Page 16 of 26
OR1.6 | Recent Advances in Orthopaedic Management — SDL Guide (Part 2)
Advances in Arthroplasty
Joint replacement surgery has undergone continuous evolution in four key areas: bearing surfaces (to reduce wear and extend implant life), fixation methods (cemented versus cementless), surgical approach (minimally invasive techniques), and technological assistance (computer navigation and robotic systems). The goal of each advance is the same: a hip or knee replacement that functions normally, lasts for the patient's remaining lifetime, and can be revised if necessary without catastrophic bone loss. Understanding which advances are evidence-based and which remain investigational allows the clinician to make appropriate implant recommendations and to explain the rationale for each choice to the patient.
Bearing surface evolution in total hip arthroplasty (THA):
The original metal-on-polyethylene (MoP) bearing was limited by wear of the polyethylene liner, generating particulate debris that caused aseptic loosening (osteolysis around the implant — the single most common cause of THA failure). Advances have progressively reduced wear:
- Highly cross-linked polyethylene (XLPE): irradiation cross-linking of polyethylene dramatically reduces wear by up to 95%; now the standard polyethylene used in most THA.
- Ceramic-on-ceramic (CoC): alumina or zirconia toughened alumina bearings; lowest wear, excellent hardness and scratch resistance; risk of 'squeaking' and catastrophic fracture (rare); preferred in young high-demand patients where 25–30 year implant survival is needed.
- Metal-on-metal (MoM): largely abandoned after the MHRA and FDA recalled certain designs due to high cobalt-chromium ion levels (causing pseudotumour formation and 'metallosis') — a cautionary example of rapid adoption without long-term follow-up.
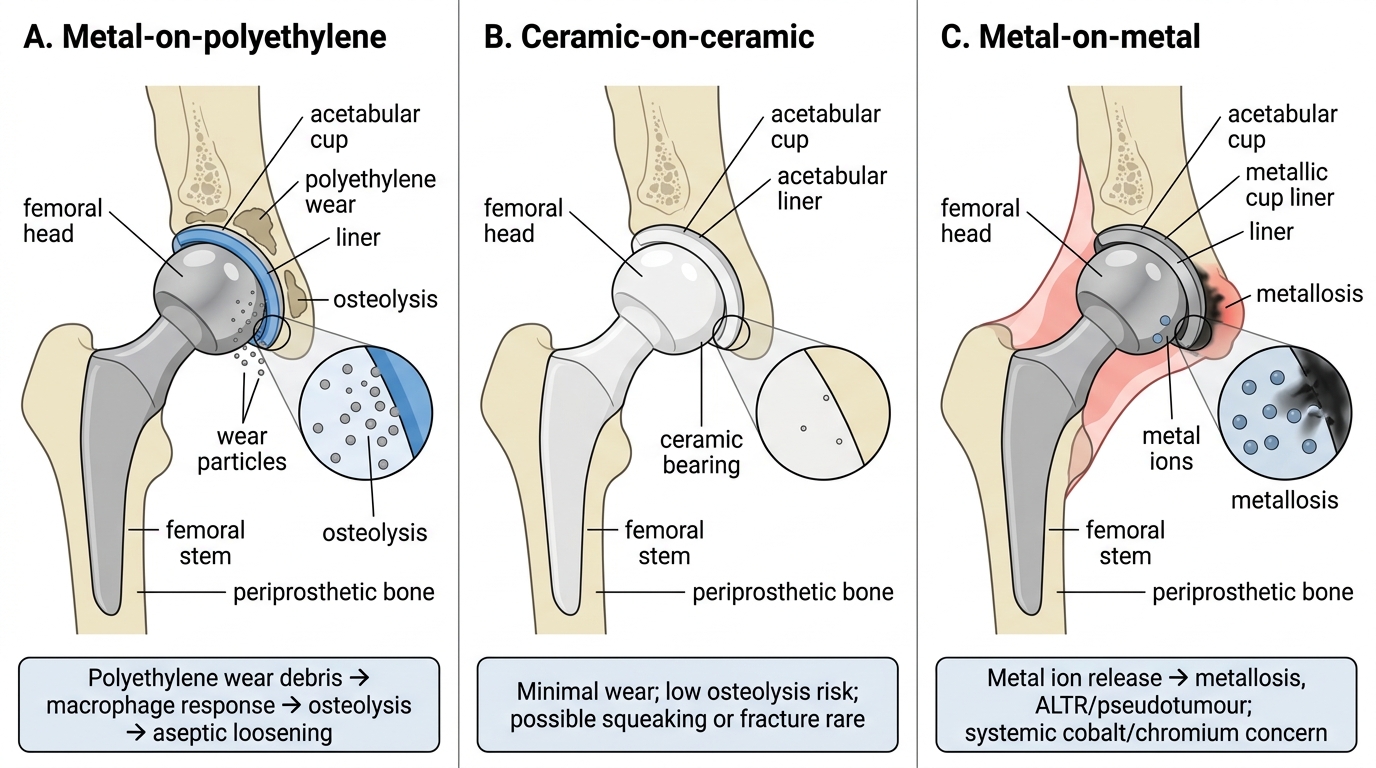
Bearing Surfaces in Total Hip Arthroplasty
Cementless versus cemented fixation:
Cemented fixation (polymethylmethacrylate, PMMA bone cement) achieves immediate stability and reliable results in elderly patients with poor bone quality. Cementless fixation relies on osseointegration — the implant surface (sintered beads, hydroxyapatite coating, trabecular metal) allows bone ingrowth and ongrowth, achieving biological fixation over 6–12 weeks. Cementless fixation is preferred in younger patients (bone ingrowth provides durable long-term fixation without cement degradation); cemented fixation remains the standard in elderly osteoporotic patients.
