Page 14 of 23
OP8.5 | Aphakia — SDL Guide (Part 2)
Optical Aberrations of Aphakic Spectacles
Before IOL implantation became universal, aphakic spectacles (thick +10 dioptre convex lenses) were the only form of optical rehabilitation available to the millions of post-cataract patients globally. Understanding their optical aberrations remains important for three reasons: first, these spectacles are still in use by elderly patients operated decades ago; second, the aberrations explain the functional limitations reported by those patients and why their vision is poor despite technically successful surgery; and third, the optical principles — image magnification, pincushion distortion, ring scotoma — are examined in the NMC CBME theory and OSCE components. A +10D thick convex lens placed at the spectacle plane (approximately 12–14 mm from the cornea) introduces several clinically significant optical distortions that are qualitatively different from the minor aberrations of myopic or hypermetropic spectacle correction. These aberrations are predictable consequences of lens physics, not manufacturing defects, and they are the reason that aphakic spectacles are completely unsuitable for unilateral aphakia.
A +10D thick convex lens placed at the spectacle plane (approximately 12–14 mm from the cornea) introduces several clinically significant optical distortions:
Optical Aberrations of Aphakic Spectacle Correction
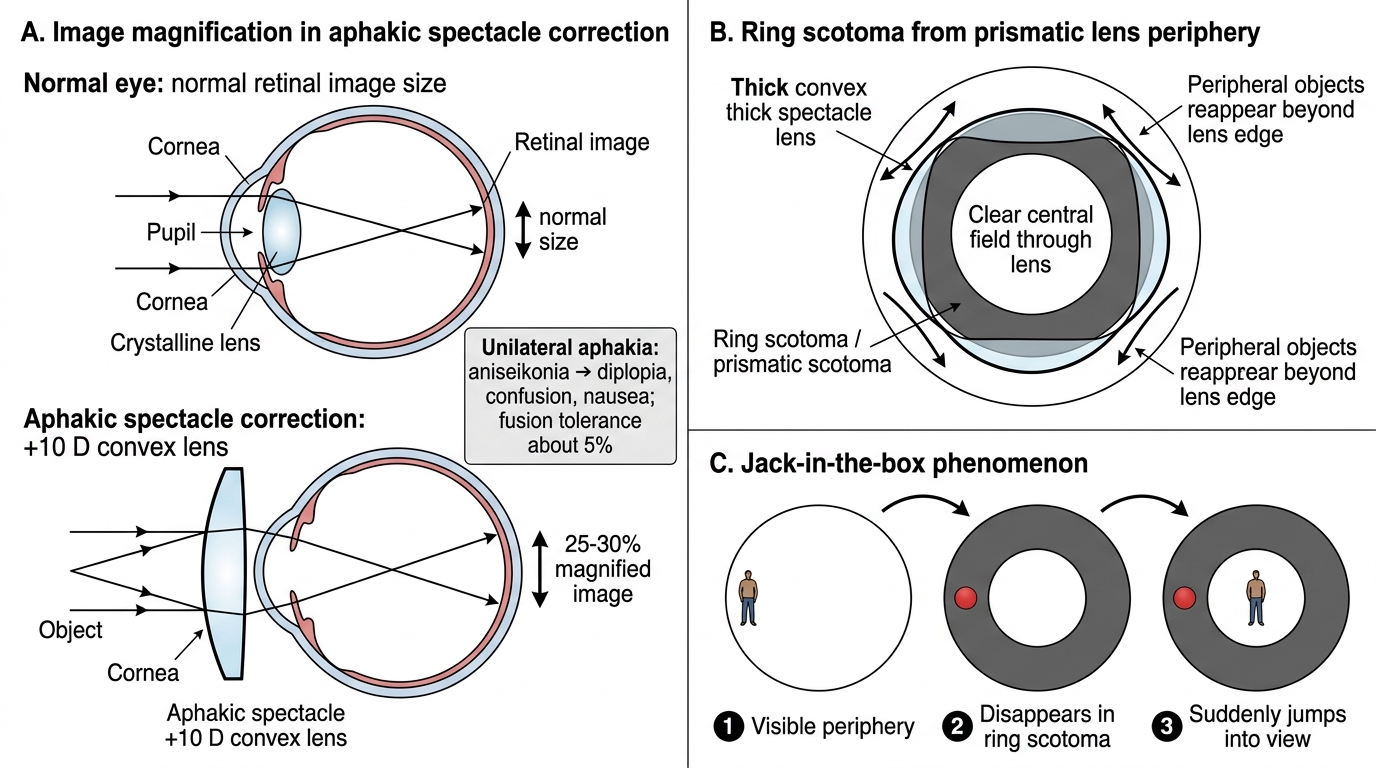
1. Image Magnification (~25–30%): A +10D convex spectacle lens magnifies the retinal image by approximately 25–30% compared to the normal eye. For bilateral aphakia, both eyes see magnified images of equal size — the brain can adapt. For unilateral aphakia, one eye sees a 25–30% larger image than the other — producing aniseikonia (unequal image sizes). The maximum tolerable aniseikonia for binocular fusion is approximately 5%; a 25–30% difference is not tolerated and causes diplopia, confusion, and nausea. This is why aphakic spectacles are absolutely contraindicated in unilateral aphakia.
