Page 12 of 18
OP6.4 | Systemic Uveitis Associations and Patient Counselling — SDL Guide (Part 2)
Counselling the Patient with Uveitis: A Structured Framework
Effective patient counselling in uveitis requires a structured approach because the information load is high, the disease is chronic, and the consequences of poor understanding (stopping drops too early, ignoring a recurrence, failing to attend follow-up) are severe. A five-domain framework ensures comprehensive coverage without overwhelming the patient in a single encounter.
Provided image
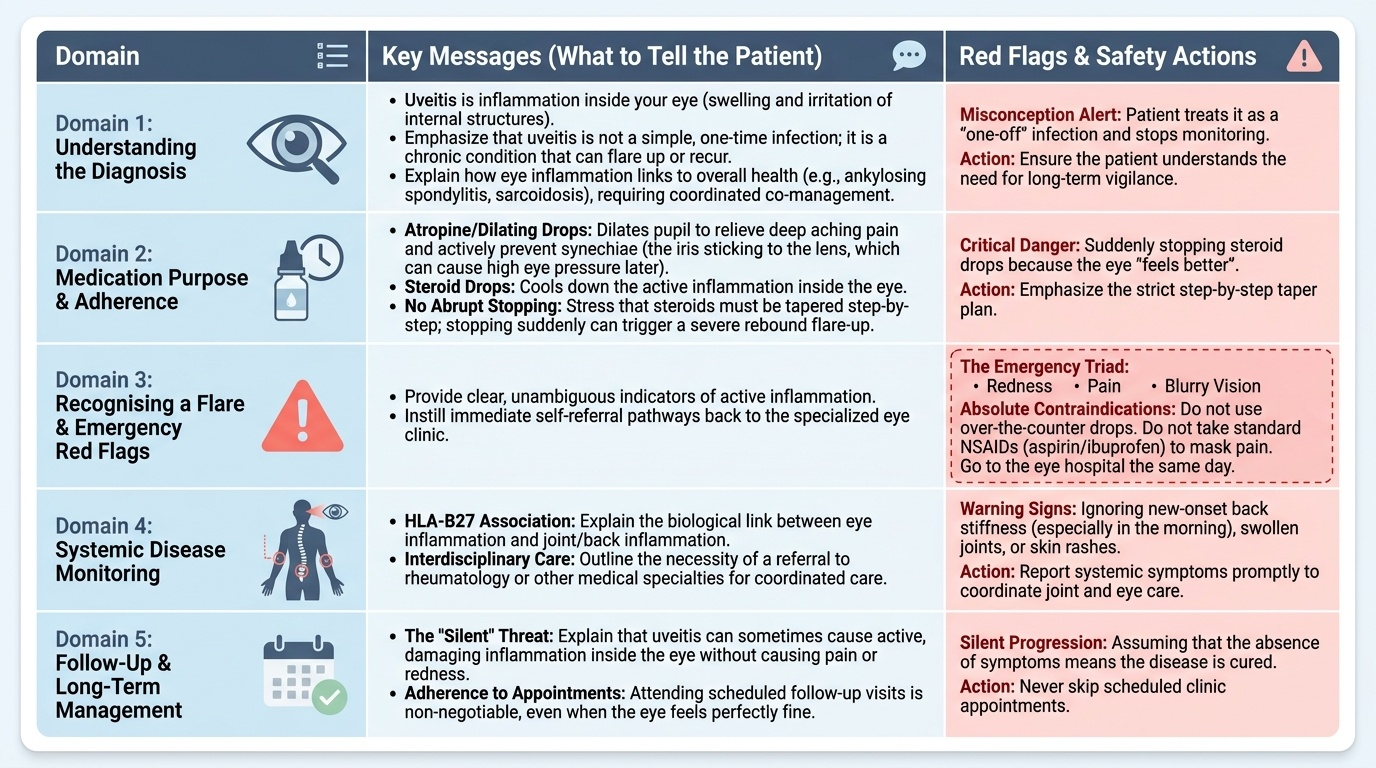
Domain 1 — Understanding the diagnosis:
Explain in plain language: 'Uveitis means that the inside of your eye is inflamed — there is swelling and irritation of the structures that make the eye work. We have treated it with eye drops. The important thing to understand is that this is a condition that can come back — it is not like a simple infection that you treat once and is gone.'
For patients in whom a systemic association is found: 'We have found that your eye inflammation is linked to [ankylosing spondylitis / sarcoidosis / etc.]. This means the eye is telling us something important about your overall health, and we need to manage both together.'
