Page 10 of 20
OP7.4 | Secondary Glaucoma: Cause Framework — SDL Guide
Learning Objectives
- Classify secondary glaucoma by mechanism: open-angle (pre-trabecular, trabecular, post-trabecular) and closed-angle (with/without pupil block)
- Identify the major named secondary glaucomas and their underlying causes
- Distinguish phacomorphic (closed-angle) from phacolytic (open-angle) glaucoma by mechanism and gonioscopy
- Recognise the clinical clues pointing to specific secondary glaucoma causes (Krukenberg spindle, PXF material, rubeosis iridis, angle recession)
- Describe the two-pronged management approach: IOP reduction plus treatment of the underlying cause
- State why steroid-induced glaucoma is clinically important and how it is managed
INSTRUCTIONS
Secondary glaucoma is a heterogeneous group of conditions unified by a single theme: intraocular pressure is elevated because an identifiable underlying disease or factor is physically obstructing aqueous outflow. The skill in secondary glaucoma is detective work — finding the cause from the history, slit-lamp signs, and gonioscopy. This module uses a mechanistic framework (the HOW: open-angle vs closed-angle, and WHERE within each) as the intellectual scaffold, then maps the major named glaucomas onto it. This approach is more durable than rote memorisation of a list, because once you understand the mechanism, the clinical presentation and treatment follow logically.
References
- AK Khurana — Comprehensive Ophthalmology, 7th edition, Chapter: Glaucoma (textbook)
- Parsons' Diseases of the Eye, 23rd edition, Chapter: Glaucoma (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients attend the glaucoma clinic on the same morning. Patient A is a 35-year-old myopic male who is surprised to find his IOP is 28 mmHg — his optician noticed a faint brownish vertical band on his cornea. Patient B is a 70-year-old diabetic with proliferative retinopathy; his IOP is 46 mmHg and you can see fine blood vessels on the surface of his iris. Patient C is a 65-year-old who was started on prednisolone eye drops 6 weeks ago for an inflammatory condition; his IOP was 14 mmHg before the drops and is now 34 mmHg. All three have elevated IOP, but none has primary open-angle glaucoma. What is causing each patient's pressure to rise — and how does understanding the mechanism change what you do next?
WHY THIS MATTERS
Secondary glaucomas are collectively important for several reasons that make them disproportionately impactful in clinical practice. First, they are frequently more severe than primary glaucomas at presentation — IOP can rise dramatically and rapidly (as in neovascular glaucoma or phacomorphic glaucoma), leaving less time for optic nerve rescue. Second, they are often treatable at the cause level — steroid-induced glaucoma resolves when the steroid is stopped; phacomorphic glaucoma resolves when the lens is removed; neovascular glaucoma can be reversed by anti-VEGF therapy combined with pan-retinal photocoagulation. Third, they are preventable: the glaucoma physician who routinely monitors IOP in patients on topical steroids prevents steroid-induced blindness; the retinal team that aggressively treats proliferative diabetic retinopathy prevents neovascular glaucoma. For the MBBS graduate, the most clinically critical secondary glaucomas to know are steroid-induced (because steroids are prescribed across every specialty), lens-induced (because cataract is universal in India), and neovascular (because diabetic retinopathy is epidemic). A framework understanding — mechanism first, cause second — allows rapid recognition of any secondary glaucoma even on first encounter.
RECALL
Recall the aqueous humour drainage anatomy before building the secondary glaucoma framework. Aqueous flows from the posterior chamber → through the pupil → anterior chamber → iridocorneal angle. At the angle, it must pass through three sequential structures: (1) the trabecular meshwork (TM) — the primary resistance site; (2) Schlemm's canal — the collecting channel; (3) aqueous veins → episcleral venous system — the outflow into systemic circulation. IOP elevation can occur at any of these levels. Also recall the two angle types: OPEN angle (trabecular meshwork, scleral spur, and ciliary band visible on gonioscopy) and CLOSED angle (peripheral iris in contact with TM — iris physically covers the drainage). This distinction — open vs closed angle on gonioscopy — is the most critical initial decision in managing any glaucoma: it separates the treatment pathways. Normal IOP is 10–21 mmHg. Finally, recall that the lens, iris, vitreous, and retina can all generate pathological products or physical changes that disrupt aqueous drainage at one of these levels — this is the logic of secondary glaucoma.