Robotic-assisted arthroplasty (e.g., MAKO system): uses CT-based 3D planning and an intraoperative robotic arm to guide bone resection with sub-millimetre precision. Clinical studies show improved component positioning accuracy and reduced outliers; whether this translates to improved long-term patient outcomes is under investigation. Available at select tertiary centres in India.
Unicompartmental knee arthroplasty (UKA): for patients with isolated medial compartment osteoarthritis and intact ACL; replaces only the medial compartment, preserving bone stock and proprioception; faster recovery than total knee replacement; conversion to TKR is straightforward if the disease progresses. Requires careful patient selection.
Advances in Spine Surgery
Spinal surgery has been revolutionised by three parallel developments: minimally invasive spine surgery (MISS), motion-preserving procedures (cervical disc replacement, dynamic stabilisation), and improved understanding of sagittal balance. Together these have shifted the goal of spinal surgery from 'decompress the neural elements' to 'restore the mechanical architecture of the spine while decompressing neural elements with minimal collateral tissue damage.'
Minimally invasive spine surgery (MISS): traditional open spinal surgery requires extensive paraspinal muscle stripping, causing denervation, atrophy, and chronic back pain — the 'fusion disease' or 'failed back surgery syndrome' that has long complicated spinal outcomes. MISS techniques use tubular retractors, expanded working channels, or endoscopic systems to reach the spine with minimal muscle disruption. Clinical benefits demonstrated in RCTs include reduced blood loss, shorter hospital stay, reduced post-operative pain, and faster return to activity. MISS is now standard for single-level lumbar discectomy, lumbar decompression, and selected lumbar interbody fusion procedures.
Cervical total disc replacement (TDR): in conventional cervical discectomy and fusion (ACDF), the degenerate disc is removed and the level is fused with a cage and plate. Fusion eliminates motion at that level, transferring stress to adjacent levels — 'adjacent segment disease' develops in approximately 2.5% of cases per year. Cervical TDR implants a prosthetic disc that preserves segmental motion, potentially reducing adjacent segment stress. Multiple RCTs have shown TDR to be non-inferior to ACDF for radiculopathy and superior for some functional outcomes at 5–7 years; FDA approved for single and two-level disease. Not suitable for patients with facet joint arthritis, osteoporosis, or segmental instability.
