Page 6 of 26
OR1.2 | Shock in Orthopaedic Trauma — SDL Guide (Part 2)
Investigations in Traumatic Shock
The clinical evaluation of shock must be supported by targeted investigations that quantify the degree of haemorrhage, guide resuscitation, and detect occult injuries contributing to the haemodynamic instability. These investigations should be obtained rapidly and in parallel with ongoing resuscitation — not used to delay treatment. The discipline of ordering only what is immediately actionable is itself a management skill: a FAST ultrasound and a blood gas take minutes and change immediate decisions; a full metabolic panel takes half an hour and changes nothing in the first hour. Understanding the clinical utility and timing of each investigation allows a doctor to act on early results while awaiting those that take longer, without either over-investigating (delaying resuscitation) or under-investigating (missing occult haemorrhage).
Primary haematological investigations are obtained from a single venepuncture at IV cannula insertion:
- Full blood count (FBC): haemoglobin and haematocrit are UNRELIABLE in the acute phase of haemorrhage because haemodilution takes several hours; do not be reassured by a normal Hb in early haemorrhagic shock
- Coagulation profile (PT, APTT, INR): establishes baseline; trauma-induced coagulopathy may be present even at initial presentation in severe polytrauma
- Serum lactate: most sensitive marker of tissue hypoperfusion; lactate >2 mmol/L indicates significant shock even with normal vital signs; serial lactate guides response to resuscitation
- Arterial blood gas (ABG): base deficit <-6 mEq/L correlates with Class III/IV shock and the need for massive transfusion; pH <7.35 indicates established metabolic acidosis
- Blood group and cross-match: type O-negative blood is given in exsanguinating shock while type-specific blood is being prepared
- Urea, creatinine, electrolytes: baseline renal function; hyperkalaemia may accompany massive haemorrhage and rhabdomyolysis
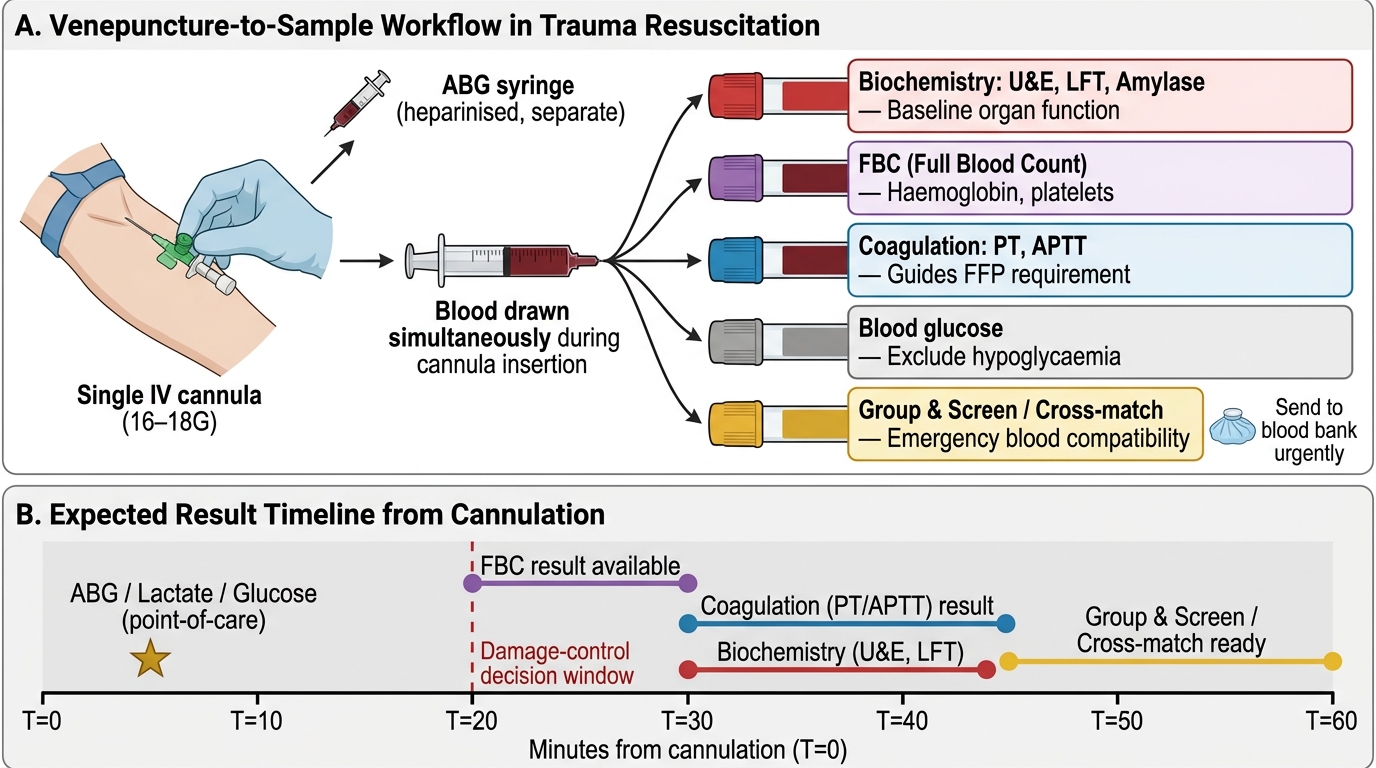
Venepuncture-to-Result Workflow in Trauma Resuscitation
Bedside investigations during primary survey:
