Page 7 of 20
OP7.3 | Primary Angle Closure Glaucoma — SDL Guide
Learning Objectives
- Describe the pathophysiology of primary angle closure glaucoma (PACG) including the pupil block mechanism and iris bombe
- Recognise the acute angle-closure attack as an ophthalmic emergency with its characteristic presentation
- Identify the anatomical risk factors predisposing to angle closure (hypermetropia, shallow anterior chamber, thick lens)
- Stage the PACG spectrum: PACS, PAC, and PACG, and understand their clinical implications
- Describe the immediate emergency treatment and the definitive surgical/laser management of acute PACG
- Explain why the fellow eye must also be treated prophylactically after an acute attack
INSTRUCTIONS
Primary angle-closure glaucoma is, in many ways, the dramatic opposite of primary open-angle glaucoma. While POAG is silent and insidious, an acute PACG attack is a screaming emergency — severe eye pain, sudden vision loss, nausea and vomiting, a rock-hard red eye with a hazy cornea and a mid-dilated fixed pupil, often with IOP exceeding 50–80 mmHg. Every hour of delay risks permanent vision loss. This module follows the OP arc (presentation → anatomy/pathophysiology → examination → diagnosis → management → self-assessment) to build both the knowledge to recognise PACG and the confidence to initiate appropriate emergency management while awaiting ophthalmology review. The contrast with POAG is woven throughout — getting the management right depends entirely on knowing which type of glaucoma you are treating.
References
- AK Khurana — Comprehensive Ophthalmology, 7th edition, Chapter: Glaucoma (textbook)
- Parsons' Diseases of the Eye, 23rd edition, Chapter: Glaucoma (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old hypermetropic woman presents to the emergency department at 11 PM with a 4-hour history of severe right-sided headache, nausea, and two episodes of vomiting. She mentions that her right eye has been red and painful since the evening, and that she saw coloured haloes around lights before her vision blurred. The emergency physician initially considers migraine and administers an analgesic. But the examining intern notices the right eye is strikingly red with a hazy cornea, a semi-dilated pupil that does not react to light, and that the eye feels rock-hard on gentle palpation. IOP measured with a portable tonometer is 64 mmHg. The left eye IOP is 18 mmHg. What is happening in this woman's right eye, and what must you do in the next 30 minutes to save her vision?
WHY THIS MATTERS
Primary angle-closure glaucoma is not the rarest form of glaucoma, but it is arguably the most dramatic — and the most dangerous when misdiagnosed. In India and across South-East and East Asia, PACG has a higher prevalence than in European populations: South Asian and East Asian individuals have shorter axial lengths, shallower anterior chambers, and thicker lenses that predispose to angle closure. In India, it is estimated that approximately 20 million people have primary angle closure disease, with a significant proportion undetected until an acute attack. The acute angle-closure crisis — as illustrated in the hook — carries a risk of permanent blindness from optic nerve damage if IOP is not brought down within hours. Furthermore, because the fellow eye has the same anatomical predisposition, a bilaterally preventable condition becomes a bilateral emergency without prophylactic treatment. The MBBS graduate stationed in a district hospital or emergency department may be the first — and sometimes the only — clinician available in the critical window before ophthalmology arrives. Recognition and initiation of emergency management can make the difference between preserved and lost vision.
RECALL
To understand angle closure, recall the anatomical relationships of the anterior segment. The anterior chamber is the fluid-filled space between the cornea anteriorly and the iris/lens posteriorly. The iridocorneal angle (drainage angle) is located at the peripheral junction between the cornea and iris root and contains the trabecular meshwork and Schlemm's canal — the primary aqueous outflow route. The pupil is the aperture through which aqueous flows from the posterior chamber (behind the iris, in front of the lens) into the anterior chamber. In a normal eye, this flow is unobstructed. Now recall the concept of ocular dimensions: eyes with shorter axial length (typically hypermetropic eyes) tend to have smaller anterior segments — shallower anterior chambers, more anteriorly situated lens, and more crowded angles. Normal anterior chamber depth is approximately 2.5–3.0 mm; a depth <2.0 mm significantly increases angle-closure risk. Finally, recall that normal IOP is 10–21 mmHg and that the trabecular meshwork must remain functionally open for drainage to proceed normally. Any event that physically occludes the angle will block all conventional outflow and cause a rapid, catastrophic IOP rise.