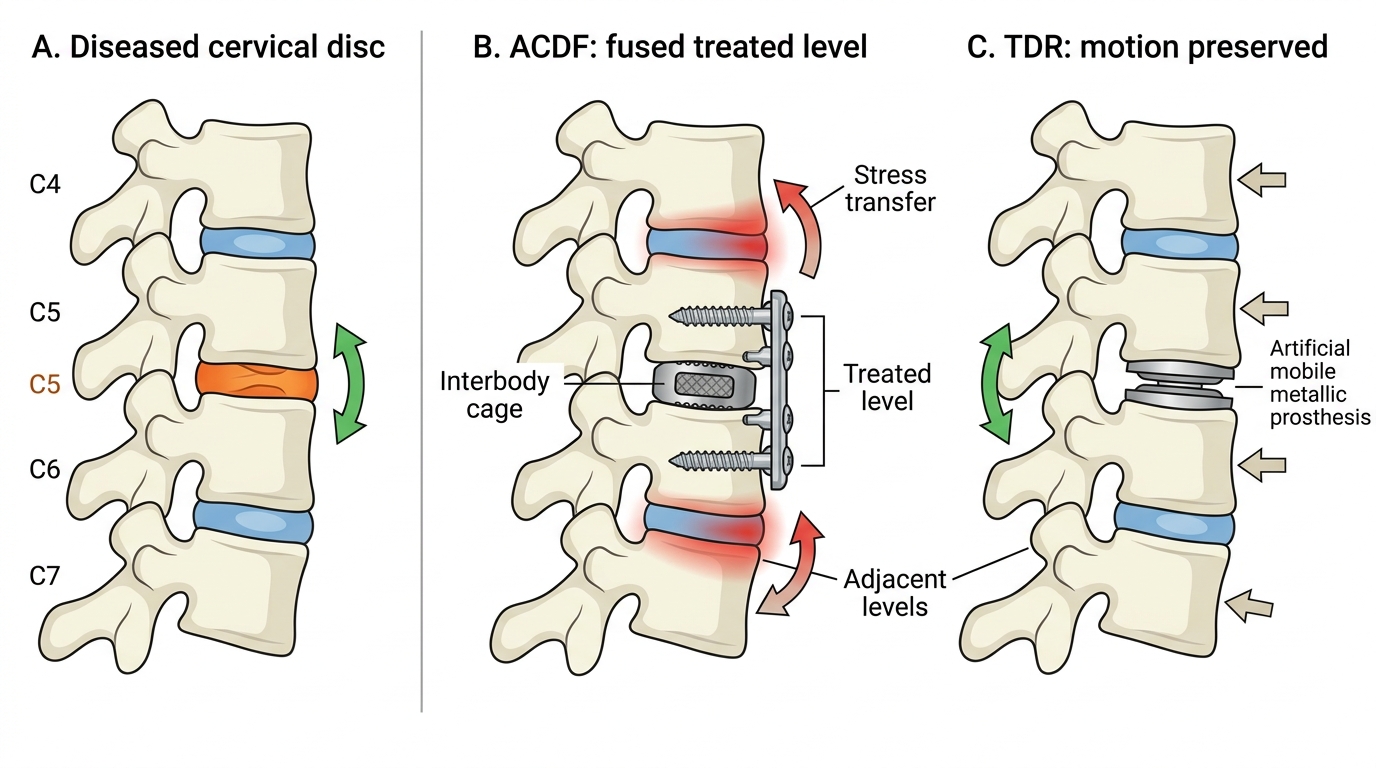
ACDF Versus Cervical Disc Replacement
Lumbar total disc replacement is more technically challenging than cervical TDR (larger working space required, anterior approach to the lumbar spine, proximity to great vessels) and remains under investigation for broader indications. Currently approved for single-level L4-5 or L5-S1 disc degeneration in young patients without facet degeneration.
Computer-assisted pedicle screw placement: pedicle screws are the workhorses of posterior spinal fixation; misplacement breaches the pedicle cortex and risks neural or vascular injury. Navigation using preoperative CT or intraoperative O-arm imaging reduces screw misplacement rates from approximately 10–15% (free-hand) to 2–4% (navigated). Robotic systems (Mazor, Globus) further automate screw trajectory planning and execution.
Vertebroplasty and kyphoplasty for osteoporotic vertebral compression fractures: vertebroplasty injects polymethylmethacrylate (PMMA) cement directly into the fractured vertebral body to provide mechanical stabilisation and pain relief. Kyphoplasty uses an inflatable balloon to first restore vertebral body height, then fills with cement. Vertebroplasty provides pain relief in acute fractures (<6 weeks); kyphoplasty additionally restores height and reduces kyphosis. Both are performed percutaneously under fluoroscopic guidance.