Secondary Glaucoma: Clinical Clues and the Why
The clinical hallmark of any secondary glaucoma is that the elevated IOP has an identifiable underlying cause — it is not a primary failure of the drainage system but a consequence of another ocular or systemic disease, or a drug, or a physical event. This is both the defining feature and the clinical opportunity: identify the cause, and you may be able to treat it at source rather than merely controlling the IOP symptomatically. In primary glaucomas (POAG, PACG), no reversible underlying cause exists and treatment is lifelong IOP reduction. In secondary glaucomas, by contrast, removing the cause may resolve the glaucoma entirely: stopping the offending steroid can normalise IOP within weeks in steroid-induced glaucoma; extracting the swollen lens in phacomorphic glaucoma opens the angle immediately; administering anti-VEGF in neovascular glaucoma causes rubeosis to regress within days. This therapeutic reversibility makes secondary glaucoma both diagnostically important and clinically rewarding — but only if the clinician has the pattern-recognition skills to identify the underlying cause at the first encounter rather than treating elevated IOP blindly.
The clinical approach to secondary glaucoma always starts with history and context:
- Medical history: diabetes (neovascular glaucoma), inflammatory conditions (uveitic glaucoma), steroid use (steroid-induced), trauma (angle recession)
- Drug history: any topical, periocular, or systemic steroid; mydriatics; certain antihypertensives
- Ocular history: previous uveitis, previous retinal vein occlusion, previous vitreous haemorrhage, previous ocular surgery
- Family history: less prominent than in primary glaucomas, but some secondary types have genetic predispositions (pseudoexfoliation has genetic associations with LOXL1 gene)
The secondary glaucoma patient almost always has additional ocular signs that point to the underlying cause — signs that are absent in primary glaucoma. The slit-lamp and gonioscopy are your diagnostic tools: they will reveal the Krukenberg spindle of pigmentary glaucoma, the white PXF material on the anterior lens capsule and pupil margin in pseudoexfoliation, the new blood vessels on the iris (rubeosis iridis) in neovascular glaucoma, the angle recession of traumatic glaucoma, or the hypermature swollen lens of lens-induced glaucoma. This pattern-recognition approach — 'what does the slit-lamp show me that is NOT present in a normal eye?' — is the key clinical skill.
Presentation modes vary:
- Acute: sudden very high IOP, pain, red eye (phacomorphic, neovascular, uveitic)
- Subacute/chronic: gradually rising IOP without acute symptoms (steroid-induced, pseudoexfoliation, pigmentary, angle recession — the same silent presentation as POAG)
- Discovered incidentally: elevated IOP noted on routine check-up (steroid-induced especially)
Pathophysiological Framework: How the IOP Rises
Rather than memorising a list of secondary glaucomas, understanding them through a mechanistic scaffold is more efficient and more durable. The framework has two branches — OPEN-ANGLE and CLOSED-ANGLE — each with sub-levels indicating WHERE in the outflow pathway the obstruction occurs. This scaffold works because the anatomy of aqueous drainage is fixed: fluid must pass through the trabecular meshwork, then Schlemm's canal, then the episcleral venous system. Any secondary glaucoma impairs drainage at one of these anatomical stations, and the gonioscopic appearance (open or closed angle) immediately narrows which branch applies. An open angle on gonioscopy means aqueous can reach the trabecular meshwork but cannot pass through it or beyond it — the obstruction is at or downstream of the meshwork. A closed angle means the peripheral iris has physically occluded the trabecular meshwork before aqueous can even reach it — the obstruction is at the entrance to the drainage system. This single gonioscopic finding — open vs closed — is therefore not merely descriptive; it is the first and most powerful branch point in determining both mechanism and treatment in any case of secondary glaucoma.