The Acute Angle-Closure Attack: Presenting Emergency
The acute angle-closure attack — also called an acute angle-closure crisis (AACC) or acute congestive glaucoma — is one of the most dramatic presentations in ophthalmology and one that all clinicians must recognise, because the window for effective intervention is measured in hours, not days. The presentation is the polar opposite of the silent, asymptomatic POAG: it is noisy, painful, and unmistakable in its severity. The pathophysiological basis of this dramatic onset is the sudden, complete obstruction of the entire conventional aqueous outflow route: when the peripheral iris apposes the trabecular meshwork across 360 degrees, all trabecular drainage stops instantaneously, and IOP climbs from a normal value of 10–21 mmHg to 50–80 mmHg or higher within hours. The eye's blood supply to the iris sphincter and to the optic nerve head is compromised at these extreme pressures — which is why rapid IOP reduction is a matter of vision preservation, not merely comfort. The clinical scenario most commonly responsible is a predisposed narrow-angle eye (hypermetropic, shallow anterior chamber) caught in a state of mid-dilation — the position in which the contact area between the posterior iris surface and the anterior lens is maximised, generating the strongest relative pupil block. This is why attacks occur in dim environments (cinema, evening), under emotional stress, or after anticholinergic medication.
The classic presentation of an acute PACG attack:
- Severe unilateral ocular pain: often described as agonising, throbbing; radiates to the forehead and temple on the affected side. The pain intensity frequently leads patients (and clinicians) to think of migraine or intracranial pathology.
- Nausea and vomiting: triggered by the severity of the pain and possibly via a vagal reflex from trigeminal nerve activation; this gastrointestinal component regularly causes the initial misdiagnosis as gastroenteritis, migraine, or 'a stomach problem.'
- Sudden visual blurring: rapid onset, severe; the patient notices they cannot see clearly from the affected eye.
- Coloured haloes around lights: a characteristic symptom arising from corneal oedema (the swollen corneal epithelium acts as a diffraction grating, splitting white light into its spectral components). This is an important distinguishing symptom from other causes of acute red eye.
- Headache: often so prominent that the ocular component is overlooked, especially when examined in a poorly lit environment.
On examination:
- Circumcorneal (ciliary) flush or diffuse conjunctival redness
- Corneal haze/oedema: the cornea appears ground-glass cloudy due to epithelial oedema from raised IOP
- Shallow anterior chamber (particularly notable at the periphery)
- Mid-dilated, fixed pupil: the pupil is approximately 5–6 mm and does not react to light. This occurs because ischaemia from the extreme IOP elevation paralyses the iris sphincter, and because mid-dilation is the position of maximal pupillary block.
- Rock-hard eye on palpation: experienced clinicians may detect the elevated IOP by gentle digital palpation (the eye feels firmer than a normal eye or than the fellow eye)
- Elevated IOP: typically 50–80 mmHg or higher — values unachievable in POAG
Precipitating factors for an acute attack (clinically important):
- Dim light / darkness: physiological pupil dilation in low light increases pupillary block in a predisposed narrow-angle eye. Attacks often occur in the evening or in dark cinemas (the 'cinema sign').
- Stress and emotional upset: causes sympathetically mediated pupil dilation
- Systemic medications that dilate the pupil: anticholinergic drugs (antispasmodics, tricyclic antidepressants, antihistamines, phenothiazines), adrenergic drugs (nasal decongestants, bronchodilators). A careful drug history is essential in all angle-closure presentations.
Anatomy and Pathophysiology: Pupil Block and Angle Closure
The fundamental pathophysiological mechanism in primary angle closure glaucoma is pupil block — a relative obstruction to aqueous flow at the pupillary aperture that builds up pressure in the posterior chamber, causing the iris to bow forward and obstruct the drainage angle. Understanding this mechanism is essential, because it directly dictates treatment: relieving the pupil block is the cure.
In a predisposed eye (short axial length, hypermetropia, narrow angle, thick anteriorly situated lens), the iris sits closer to the lens surface than normal. When the pupil is in a mid-dilated position (around 5–6 mm), the contact area between the posterior iris surface and the anterior lens capsule is at its maximum. This contact acts as a relative valve: aqueous produced by the ciliary body accumulates in the posterior chamber because it cannot flow freely through the pupil aperture. The rising pressure in the posterior chamber pushes the peripheral iris anteriorly — this is called iris bombe (forward bowing of the iris). The bowed peripheral iris then comes into contact with, and occludes, the trabecular meshwork at the iridocorneal angle. With the trabecular meshwork blocked by the iris, aqueous drainage halts completely, and IOP rises precipitously — from normal to 50–80 mmHg within hours.