Clinical and Applied Significance: Indian Context and Critical Appraisal
Provided image
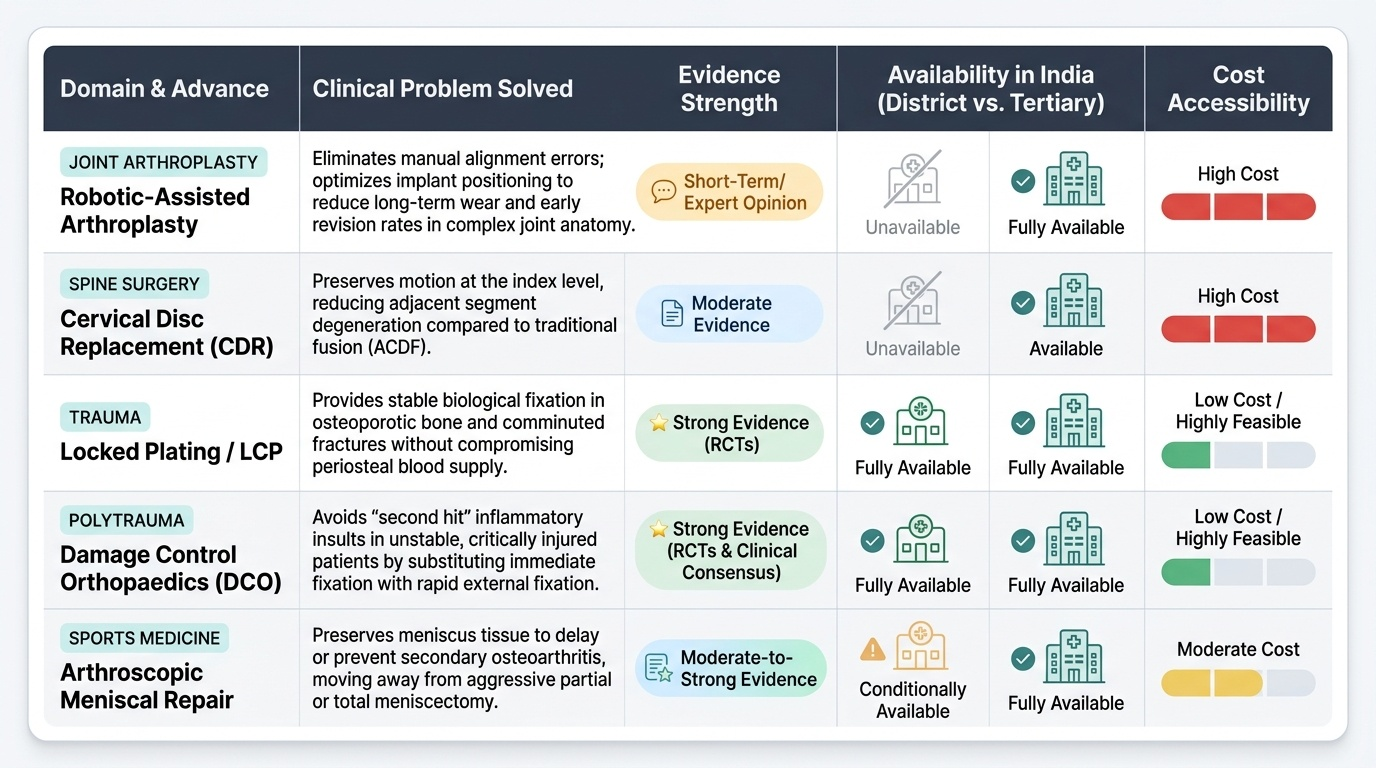
Understanding recent advances is not merely about knowing what is new — it requires the ability to critically appraise evidence, recognise the difference between a promising technique with short-term data and a proven standard-of-care advance, and apply this knowledge appropriately within the resource constraints of the Indian healthcare system. This section addresses the applied significance of the advances covered in this module and provides a framework for evaluating claims of innovation.