BRANCH A: OPEN-ANGLE SECONDARY GLAUCOMAS
The iridocorneal angle is open on gonioscopy, but the aqueous cannot drain normally because of an obstruction at or downstream of the trabecular meshwork.
A1. Pre-trabecular (a membrane or tissue covers the trabecular meshwork):
- Neovascular glaucoma (early): a fibrovascular membrane (driven by VEGF from ischaemic retina) grows over the trabecular meshwork, physically covering the drainage surface. As the membrane contracts, the angle closes (becomes closed-angle NVG — see Branch B).
- Epithelial ingrowth: epithelium grows into the anterior chamber post-surgery, covering the angle.
A2. Trabecular (obstruction within the trabecular meshwork itself):
- Pseudoexfoliation glaucoma: fibrillar extracellular material (PXF material) deposits within the trabecular beams, clogging outflow. This is the COMMONEST secondary open-angle glaucoma worldwide.
- Pigmentary glaucoma: pigment granules (from the iris pigment epithelium, mechanically rubbed off by the iris against the zonules in a concave iris configuration) deposit in the trabecular beams, obstructing them. The Krukenberg spindle (vertical pigment stripe on the corneal endothelium) is the pathognomonic slit-lamp sign.
- Phacolytic glaucoma: liquefied lens protein from a hypermature cataract leaks through the intact lens capsule; macrophages (attempting to clear the protein) and the protein itself clog the trabecular meshwork.
- Ghost cell glaucoma: degenerated, rigid, khaki-coloured red blood cells (ghost cells) from a vitreous haemorrhage enter the anterior chamber and clog the trabecular meshwork.
- Steroid-induced glaucoma: steroids reduce the phagocytic activity of trabecular endothelial cells, allowing extracellular matrix accumulation and increasing outflow resistance.
- Angle-recession glaucoma: traumatic tear in the ciliary body face (between the longitudinal and circular muscle bundles) — the angle appears widened and irregular on gonioscopy; the injured TM develops progressive fibrosis and outflow failure years later.
- Uveitic glaucoma (open-angle component): trabeculitis (direct inflammation of the trabecular meshwork) or steroid therapy given for the uveitis raises IOP.
A3. Post-trabecular (increased episcleral venous pressure backs up outflow):
- Sturge-Weber syndrome: episcleral haemangioma raises episcleral venous pressure → increased outflow resistance → elevated IOP. Associated with facial port-wine naevus (V1/V2 distribution) and choroidal haemangioma.
- Carotid-cavernous sinus fistula: arterialised blood in cavernous sinus raises episcleral venous pressure.
BRANCH B: CLOSED-ANGLE SECONDARY GLAUCOMAS
The peripheral iris is in contact with the trabecular meshwork, obstructing outflow by physical apposition.
B1. With pupil block (aqueous trapped in posterior chamber → iris bombe → angle closure):
- Uveitic glaucoma (closed-angle): posterior synechiae (adhesions between iris and anterior lens capsule) form in anterior uveitis → pupil margin becomes adherent to the lens → seclusio pupillae (360-degree posterior synechiae) → complete pupil block → iris bombe → closed-angle glaucoma.
- Subluxation of lens: if the lens subluxes forward, it may occlude the pupil → pupil block.
B2. Without pupil block (iris pushed or pulled into angle without pupil block):
- Phacomorphic glaucoma: a swollen, intumescent mature cataract physically pushes the iris-lens diaphragm anteriorly, mechanically closing the angle. The angle is closed but there is no pupil block — confirmed by the lens occupying most of the posterior chamber. Treatment: phacoemulsification (lens removal).
- Neovascular glaucoma (late/contracted): the fibrovascular membrane that initially covered the angle (pre-trabecular, open-angle) contracts, dragging the peripheral iris over the trabecular meshwork and closing the angle.