Anatomical risk factors for PACG:
- Hypermetropia (short axial length): the eye is smaller overall, with less room in the anterior segment
- Shallow anterior chamber depth (<2.0 mm): less space between the iris and cornea
- Thick, anteriorly situated crystalline lens: increases lens-iris contact area
- Short axial length: structural crowding
- Age: the crystalline lens grows throughout life; progressive anterior displacement increases angle-closure risk with age
- Female sex: hypermetropia is more common in women; female eyes tend to have shallower anterior chambers
- East Asian and South Asian ethnicity: population-based anatomical differences in anterior segment dimensions
A critical concept: the pupil block mechanism explains why pilocarpine (a miotic) is an appropriate EMERGENCY treatment for acute PACG. Pilocarpine constricts the pupil by activating the iris sphincter, which reduces the pupillary diameter and pulls the peripheral iris away from the trabecular meshwork, opening the angle. This is mechanistically appropriate because the problem is the iris physically blocking the angle — pulling the iris away opens it. CONTRAST: In POAG, where the angle is already open and the problem is trabecular resistance, pilocarpine adds no benefit and can worsen visual quality through induced myopia and ciliary spasm. This is the most important management distinction in glaucoma.
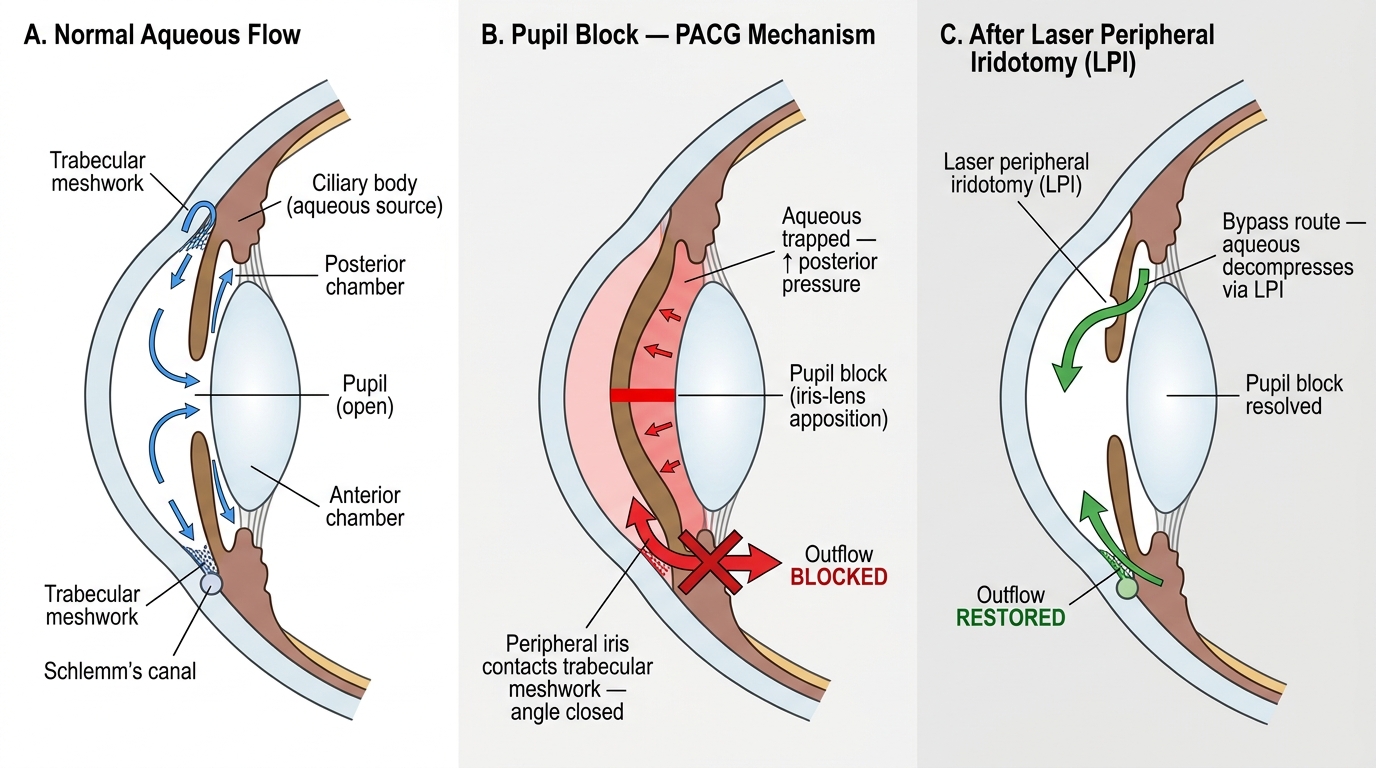
Pupil Block Mechanism in Primary Angle-Closure Glaucoma and Resolution by Laser Peripheral Iridotomy
Examining the Angle-Closure Eye
The examination of a patient presenting with suspected acute PACG must be rapid, systematic, and purposeful — every minute of elevated IOP adds to the risk of permanent optic nerve and iris sphincter damage. The examination should simultaneously confirm the diagnosis, assess severity, and exclude alternative diagnoses. Two important principles govern this examination. First, the findings in acute PACG are largely pathognomonic — the combination of mid-dilated non-reacting pupil, hazy cornea, rock-hard eye, ciliary flush, and extremely high IOP is not seen in any other common ocular emergency. Second, the examination must include the fellow eye, because the fellow eye in an acute PACG attack almost always has the same predisposing narrow-angle anatomy, and if left untreated it will suffer a similar attack. The fellow eye is anatomically vulnerable even though it is symptom-free at this moment. This two-eye perspective — treating the symptomatic eye urgently while planning prophylactic intervention for the fellow — is one of the defining principles of PACG management that distinguishes it from most other ophthalmic emergencies.