The Indian orthopaedic landscape is characterised by a significant urban-rural divide in access to tertiary care. Many of the advances described — robotic arthroplasty, cervical disc replacement, navigated spine surgery — are concentrated in metropolitan teaching hospitals and private sector tertiary centres. The district hospital orthopaedic surgeon must apply the principles of these advances with available resources: locked plating over conventional plating where implants are available, DCO principles for polytrauma even without CT navigation, arthroscopic meniscal repair over meniscectomy where arthroscopic equipment is accessible.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
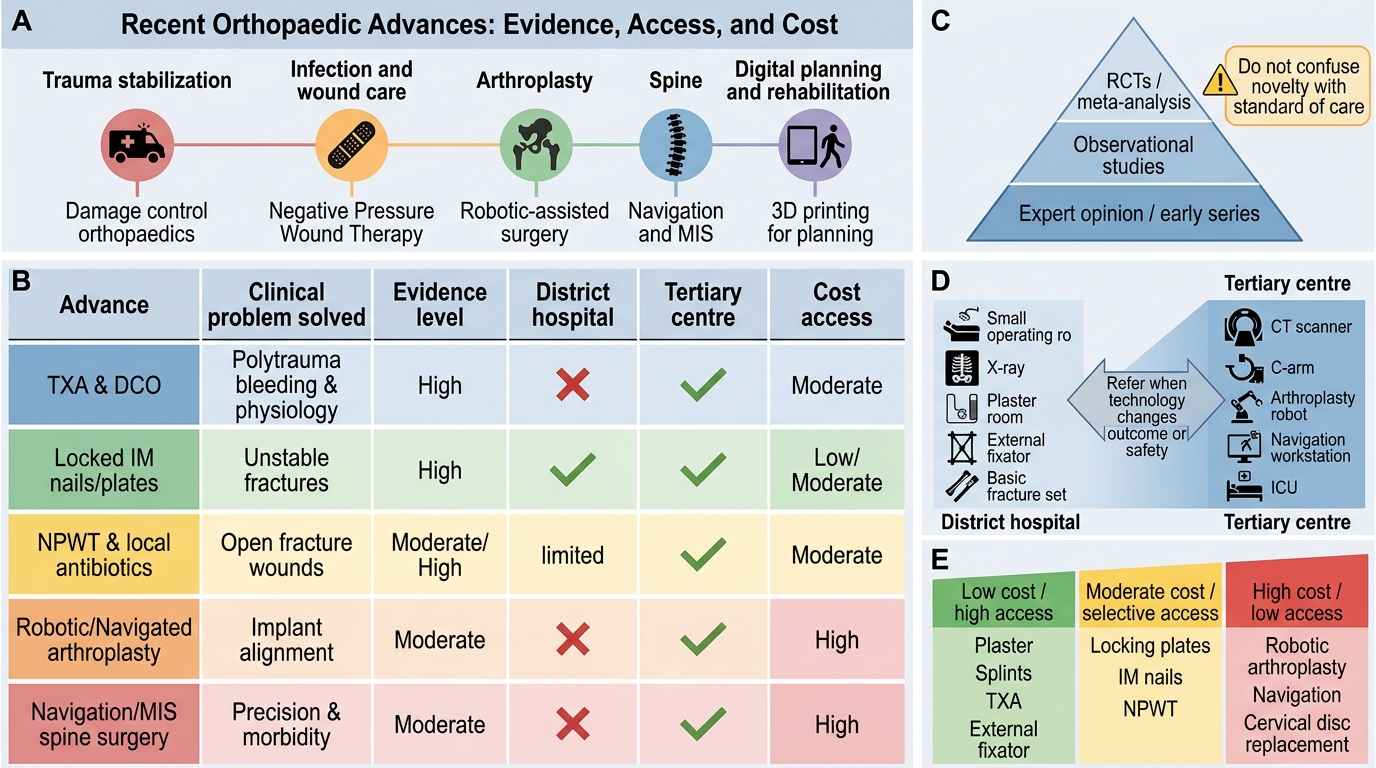
Recent Orthopaedic Advances: Evidence, Access, and Cost
Applying critical appraisal to orthopaedic advances:
- Platelet-rich plasma (PRP): widely marketed and commercially available; heterogeneous preparation protocols and variable clinical trial quality make evidence interpretation difficult. Current consensus: moderate evidence for lateral epicondylitis; insufficient evidence for routine use in ACL, cartilage, and most tendinopathies. Do not recommend based on patient demand alone.
- Metal-on-metal hip implants: a widely adopted advance (large-head CoC bearings for hip resurfacing) that was later found to cause cobalt-chromium systemic toxicity (ALVAL — adverse local tissue reaction) and required mass recall. Lesson: long-term follow-up data are essential before widespread adoption.
- BMP in spine fusion: FDA-approved for ALIF (anterior lumbar interbody fusion); off-label use in posterolateral and cervical fusion associated with increased complication rates (ectopic bone, oedema, dysphagia). The 'Spine Journal' 2011 special issue exposed industry-sponsored data manipulation in BMP trials. Critical reading of funding sources is mandatory.
The role of registries in evaluating arthroplasty: national joint registries (Australian, UK, Swedish, Nordic) track every implant inserted and every revision, generating long-term population-level data on implant survival. These registries have driven rapid recall of poorly performing implants (e.g., metal-on-metal bearings, early ceramic-on-ceramic designs that fractured) and have defined which implant combinations carry the best 10, 15, and 20-year survival. India lacks a comprehensive national arthroplasty registry — an evidence gap that affects our ability to appraise implant performance in our population.