Page 16 of 23
OP8.6 | IMG Team Participation in Cataract Surgery — SDL Guide
Learning Objectives
- Describe the role of an intern medical graduate (IMG) in the pre-operative, intraoperative, and post-operative phases of cataract surgery
- Identify the instruments and equipment used in the cataract operating theatre
- Demonstrate the pre-operative preparation steps performed by the IMG: pupil dilation, systemic checks, prophylactic antisepsis, and consent verification
- Explain the importance of sterile technique and the IMG's intraoperative responsibilities
- Recognise post-operative red flag signs after cataract surgery and initiate appropriate action
- Describe the IMG's role in community eye health outreach and NPCBVI cataract camp settings
INSTRUCTIONS
India performs more cataract surgeries than any other country in the world — over 6 million procedures annually — and the quality of every single one depends not just on the primary surgeon, but on the entire surgical team functioning efficiently. As an IMG entering ophthalmology rotations and clinical posting, you are joining this team. OP8.6 at SH (Skill with Help) level does not mean you will be operating — it means you will be a competent, contributing team member: preparing the patient, maintaining sterility, recognising complications, counselling post-operatively, and serving as a frontline eye health advocate in community settings. This module maps the full scope of that participation.
References
- Khurana AK. Comprehensive Ophthalmology, 7th edition. Chapter 7: Cataract Surgery — Theatre Preparation and Team Roles. (textbook)
- Parson JH. Diseases of the Eye, 22nd edition. Chapter 8: Cataract — Preoperative Care and Postoperative Management. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 7:30 AM and you are reporting to the cataract theatre for your first week of ophthalmology posting. Thirty patients are listed for surgery. The senior resident looks at you and says: 'Good — you're the fourth person I needed. Check the consent forms on the first ten patients, make sure all of them have had their mydriatics, and tell me if any of them has a BP over 180. Then come in to watch the first case.' You stare at the forms, the drop bottles, the sphygmomanometer, and the sterile packs. This is not a passive observation — you have a role, a checklist, and a responsibility. The first patient — a 72-year-old farmer with a bilateral mature cataract — will have a safer, more efficient surgery because you did your part correctly. Welcome to the surgical team.
WHY THIS MATTERS
India's National Programme for Control of Blindness and Visual Impairment (NPCBVI) has set a target cataract surgical rate (CSR) of 8,000 operations per million population per year — a number achievable only with efficient, well-trained surgical teams operating smoothly at scale. In district hospital camps and urban eye care centres alike, the IMG is not a spectator: in the pre-operative area, you check systemic parameters and verify the pre-op workup; in the theatre, you understand the surgical sequence well enough to anticipate and assist; post-operatively, you write the first orders, counsel the patient, and serve as the first line of recognition for surgical complications. OP8.6 — 'Participation of IMG in the team for cataract surgery' — is therefore a clinical SH competency with real patient safety implications, not a box-ticking rotation task.
RECALL
You have already studied the full clinical spectrum of cataract surgery across this module cluster: the anatomy of the lens (OP8.1), the classification and complications of cataract (OP8.2), the pre-operative evaluation and counselling consultation (OP8.3), the surgical techniques including ECCE steps and anaesthesia (OP8.4), and aphakia management (OP8.5). This module synthesises that knowledge into your active clinical role. Recall especially: the pupil must be widely dilated (>6–7 mm) for phacoemulsification; povidone-iodine to the conjunctival sac is the gold-standard pre-operative infection prophylaxis; endophthalmitis on days 2–7 is a same-day emergency; PCO months later is treated by Nd:YAG laser outpatient. These are the facts you will act on.
Why IMG Team Participation Matters in Cataract Surgery
Cataract surgery is India's most impactful elective surgical procedure — a 30-minute operation that restores productive vision to a patient who may have been functionally blind for years. At the systemic level, cataract surgery is the single largest intervention within the NPCBVI, which aims to address the fact that cataract is the leading cause of reversible blindness in India, responsible for approximately 65% of all blindness. The programme trains surgeons, funds operations, and operates camp-format outreach — but the entire pipeline requires a well-functioning team at every step.