- FAST ultrasound: detects free intraperitoneal or pericardial fluid; a positive FAST in a haemodynamically unstable patient mandates immediate operative haemorrhage control
- Chest and pelvis X-rays: portable, AP views that detect haemothorax, pneumothorax, and pelvic ring disruption
Extended investigations (in stabilised patients):
- CT scan with contrast (pan-scan): head, chest, abdomen, pelvis; identifies all injury sources; only for haemodynamically stable or transiently responsive patients
- CT angiography: identifies active arterial haemorrhage amenable to interventional radiology embolisation (especially for pelvic fractures)
Management of Haemorrhagic Shock: Principles
The management of haemorrhagic shock integrates two simultaneous strategies: resuscitation (restoring circulating volume to reverse ischaemia) and source control (stopping the haemorrhage that is causing the volume loss). Resuscitation alone is futile if the source is not controlled — pouring fluid into an open drain. Conversely, source control is unsuccessful if the patient does not survive long enough to reach operative haemorrhage control. These two goals are pursued in parallel by the trauma team. For the orthopaedic surgeon specifically, source control includes a range of immediately available mechanical interventions — pelvic binder, traction splint, tourniquet, wound packing — that can be deployed in the resuscitation bay before the patient reaches theatre. Understanding which intervention applies to which injury pattern is the practical clinical skill that translates physiological knowledge into reduced mortality.
Immediate haemorrhage control measures:
- External compression: direct pressure on accessible wounds, tourniquet for extremity haemorrhage (apply proximally, note time, never remove in field)
- Pelvic binder: applied at the level of the greater trochanters for suspected open-book pelvic fractures, reducing pelvic volume and tamponading venous haemorrhage
- Fracture splinting: immobilising the femur (traction splint) or tibia reduces ongoing haemorrhage from fracture ends and surrounding muscle injury; a Thomas splint can reduce femoral shaft blood loss by approximately 500–700 mL
- Damage control surgery: packing retroperitoneal haematoma, ligating bleeding vessels, temporary external fixation of unstable pelvic fractures