Domain 2 — Medication purpose and adherence:
Explain each medication: 'The atropine drops keep your pupil open — this is not just to help the pain; it actively prevents a complication called synechiae, which is when the iris sticks to the lens and can cause pressure problems later. The steroid drops reduce the inflammation. It is critical that you do not stop these drops suddenly, even when your eye feels better — stopping too early can cause the inflammation to flare back, sometimes worse than before. I will tell you exactly how to reduce them step by step.'
Domain 3 — Recognising a flare and emergency red flags:
This is the most safety-critical domain. Give specific, actionable instructions: 'If your eye becomes red, painful, or your vision blurs — come to the eye hospital the same day. Do not wait. Do not take over-the-counter eye drops. Do not take aspirin or ibuprofen for the pain. Come to us immediately.'
Domain 4 — Systemic disease monitoring:
For HLA-B27-positive patients: 'Your eye inflammation is linked to inflammation in your joints and back. We are referring you to a rheumatologist. Even if your back is not painful right now, it is important to be evaluated.' For sarcoidosis/TB: 'We are arranging tests to find out if there is inflammation [infection] in other parts of your body — particularly the lungs. This is important for your overall health.'
Domain 5 — Long-term vision and lifestyle:
'With proper treatment and follow-up, most people with uveitis keep good vision. However, if the inflammation is not controlled, it can cause permanent damage — pressure in the eye, cataract, or scarring at the back of the eye. This is why regular follow-up is not optional — even when you feel well. Regular check-ups allow us to detect and treat any complications early.'
Applying the Framework: Counselling Scenarios in a Simulated Environment
Reading a counselling framework is not the same as being able to apply it under the time pressure and emotional complexity of a real (or simulated) clinical encounter. The following two worked scenarios provide model language and decision points — read them as an actor would read a script: internalise the logic and the words, then practise with a partner until they become natural.
Scenario 1: Newly diagnosed HLA-B27 anterior uveitis with ankylosing spondylitis
Patient: 32-year-old man, third episode of acute left anterior uveitis. HLA-B27 positive. Complains of morning back stiffness for 3 years.
Opening (elicit understanding first): 'Before I explain what we found, can you tell me what you already know about uveitis — or what you think has been causing your red eye attacks?'
Explaining the link: 'Your blood test has come back positive for something called HLA-B27. This is a genetic marker that means your immune system has a tendency to become overactive in certain ways — and this is causing both the eye attacks and, we suspect, the back stiffness you have been experiencing. The two conditions are connected — it is the same underlying immune issue showing up in two places.'
Explaining recurrence risk honestly: 'I want to be clear with you: this is a condition that is very likely to come back in one or both eyes over the coming years. That is not a reason to be frightened — but it is a reason to be prepared. Every time you notice a painful, red, light-sensitive eye, even mild, come to us the same day. The earlier we treat it, the better the outcome and the lower the risk of permanent damage.'
Medication counselling: 'For this episode, you will use two kinds of drops. The atropine is to keep the pupil open and prevent the iris from sticking to the lens. The steroid drops fight the inflammation. Here is the taper schedule — let me write it down for you. Do not stop the drops before finishing the schedule, even if the eye looks and feels completely normal.'
Referral: 'I am referring you to a rheumatologist — a specialist in joint and back conditions — today. Please do not delay this appointment.'
Scenario 2: Counselling a parent of a child with JIA-associated asymptomatic uveitis
Patient: mother of a 9-year-old girl with oligoarticular JIA (ANA-positive), who is asymptomatic. Slit-lamp shows 2+ bilateral cells.
Explaining the paradox: 'I know it seems strange that I am telling you your daughter has eye inflammation when she has no symptoms at all. She has not complained of a red eye, pain, or blurred vision — and that is actually exactly the problem. This type of uveitis that occurs with her type of arthritis is often completely silent. The inflammation is happening invisibly, and without treatment, it can permanently damage her vision over time — including causing a type of calcium deposit on the cornea called band keratopathy and, eventually, cataract.'
Explaining treatment necessity: 'Because we have found active inflammation on examination — even without symptoms — she needs treatment now. We will start anti-inflammatory eye drops. It is critical that she uses them regularly even though her eyes look and feel completely normal to her. The drops are treating something she cannot feel.'
Explaining screening: 'Even with treatment, we need to see her every three months for a slit-lamp examination. This is because we cannot rely on symptoms to tell us whether the inflammation is controlled. Only the slit-lamp can tell us that. Please do not skip these appointments even if she is completely well — the examination IS the check-up.'