The cataract surgical team in a district hospital setting typically includes: the primary surgeon (ophthalmologist), a surgical assistant (often an experienced nurse or resident), a scrub nurse/technician, an anaesthesia provider (for local block cases, often a nurse under supervision), and the IMG assigned to the theatre. Each role has defined responsibilities that, when executed well, reduce operating time, prevent complications, and optimise post-operative outcomes.
For the IMG specifically, the clinical competency at SH level means: you are present, you understand the procedure, you contribute actively to the team, and you perform defined tasks under supervision. You are not expected to perform phacoemulsification, but you ARE expected to: verify that the patient is correctly prepared; ensure the consent form is signed and the pre-operative workup is documented; monitor the patient's systemic parameters; counsel the patient post-operatively; and — critically — recognise and escalate complications without delay.
India's high-volume camp model makes this team role especially important: at a district camp, 40–60 patients may be operated in a single day. The IMG who understands the workflow — which patients need extra mydriatics, whose blood glucose is too high to proceed, who needs an urgent referral after day-1 review — directly influences the safety and efficiency of the programme.
Instruments and Equipment in the Cataract Theatre
Familiarity with the instruments and equipment in the cataract theatre is essential for the IMG to function confidently. You cannot participate safely in a sterile environment if you cannot identify what you are handling, what it is for, and how to pass it correctly.
Operating microscope: A binocular ophthalmic microscope mounted on a ceiling or floor stand, with coaxial illumination that produces the red reflex used during surgery. The IMG typically does not adjust the microscope during a case — but should know how to focus and tilt under supervision before the list begins.
Phacoemulsification machine: The console that delivers calibrated ultrasonic energy, irrigation (balanced salt solution, BSS), and aspiration through the phaco probe. The IMG may be asked to confirm irrigation fluid levels and settings at the start of the list.
Slit-lamp biomicroscope: Used pre- and post-operatively, not during surgery. The IMG should be comfortable with its setup for pre-op checks.
Surgical instruments — key items the IMG must recognise:
- Lid speculum — stainless steel or wire spring device that holds the eyelids apart
- Cystotome / capsulorhexis forceps — for creating the anterior capsulotomy
- Phaco probe (25–27 gauge) — delivers ultrasonic energy; handle with care; the tip is sharp
- Irrigation-Aspiration (I/A) handpiece — dual-channel; irrigation enters through one port, aspirated fluid exits through the other
- IOL introducer / forceps — for loading and delivering the foldable IOL
- Vectis / lens spoon — for nucleus expression in ECCE/MSICS
- Needle holder and suture scissors — for wound closure
- BSS (Balanced Salt Solution) bottles — irrigation fluid; should be at room temperature or body temperature; check expiry date
- Viscoelastic (OVD — Ophthalmic Viscosurgical Device): Methylcellulose or sodium hyaluronate (Healon); used to protect endothelium and maintain AC depth; always ensure viscoelastic is available and at the scrub table
Instrument handling rules for the IMG: Never reach across the sterile field. Pass instruments handle-first. Announce the instrument name when passing. Keep the instrument trolley organised so the surgeon does not need to search. If unsure, ask — a delayed but safe instrument pass is better than a contaminated field.
Pre-operative Preparation — The IMG's Role
The pre-operative preparation of the patient for cataract surgery is one of the most concrete and directly teachable components of the IMG's role. Each step has a specific rationale, and errors — such as inadequate dilation or a missed systemic contraindication — can require case postponement or cause preventable complications. This is not a passive support role: the intern who prepares the patient correctly enables the surgeon to operate safely and efficiently, while the intern who makes an error — failing to instil mydriatics, omitting the povidone-iodine prep, or missing an elevated blood pressure — creates real clinical risk. Knowing not just what to do but why each step matters is the difference between mechanical task completion and competent clinical participation. The preparation protocol is standardised across most Indian ophthalmic units, but you must also understand how to adapt it when a patient presents with a complication — uncontrolled hypertension on the day of surgery, allergy to povidone-iodine, or refusal to sign consent — and know the correct escalation pathway.