2. Ring (Prismatic) Scotoma: The thick lens has a prismatic effect at its periphery. Objects at the periphery of the visual field appear displaced or hidden — the patient sees a clear central field, then an absolute scotoma ring, and then peripheral objects again beyond the lens edge. This creates the illusion that objects 'jump' into the central field as the patient turns their head — the
3. Jack-in-the-Box Phenomenon: Objects disappear into the ring scotoma when they are in the scotomatous zone, then suddenly 'jump' into view when the patient moves their head to bring the object into the central clear field — like a jack-in-the-box toy. This is particularly disorienting when walking, especially on stairs.
4. Spherical Aberration: Peripheral rays through a thick lens are refracted differently from central rays, causing peripheral image blur and distortion ('barrel distortion' for convex lenses).
5. Chromatic Aberration: Different wavelengths of light are refracted differently by the thick glass, causing coloured fringes around objects.
6. Weight and Cosmesis: A +10D glass lens is thick and heavy; it requires a strong frame. Modern plastic (polycarbonate) aphakic lenses are lighter, but still cosmetically conspicuous.
Management of Aphakia — Optical Correction Options
The management of aphakia is primarily optical — restoring adequate refractive correction so that the aphakic eye can form a focused retinal image and provide useful vision to the patient. This is both a technical and a patient-centred challenge: the optical correction must not only achieve adequate acuity but must also be tolerable, practical, and compatible with the patient's other eye. In bilateral aphakia, spectacles are a reasonable first option despite their aberrations, because both eyes are corrected equally and aniseikonia is not a clinical problem. In unilateral aphakia, however, the spectacle magnification of 25–30% in the aphakic eye creates an intolerable aniseikonia when the other eye is phakic or correctly pseudophakic — the brain cannot fuse images of such dramatically different sizes, and the patient effectively loses binocular function despite technically functioning eyes. Three modalities of optical correction are available, each with distinct optical characteristics that determine their clinical applicability in specific situations.
Provided image
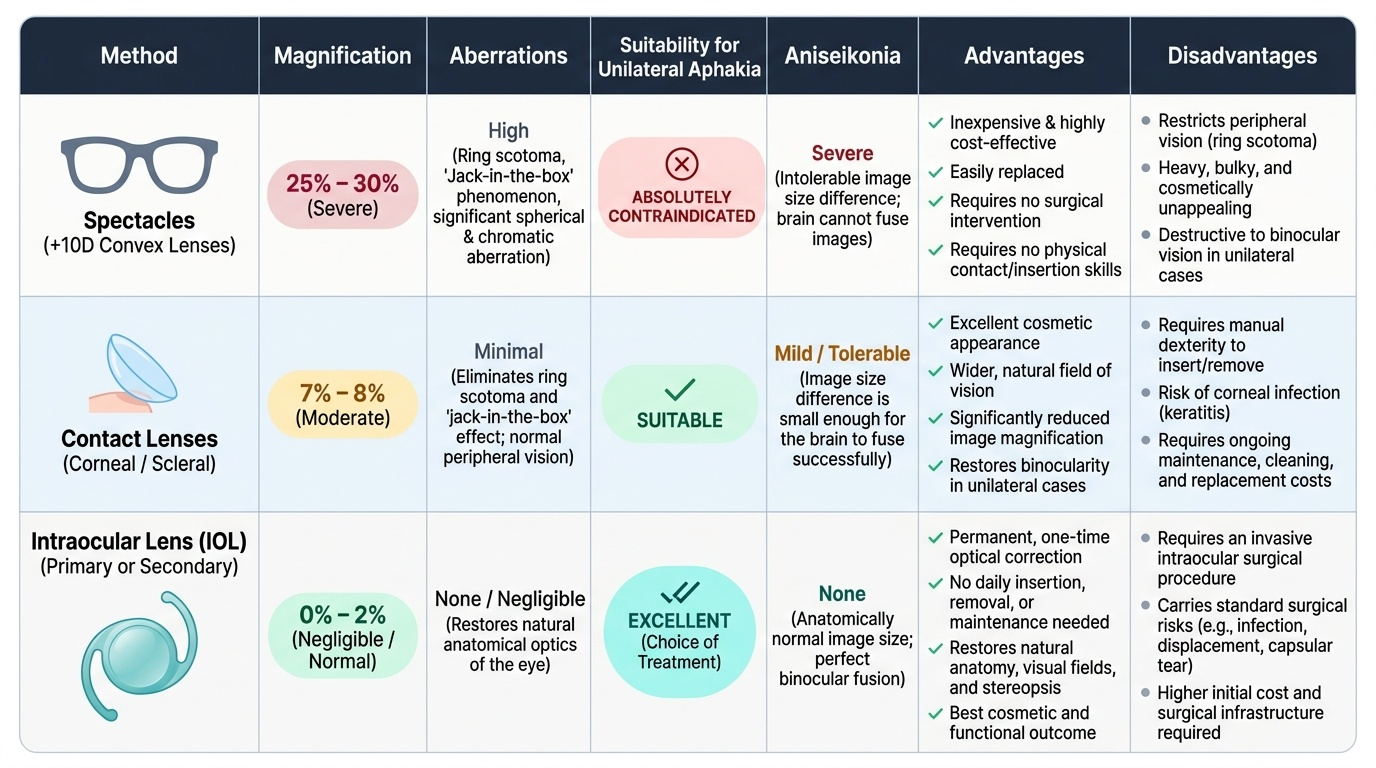
1. Aphakic Spectacles (+10D convex lenses):
Advantages: Inexpensive, easily replaced, requires no surgical or contact lens insertion skill. Available under government schemes.
