrating four clinical parameters: pathology depth, endothelial status, indication category, and host corneal vascularity. This integration is what separates competent clinical reasoning from simple pattern-matching — each parameter modifies the others, and the final decision must account for the whole patient rather than any single finding in isolation. A patient with mid-stromal scarring and apparently healthy endothelium on specular microscopy (suggesting DALK) may actually need PK if the AS-OCT shows the scar abutting Descemet's membrane, because an attempted DALK dissection at this depth risks intraoperative Descemet's perforation and conversion to PK under emergency conditions — better to plan PK from the start. Conversely, a patient with a heavily vascularised host cornea from old trachoma who nominally qualifies for PK carries such high rejection risk that the surgeon must counsel the patient about the realistic probability of graft failure and consider whether preoperative systemic immunosuppression or counselling about prognosis changes the management plan. The decision framework therefore functions as a starting scaffold for clinical reasoning, not a rigid algorithm, and must always be applied with the patient's specific clinical context, expectations, and access to follow-up care in view.
Is the endothelium healthy?
- Healthy endothelium (specular microscopy count adequate, Descemet's intact on AS-OCT) → preserve it → DALK (anterior disease) or lamellar SALK (superficial only)
- Failed endothelium, stromal opacity minimal → DSEK or DMEK
- Failed endothelium WITH stromal opacity, or full-thickness disease → PK
What is the depth of pathology?
- Superficial (Bowman's/anterior stroma only) → SALK or PTK
- Mid-stromal, Descemet's spared → DALK
- Full-thickness, Descemet's/endothelium involved → PK
- Posterior (endothelium only failing) → DSEK/DMEK
What is the indication category?
- Optical keratoplasty (most cases): choose by depth + endothelial status
- Tectonic keratoplasty (descemetocele/perforation): PK is almost always required — the full-thickness structural repair is the priority, not tissue preservation
- Therapeutic keratoplasty (uncontrolled fungal): PK removes all infected tissue
- Cosmetic: PK or DALK depending on depth; vision gain is not the primary goal
Is the host cornea vascularised?
- Avascular cornea (keratoconus, Fuchs') → lower rejection risk → DALK/DMEK optimal
- Heavily vascularised cornea (old fungal scar, trachoma) → high rejection risk for PK → consider systemic immunosuppression preoperatively; worse prognosis
A summary decision guide: keratoconus → DALK (or PK if failed DALK); Fuchs' endothelial dystrophy / pseudophakic bullous keratopathy → DSEK or DMEK; full-thickness post-infective leukoma / adherent leukoma → PK; descemetocele/perforation → PK (tectonic).
Self-Assessment: Keratoplasty
Apply your knowledge to these clinical scenarios.
Scenario 1: A 58-year-old woman with Fuchs' endothelial dystrophy has diffuse bilateral corneal oedema. Her corrected VA is 6/60 in both eyes. Specular microscopy shows 350 cells/mm² bilaterally. Anterior segment OCT shows clear stroma with no opacity above Descemet's membrane. Which keratoplasty is indicated, and what is its advantage over PK? Answer: DSEK or DMEK — endothelial keratoplasty. The stroma is healthy and transparent; only the endothelium is failing. DSEK/DMEK replaces only the failing layer (Descemet's + endothelium) through a small incision. Advantages over PK: faster visual recovery, no large wound (lower risk of traumatic rupture), lower endothelial rejection rate, preservation of host stromal architecture.
Scenario 2: A patient who underwent PK for a fungal keratitis scar 2 years ago calls your clinic at 7 PM with sudden redness, photophobia, and haloes around lights in the grafted eye. What is your diagnosis and management? Answer: Suspect endothelial rejection (the timing, symptoms, and context all fit — RSVP symptoms). Tell the patient to come in immediately (same evening if possible). On slit-lamp — look for the Khodadoust line. If confirmed: start prednisolone 1% every hour immediately; consider oral prednisolone 1 mg/kg; review the next day. Do not wait for morning clinic.
Scenario 3: Name the four types of keratoplasty rejection in order from least to most serious, giving the specific slit-lamp sign for each. Answer: (1) Epithelial — Eisner's line (advancing epithelial line); (2) Subepithelial — Krachmer's spots (scattered subepithelial infiltrates); (3) Stromal — diffuse stromal haze and vascularisation; (4) Endothelial — Khodadoust line (line of endothelial KPs advancing from periphery to centre); most serious.