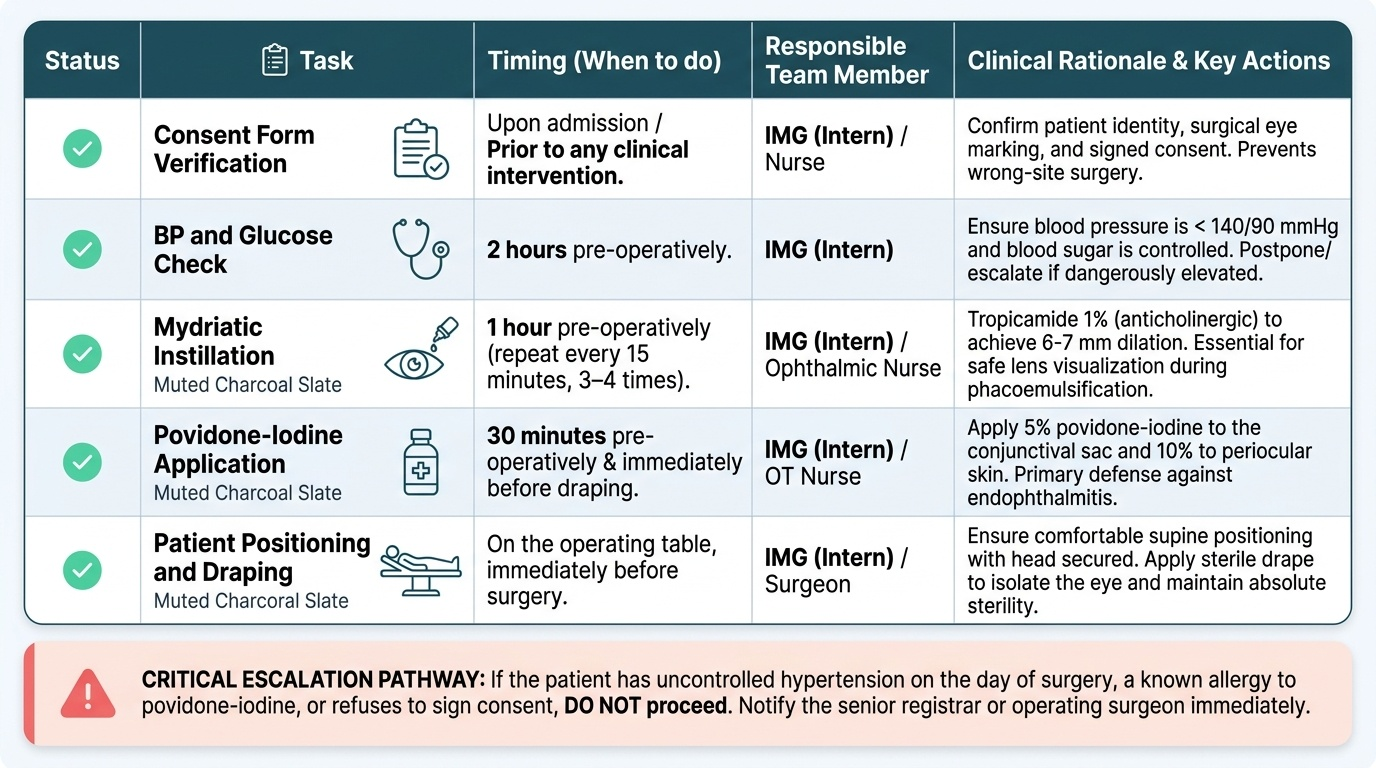
Provided image
Step 1 — Pupil Dilation (Mydriasis):
Adequate mydriasis is essential for phacoemulsification and ECCE — the surgeon needs a dilated pupil (>6–7 mm) to visualise the lens capsule and nucleus. Standard mydriatic protocol:
- Tropicamide 1% (anticholinergic — dilates by paralysing the sphincter pupillae): instil 1 drop every 20–30 minutes × 3 doses; onset 20–30 minutes; maximum effect ~45 minutes.