CLINICAL PEARL
Two counselling rules that prevent the most dangerous patient errors in uveitis: (1) 'Never stop the drops suddenly — taper as I showed you.' Patients who feel better often stop their steroid drops abruptly and present 2 weeks later with a severe rebound flare and new posterior synechiae. (2) 'Any red eye is an emergency until we see you.' Patients with recurrent uveitis sometimes try to 'manage it at home' or go to a pharmacy for over-the-counter drops — this delays treatment during the critical window when cycloplegia prevents synechiae formation. Both errors are entirely preventable with clear, specific, written counselling instructions.
Evaluating Your Counselling: Principles and Pitfalls
After any counselling encounter — real or simulated — a competent clinician reflects on whether the communication achieved its purpose. In the OSCE context, you will be evaluated on specific behaviours; in clinical practice, self-evaluation determines whether you improve. The following framework helps identify the most common counselling failures in uveitis encounters and how to correct them.
Common pitfall 1 — Over-reassurance ('You'll be fine'):
Telling a patient with a chronic, recurrent condition that 'everything will be fine' is inaccurate and sets them up for a crisis if they experience a severe recurrence. Honest, calibrated reassurance is better: 'With proper treatment and follow-up, the large majority of patients with uveitis maintain good vision. However, we need to work together — the treatment and the monitoring are both essential.' Calibrated hope, not false certainty.
Pitfall 2 — Jargon and technical terms without explanation:
'You have HLA-B27-associated iridocyclitis with posterior synechiae risk' is incomprehensible to most patients. Translate every technical term: 'You have inflammation inside the eye linked to a genetic marker that also affects your joints. The drops prevent the iris from getting stuck to the lens.'
Pitfall 3 — Not explaining the recurrence risk:
The single most important piece of information for a patient with recurrent anterior uveitis is that the condition will return, and that the response time to that recurrence determines the outcome. Many clinicians focus on the current episode and forget to explain this. Every uveitis counselling encounter must include the recurrence message.
Pitfall 4 — Not explaining the steroid taper:
Patients who do not understand why the drop frequency has to be reduced slowly (rather than stopping when 'better') will stop too early. Explain with an analogy: 'Reducing these drops gradually is like turning down a fire slowly — if you turn off the hose all at once, the fire flares up. We reduce the drops step by step so the inflammation does not bounce back.'
Evaluating yourself after a simulated encounter:
Ask three questions: (1) Did the patient understand what they have? (2) Do they know what to do if it comes back? (3) Do they understand how to use and taper the medication? If you cannot confirm all three with a 'teach-back' from the patient, the counselling is incomplete.
SELF-CHECK
A 28-year-old patient with a first episode of acute anterior uveitis has been treated for 3 weeks with prednisolone acetate 1% four times daily and atropine. His eye now looks and feels completely normal. He asks if he can stop the drops today since he is better. The correct advice is:
A. Yes — if the eye is symptom-free and looks normal, it is safe to stop immediately
B. No — he must taper the steroid drops gradually (reduce frequency step by step) over several more weeks; stopping abruptly risks rebound flare
C. Stop the atropine today but continue the steroid at the same frequency for another month
D. Switch to a weaker steroid drop immediately and stop in one week
Reveal Answer
Answer: B. No — he must taper the steroid drops gradually (reduce frequency step by step) over several more weeks; stopping abruptly risks rebound flare
Steroid drops must be tapered gradually by reducing frequency — from 4× daily to twice daily to once daily to alternate days to stop — not stopped abruptly. Abrupt cessation when the eye appears quiet risks a rebound inflammatory flare as the residual low-level inflammation resurges without suppression. This is one of the most important counselling messages to give uveitis patients. The atropine can be tapered more rapidly as the active inflammation settles, but the steroid taper is essential.
Self-Assessment: Systemic Associations and Counselling Competence
The following questions test both the factual (enumeration of systemic associations) and the applied (counselling decision-making) dimensions of OP6.4. For the factual questions, use the anatomical classification framework (anterior/intermediate/posterior/panuveitis) as your organiser. For the counselling questions, apply the five-domain framework (diagnosis understanding, medication adherence, recurrence/emergency recognition, systemic monitoring, long-term outlook) and identify which domain was being tested. This dual-skill structure reflects the actual NMC competency requirement for OP6.4, which explicitly combines disease knowledge with communication performance in a simulated environment — both elements are equally examinable, and weakness in either will limit your overall competency rating. Approaching the self-assessment with that dual lens active — factual recall and communication reasoning together — is the most productive preparation for the OSCE.
After completing the questions, consider: which systemic association do you feel least confident about? Which domain of the counselling framework is hardest for you to articulate naturally? Targeted practice of the weak areas — either with a revision tool or with a peer in a role-play — is the most efficient path to competence in this dual-skill module.