Disadvantages: Image magnification (~25–30%), ring scotoma, jack-in-the-box phenomenon, spherical and chromatic aberration, heavy and cosmetically prominent. ABSOLUTELY CONTRAINDICATED in unilateral aphakia (intolerable aniseikonia).
Current role: Appropriate ONLY for bilateral aphakia where the patient cannot wear contact lenses and where IOL implantation is not feasible or desired. Rarely prescribed in modern practice but still encountered in patients operated before IOL use was widespread in India.
2. Contact Lenses:
A contact lens sits on the cornea (approximately 2–3 mm from the corneal surface, much closer than the spectacle plane). Because of this proximity to the nodal point of the eye, the image magnification is reduced to approximately 7–8% (from 25–30% with spectacles). This level of magnification is much better tolerated.
Advantages: Much less image magnification than spectacles; no ring scotoma; better cosmesis; suitable for unilateral aphakia (much lower aniseikonia).
Disadvantages: Requires dexterity for insertion and removal; risk of contact-lens-related infection (microbial keratitis — a significant concern in India where contact lens hygiene education may be limited); repeated replacement cost; elderly patients may struggle with handling.
Types used: Daily wear soft lenses, extended-wear lenses, gas-permeable rigid lenses. For infants and young children: contact lens (daily disposable soft, or extended-wear silicone hydrogel) is currently the preferred primary correction in many centres, though secondary IOL implantation is planned later.
3. Intraocular Lens (IOL) Implantation:
Placing an IOL inside the eye at the time of cataract surgery (primary IOL) or as a secondary procedure (secondary IOL) is the current standard of care and provides the best optical outcome. The IOL lies within or very near the nodal point of the eye — image magnification is approximately 1–2%, essentially zero for practical purposes. No ring scotoma, no jack-in-the-box phenomenon. The patient does not need to insert or remove anything.
Types of IOL and their capsular support requirements:
- In-bag IOL (posterior chamber IOL in capsular bag): requires intact capsular bag — possible after ECCE or phacoemulsification; foldable acrylic or PMMA.
- Sulcus IOL (posterior chamber IOL in the sulcus, behind the iris): requires at least posterior capsule rim support; used when the bag is ruptured but posterior capsule rim remains.
- Anterior Chamber IOL (AC-IOL): sits in the anterior chamber angle; used when no posterior capsular support exists (e.g. post-ICCE, or complete capsular bag loss). AC-IOLs have higher rates of corneal endothelial damage over time.