- Malignant glaucoma (aqueous misdirection): aqueous secreted into the vitreous rather than the anterior chamber; lens and iris pushed forward; can occur after intraocular surgery. A notoriously difficult management problem.
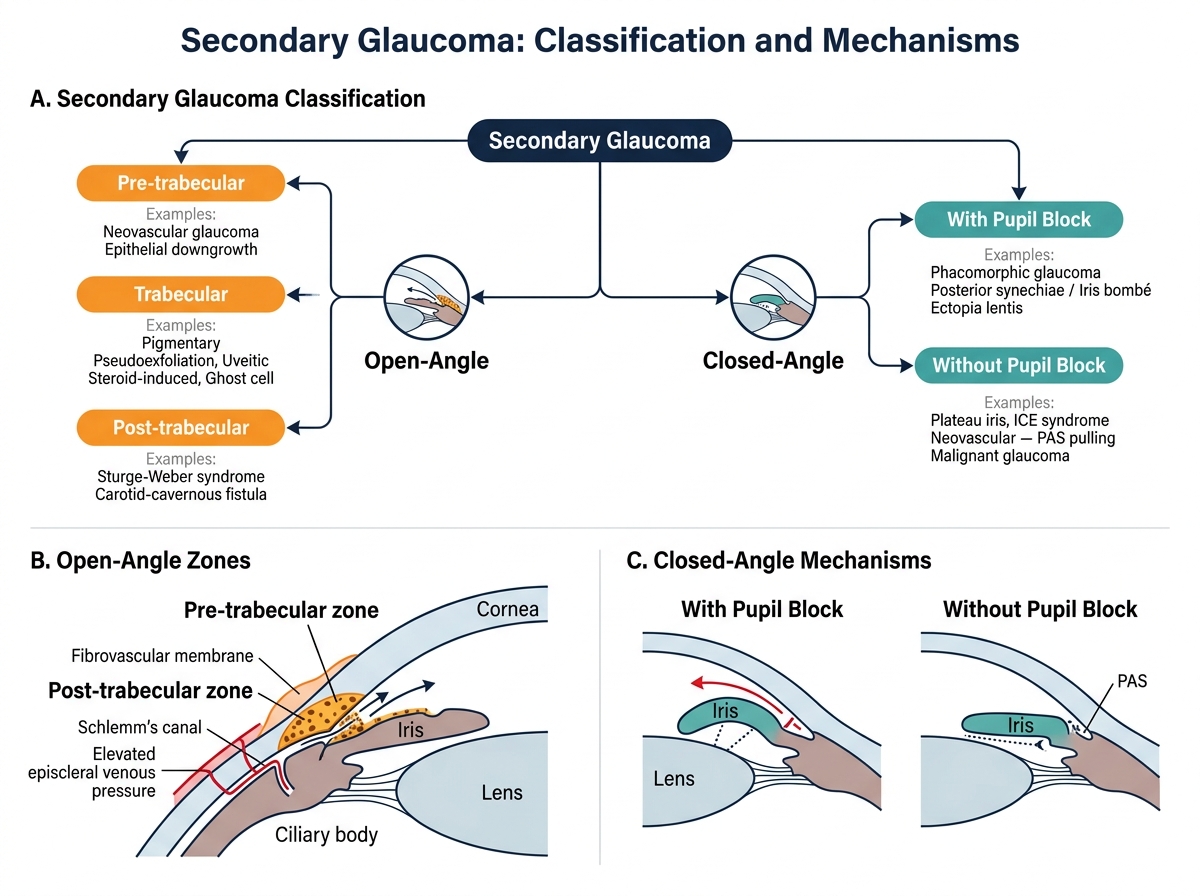
Classification of Secondary Glaucoma by Outflow Obstruction Mechanism
Key Investigations for Secondary Glaucoma
The investigation of secondary glaucoma is guided by the principle that the slit-lamp and gonioscopy will usually reveal the underlying cause if examined systematically. The standard glaucoma work-up (tonometry, optic disc assessment, perimetry, OCT) applies to all cases; the cause-specific investigations are layered on top. The key insight is that secondary glaucoma patients almost always have additional anterior segment signs that are absent in primary glaucoma — signs that point directly to the underlying aetiology. The examining clinician's task is therefore not simply to measure IOP and assess the optic nerve (as in POAG), but to read the entire anterior segment as a diagnostic text: the corneal endothelium, the anterior chamber depth and clarity, the iris surface and pupil margin, the anterior lens capsule, and the angle on gonioscopy each carry specific diagnostic information. Missing these signs — focusing only on IOP and the disc — leads to the dangerous error of treating secondary glaucoma as if it were POAG, missing the reversible underlying cause, and committing the patient to lifelong IOP therapy when the correct intervention is entirely different.