Slit-lamp examination reveals the cardinal features of acute angle closure:
- Corneal oedema: the epithelium appears hazy ('ground-glass' or 'steamy'), due to the extremely high IOP preventing normal endothelial pump function. This reduces the view of the iris and lens.
- Shallow anterior chamber: the peripheral anterior chamber appears very narrow or the iris appears to be nearly touching the cornea at the periphery. Van Herick's method (a slit-beam technique) estimates angle depth: grade ≤II suggests a narrow/occludable angle.
- Mid-dilated, non-reacting pupil: the pupil is typically 5–6 mm and oval or vertically elongated. Non-reactivity is due to ischaemic sphincter paralysis from extreme IOP elevation.
- Ciliary flush (circumcorneal injection): deep red flush around the limbus, indicating ciliary body involvement — distinguishes from simple conjunctivitis.
- Iris may be bowed forward (iris bombe): visible as a forward convexity of the iris toward the cornea.
- Lens changes: a sector-shaped white lens opacity (Glaucomflecken — anterior lens capsule and subcapsular epithelial damage from ischaemia) may appear after an acute attack and persist as a permanent marker.
Tonometry:
IOP measurement confirms the diagnosis — values of 50–80+ mmHg are typical. When the cornea is oedematous, the Goldmann reading may be less reliable; the Perkins or Icare tonometer can help.
Gonioscopy (when possible — after IOP reduction):
Gonioscopy is the definitive investigation — it reveals iridotrabecular contact (peripheral anterior synechiae — PAS — if chronic) or appositional closure. The angle is CLOSED, in stark contrast to the OPEN angle of POAG. Gonioscopy during an acute attack is often deferred until IOP is partially reduced.
Fellow eye:
The unaffected fellow eye is examined to assess its angle — it will almost certainly have the same narrow, predisposed anatomy. In an acute unilateral attack, the fellow eye's angle MUST be assessed and prophylactic laser peripheral iridotomy performed as soon as practical.
IMPORTANT: Do NOT perform gonioscopy by pressing hard on the eye during an acute attack — the Schiotz tonometer (indentation) should also be avoided as it can increase IOP transiently.