- Phenylephrine 5% or 10% (sympathomimetic — dilates by stimulating the dilator pupillae): instil with tropicamide for additive effect; useful in dark-pigmented irides that dilate poorly. Note: systemic absorption of phenylephrine 10% can rarely cause hypertension — avoid in uncontrolled hypertension.
- First set of drops should be instilled 60 minutes before the scheduled surgical time.
- The IMG should check the pupil size (torch or slit-lamp) approximately 45 minutes after the first drops — a pupil still <5 mm warrants a further dose and communication to the surgeon.
Step 2 — Systemic Parameter Check:
Immediately before the patient enters the theatre:
- Blood pressure: Systolic >180 mmHg or diastolic >110 mmHg → inform the surgeon; elective surgery should be deferred unless clinically urgent (e.g. phacolytic glaucoma).
- Blood glucose (in diabetics): Fasting blood glucose >250 mg/dL → inform the surgeon; optimise before proceeding.
- Any new systemic complaint (chest pain, breathlessness, fever) → immediately inform the anaesthesia provider and surgeon; do not proceed.
Step 3 — Pre-operative Antisepsis:
- Povidone-iodine (PVI) 5% instilled into the conjunctival sac for 2–3 minutes immediately before surgery is the single most evidence-based intervention to reduce post-operative endophthalmitis. This is a non-negotiable step that the IMG should confirm has been performed.
- The periocular skin (eyelids and surrounding area) is also cleaned with diluted povidone-iodine (10%) as part of surgical preparation.
Step 4 — Consent Form and Pre-op Documentation Verification:
Before the patient enters the operating theatre, verify:
- Signed consent form present with the correct eye documented
- Pre-operative biometry result available and IOL power confirmed
- Systemic investigations (blood glucose, BP record) documented in the notes
- Allergy status recorded (povidone-iodine allergy — rare but important)
Step 5 — Patient Positioning and Draping:
The patient is positioned supine with the head resting in a head ring. A sterile drape (adhesive surgical drape with a central fenestration) is applied over the face to maintain a sterile field. The IMG may assist with draping under supervision; care is needed to ensure the drape does not occlude the airway or cause claustrophobic anxiety in the awake patient.
SELF-CHECK
You are preparing a 68-year-old man for cataract surgery. He received his first mydriatic drops 45 minutes ago. On checking his pupil, it measures 4 mm. Blood pressure is 162/95 mmHg. Blood glucose is 145 mg/dL. Which parameter(s) need action before he enters the operating theatre?
A. Blood pressure only — it is above 160 systolic
B. Pupil size only — 4 mm is inadequate for phacoemulsification
C. Both pupil size and blood pressure need to be reviewed with the surgeon; glucose is acceptable
D. All three parameters require deferral of surgery
Reveal Answer
Answer: C. Both pupil size and blood pressure need to be reviewed with the surgeon; glucose is acceptable
Both pupil size and blood pressure require communication with the surgeon. A 4 mm pupil is inadequate for phacoemulsification (need >6–7 mm) — a further mydriatic dose may be indicated. BP of 162/95 mmHg is elevated but below the typical deferral threshold of >180/110 mmHg; it should be noted and discussed with the surgeon who may proceed or defer based on clinical judgement. Blood glucose of 145 mg/dL in a diabetic patient is acceptable for surgery (threshold for deferral is typically >250 mg/dL fasting). All three values should be communicated, but glucose alone would not delay surgery.