Slit-lamp examination — look for cause-specific signs:
- Corneal endothelium (Koeppe illumination): vertical brown pigment stripe = Krukenberg spindle (pigmentary glaucoma); keratic precipitates (KPs) = uveitis; sclerotic scatter of cornea
- Anterior chamber: cells and flare (uveitis); white fluffy material (phacolytic — macrophages visible); pseudopodial anterior chamber depth (very shallow = phacomorphic)
- Iris: rubeosis iridis (fine blood vessels on iris surface, especially at the pupil margin = neovascular glaucoma); ectropion uvea (late NVG from membrane traction); heterochromia; posterior synechiae; PXF material at pupil margin
- Lens: white fluffy flocculent material on anterior lens capsule = PXF material (pseudoexfoliation); nuclear sclerosis + white flocculent material leaking = phacolytic; swollen, intumescent lens = phacomorphic; anteriorly subluxed lens = pupil block
- Vitreous: khaki/hazel-coloured cells in anterior vitreous or anterior chamber = ghost cells (vitreous haemorrhage history)
Gonioscopy — the MOST IMPORTANT investigation:
- Open angle: POAG or open-angle secondary — then look for specific angle signs:
- Dense trabecular meshwork pigmentation: pigmentary glaucoma (heavy band) or PXF (irregular deposits)
- Angle recession (widening, grey/white ciliary body band): traumatic glaucoma
- New vessels in angle (first at Schwalbe's line/iris root): neovascular glaucoma
- PXF material on trabecular surface
- Closed angle with PAS: chronic angle closure, NVG (contracted), uveitic glaucoma
- Closed angle with lens contact: phacomorphic
Additional targeted investigations:
- B-scan ultrasound: lens position, vitreous haemorrhage, retinal detachment
- Fluorescein angiogram / fundus photography: PDR, CRVO — causes of NVG
- Blood glucose, HbA1c: underlying diabetes
- TORCH screen / ACE / ANA: uveitis work-up
SELF-CHECK
A 68-year-old man with a history of blunt ocular trauma to the right eye 20 years ago presents with a gradually rising IOP (now 28 mmHg) and early arcuate field defect in that eye. Gonioscopy shows an irregular, widened angle with a visible grey-white ciliary body band. The left eye is normal. What is the most likely diagnosis?
A. Primary open-angle glaucoma (bilateral)
B. Pigmentary glaucoma (Krukenberg spindle expected)
C. Angle-recession glaucoma (traumatic — unilateral)
D. Pseudoexfoliation glaucoma
Reveal Answer
Answer: C. Angle-recession glaucoma (traumatic — unilateral)
Angle-recession glaucoma is caused by a traumatic tear in the ciliary body face (between the longitudinal and circular muscle), creating a widened irregular angle with an abnormally visible grey-white ciliary body band on gonioscopy. It is UNILATERAL (following trauma) and develops years to decades after the injury. POAG is typically bilateral. Pigmentary glaucoma shows a Krukenberg spindle on the cornea and dense TM pigmentation. PXF glaucoma shows PXF material on the lens and TM.