- Secondary IOL: delayed IOL implantation after leaving a patient aphakic — planned in infants <1 year to avoid the complexity of IOL power calculation in a rapidly growing eye.
Pseudophakia = the state of having an IOL in place within the eye.
IOL power calculation: Determined by biometry (axial length + keratometry) using formulae (SRK/T, Barrett); aim is emmetropia (no glasses for distance) or a planned slight myopia for near-task workers.
CLINICAL PEARL
Iridodonesis is the bedside diagnostic sign of aphakia. When you observe the iris trembling on slit-lamp examination during voluntary eye movement, the diagnosis of aphakia (or a subluxated lens with zonular weakness) is made immediately — no other test is needed. Conversely, an eye with an IOL in place (pseudophakia) will show a similar-looking trembling of the iris only if the IOL is dislocated or if zonular weakness is present. When you see iridodonesis in an adult who has had cataract surgery, the key question is: was an IOL implanted? If no IOL is visible on slit-lamp, the patient is aphakic. If an IOL is present, trembling may indicate IOL subluxation or zonular pathology. In either case, referral for further ophthalmic assessment is appropriate.
Special Considerations — Unilateral Aphakia and Paediatric Aphakia
Two clinical situations require special management consideration beyond the standard optical correction framework: unilateral aphakia and paediatric aphakia. Both highlight the limits of spectacle correction and the critical importance of timely IOL or contact lens rehabilitation. Both also carry amblyopia risk — the key difference is that in adults the visual cortex is mature and amblyopia is not a concern, while in children under eight years the risk of permanent cortical amblyopia from uncorrected or poorly corrected aphakia is a time-critical emergency requiring immediate action. Missing the window for amblyopia treatment in a child with aphakia results in irreversible visual loss that no amount of optical correction can subsequently reverse — this is the clinical emergency at the heart of paediatric aphakia management.
Unilateral Aphakia:
When only one eye is aphakic and the other is phakic (or pseudophakic with a correctly powered IOL), spectacle correction of the aphakic eye causes intolerable aniseikonia of approximately 25–30%. The brain cannot fuse these dramatically different image sizes — the patient experiences diplopia, confusion, and severe disorientation. Correction with spectacles alone is therefore contraindicated. Management options are:
1. Contact lens: Reduces magnification to ~7–8% — usually tolerable. Preferred for older adults or children where IOL implantation carries higher risk.
2. IOL implantation: The ideal solution — magnification ~1–2%. If primary IOL was not implanted at original surgery, secondary IOL implantation (with appropriate sulcus placement or AC-IOL if no capsular support) is the definitive treatment.
Paediatric Aphakia:
A child with aphakia after congenital cataract surgery faces two simultaneous crises: (1) Optical defocus on the aphakic retina prevents clear image formation; and (2) Amblyopia — if the aphakic eye is chronically deprived of focused visual input during the critical developmental period (birth to approximately 7–8 years), the visual cortex fails to develop the neural connections for that eye, and the resulting amblyopia is permanent even if optical correction is eventually provided.
This means that optical correction of paediatric aphakia is a time-critical emergency. Every week of delay in correcting the aphakic eye during infancy permanently worsens the amblyopia prognosis.
Current practice for paediatric aphakia:
- Infants under ~1 year: Contact lens is preferred (daily disposable silicone hydrogel aphakic lenses — +20 to +35D power, much higher than the adult because infants have short axial lengths). Secondary IOL implantation is deferred to age 1–2 years because the eye is still growing rapidly and IOL power calculation is inaccurate and unstable in the first year of life. The Infant Aphakia Treatment Study (ISIS trial) found no significant difference in visual outcomes between primary IOL and contact lens at 4.5 years — but BOTH required aggressive amblyopia treatment (patching of the fellow eye for several hours per day).
- Children over ~1–2 years: Primary IOL implantation is generally preferred at the time of cataract surgery. IOL power is slightly 'underpowered' to target slight myopia (accounting for future axial growth — the eye will grow and become more myopic, so a slightly short correction now reaches emmetropia at full growth).
- Amblyopia treatment is mandatory regardless of optical correction method — patching of the fellow eye for prescribed hours per day, monitored by compliance, is as important as the optical device chosen. No lens restores vision if the cortical amblyopia pathway is not actively treated.