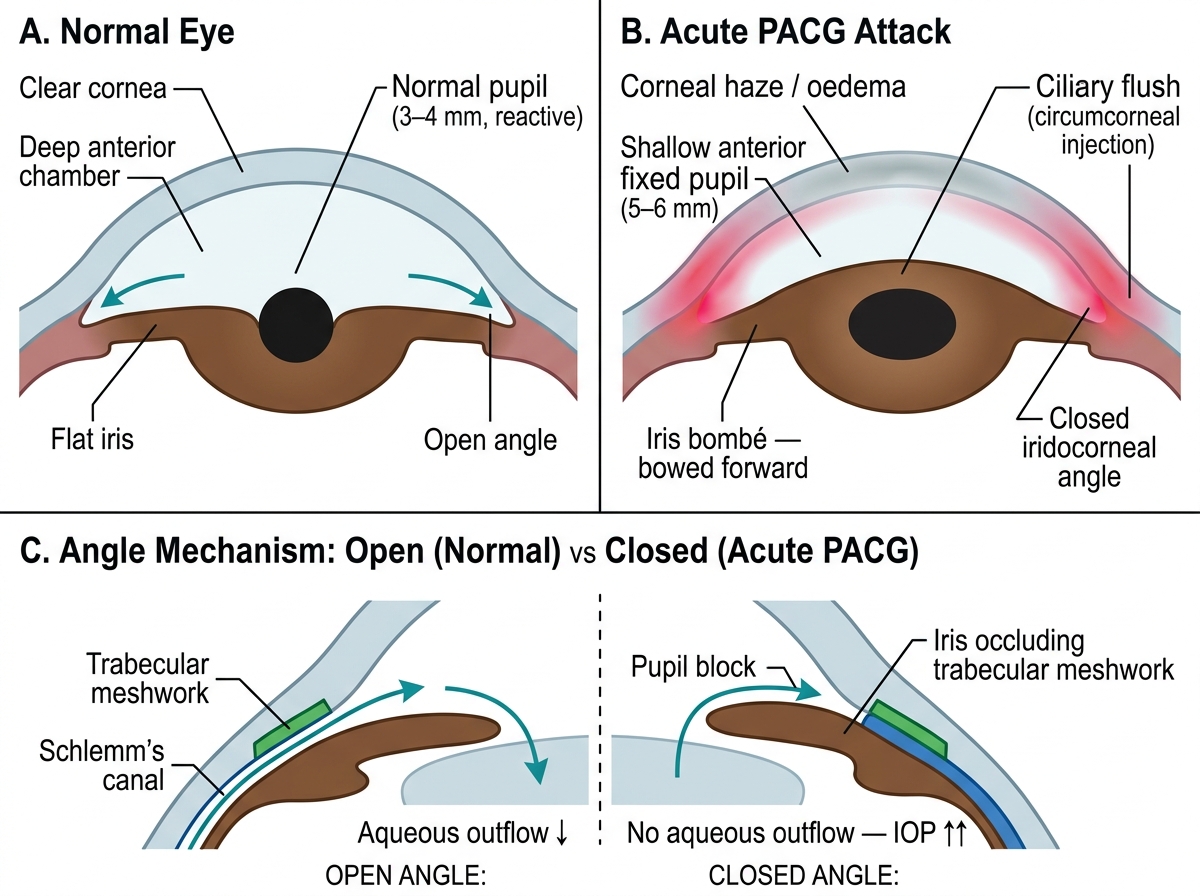
Slit-Lamp Findings: Normal Eye vs Acute Primary Angle-Closure Glaucoma (PACG)
SELF-CHECK
A 60-year-old woman presents with severe right eye pain, nausea, vomiting, and coloured haloes for 5 hours. Examination shows circumcorneal flush, hazy cornea, shallow anterior chamber, mid-dilated non-reacting pupil. IOP is 72 mmHg. Which of the following correctly describes BOTH the diagnosis AND the drug of choice to open the angle?
A. Primary open-angle glaucoma (POAG) — treat with latanoprost
B. Primary angle-closure glaucoma (PACG) acute attack — treat with pilocarpine 2%
C. Primary angle-closure glaucoma (PACG) acute attack — treat with latanoprost
D. Acute anterior uveitis — treat with topical steroids
Reveal Answer
Answer: B. Primary angle-closure glaucoma (PACG) acute attack — treat with pilocarpine 2%
This is an acute PACG attack: severe pain, haloes, shallow AC, mid-dilated non-reacting pupil, IOP 72 mmHg. The mechanism is pupil block → iris bombe → angle closure. Pilocarpine 2% (a miotic) constricts the pupil, pulling the peripheral iris away from the trabecular meshwork to open the angle — mechanistically appropriate. Latanoprost (prostaglandin analogue) is first-line for POAG (open angle) — it does not open a closed angle. This distinction (pilocarpine for angle-closure, prostaglandins for open-angle) is the most critical therapeutic distinction in glaucoma.