SELF-CHECK
A 45-year-old woman had ECCE without IOL implantation in her right eye 10 years ago. Her left eye is normal (6/6). She now wants to wear spectacles for visual rehabilitation. Why are aphakic spectacles NOT appropriate for her right eye?
A. The +10D lens is too heavy for daily wear
B. Aphakic spectacles cause a ring scotoma that cannot be tolerated
C. Unilateral aphakia corrected with +10D spectacle causes approximately 25–30% image magnification in the operated eye, creating intolerable aniseikonia
D. Aphakic spectacles only work for bilateral aphakia but not unilateral
Reveal Answer
Answer: C. Unilateral aphakia corrected with +10D spectacle causes approximately 25–30% image magnification in the operated eye, creating intolerable aniseikonia
In unilateral aphakia, a +10D spectacle correction produces approximately 25–30% image magnification in the operated eye while the fellow eye sees a normal-sized image. The resulting aniseikonia (difference in image size between the two eyes) of 25–30% far exceeds the tolerable threshold of approximately 5%, making binocular fusion impossible — the patient experiences diplopia, confusion, and disorientation. The correct correction is either an IOL (primary or secondary implantation, ~1–2% magnification) or a contact lens (~7–8% magnification). Aphakic spectacles are absolutely contraindicated in unilateral aphakia.
SELF-CHECK
The MOST important principle in managing aphakia after unilateral congenital cataract surgery in a 3-month-old infant is:
A. Immediate IOL implantation
B. Waiting until age 2 years before any optical intervention
C. Immediate optical correction AND aggressive amblyopia treatment
D. Spectacle correction with +10D aphakic glasses
Reveal Answer
Answer: C. Immediate optical correction AND aggressive amblyopia treatment
The most critical principle in paediatric unilateral aphakia management is TIMELY optical correction combined with aggressive amblyopia treatment (patching of the fellow eye). Without both, the visual cortex will fail to develop for the aphakic eye during its critical period, causing permanent amblyopia. In infants under ~1 year, optical correction is typically with contact lens (not IOL) due to rapid axial growth making IOL calculation unreliable; IOL is implanted secondarily. Aphakic spectacles are contraindicated in unilateral aphakia regardless of age. Waiting is the worst option — every week of delay worsens amblyopia.
Self-Assessment — Aphakia: Optical Principles and Clinical Management
Self-assessment at this stage consolidates the optical physics, clinical recognition, and management principles of aphakia — a topic that spans basic science (lens optics, accommodation, aberrations) and clinical medicine (examination findings, optical correction, amblyopia management in children). These questions reflect the integrated style of CBME OSCE and theory assessments. Work through them independently, applying the reasoning frameworks developed in this SDL, before checking against the content. Aphakia is a topic where examiners reward integrated understanding over list memorisation: you must be able to explain why each aberration of aphakic spectacles arises from optical first principles, why spectacles fail for unilateral aphakia, and why paediatric aphakia is a clinical emergency rather than a routine optical challenge. A student who can answer all five questions below with fluent reasoning — including the optical physics, the clinical examination, and the specific management for both adult and paediatric cases — has genuinely mastered this SDL's content and is well prepared for both the written and OSCE components of the ophthalmology assessment.
Structured Review Questions:
- A 70-year-old patient presents with vision of 6/60 in the right eye, uncorrected, that does not improve with pinhole. History reveals cataract surgery 30 years ago with no record of IOL insertion. On slit-lamp examination, the anterior and posterior segments are visible without any lens shadow in the pupillary axis. (a) What is the diagnosis? (b) List three characteristic slit-lamp findings you would expect. (c) What optical correction will you prescribe for this patient, and what magnification-related complaint should you anticipate?
- Explain why aphakic spectacles are contraindicated in unilateral aphakia. Define aniseikonia, state the approximate magnitude caused by aphakic spectacles, and explain why the brain cannot fuse such images. What is the preferred correction for unilateral aphakia in an adult?
- A 4-month-old infant undergoes surgery for congenital cataract. IOL implantation is deferred due to the infant's age. (a) What optical rehabilitation must be initiated immediately and why? (b) What additional treatment is required to prevent amblyopia? (c) At what age would you consider secondary IOL implantation?
- List the optical aberrations of aphakic spectacles in order of clinical significance, explain the physical basis of each, and describe the visual symptom each aberration produces.
- Compare contact lens correction and aphakic spectacle correction for bilateral aphakia on the following parameters: image magnification, aberrations, near vision (accommodation), patient compliance requirements, and risk of infection.