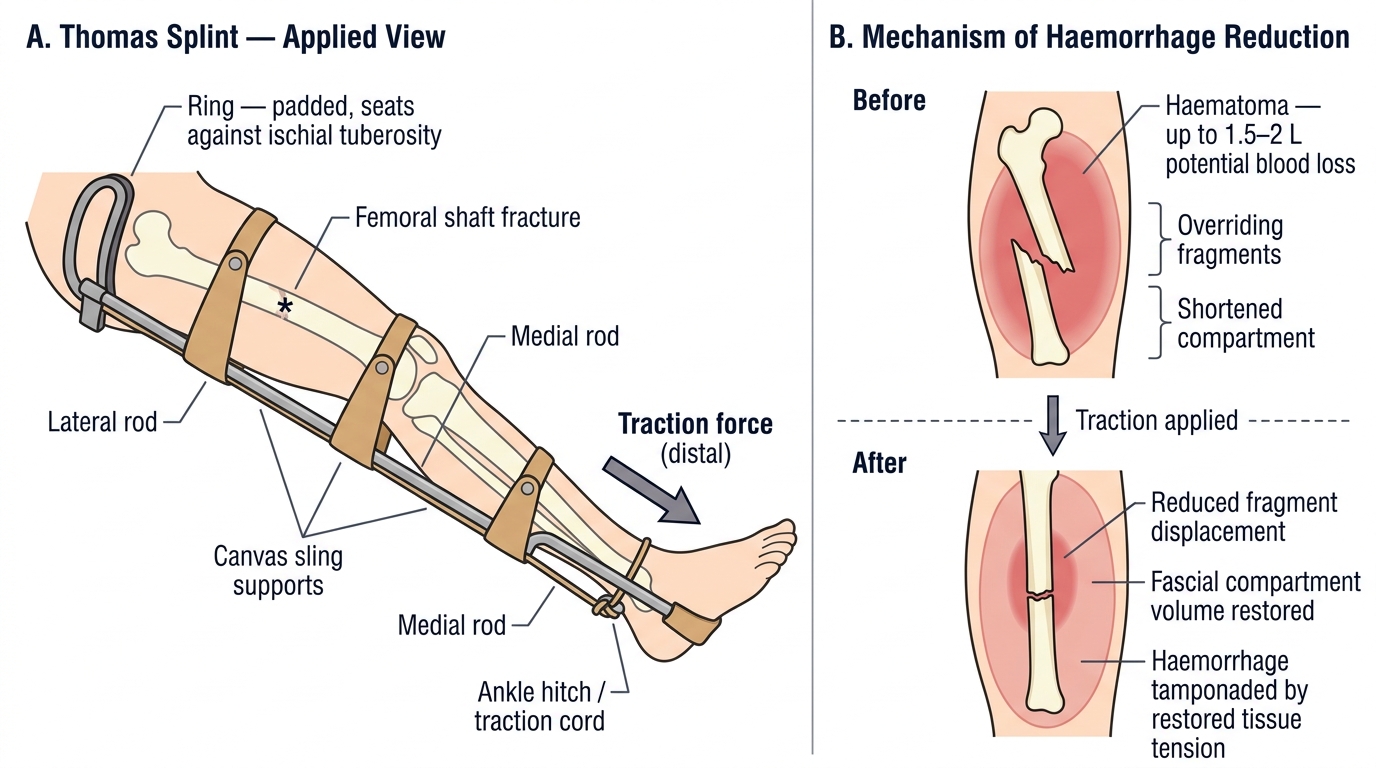
Thomas Splint Application and Mechanism of Haemorrhage Reduction in Femoral Shaft Fracture
Fluid resuscitation — the modern approach:
Traditional ATLS teaching of 2 litres of crystalloid as the initial resuscitative bolus has been substantially revised. Current evidence supports:
1. Haemostatic resuscitation (damage control resuscitation): early 1:1:1 ratio of packed red blood cells (pRBC) : fresh frozen plasma (FFP) : platelets, to address haemorrhage AND coagulopathy simultaneously
2. Permissive hypotension: in penetrating trauma without traumatic brain injury, targeting systolic BP 80–90 mmHg until operative haemorrhage control, to avoid dislodging provisional clots and worsening coagulopathy. Contraindicated in traumatic brain injury (requires adequate cerebral perfusion pressure)
3. Limit crystalloid: restrict to <1.5 L in haemorrhagic shock; large volumes cause dilutional coagulopathy, hypothermia, and abdominal compartment syndrome
4. Tranexamic acid (TXA): 1 g IV over 10 minutes within 3 hours of injury (CRASH-2 evidence), followed by 1 g over 8 hours; reduces fibrinolysis and all-cause mortality
5. Warming: all IV fluids through a warming device; hypothermia below 35°C critically impairs coagulation cascade enzyme function
Vasopressors (noradrenaline, vasopressin) have a limited role in haemorrhagic shock — they cannot compensate for depleted intravascular volume. They are appropriate as a bridge in neurogenic shock (low SVR, bradycardia) and in refractory haemorrhagic shock while blood products are being prepared.
Monitoring response to resuscitation: urine output ≥0.5 mL/kg/h, improving GCS, decreasing heart rate, improving pulse pressure, normalising lactate (serial measurements) and base deficit (ABG) are the targets. A patient who does not respond to initial resuscitation has ongoing haemorrhage and needs immediate operative intervention.
Neurogenic Shock: Recognition and Differentiation
Neurogenic shock results from disruption of the descending sympathetic pathways in the spinal cord, typically following cervical or high thoracic (above T6) spinal cord injury. Loss of sympathetic tone causes simultaneous peripheral vasodilation (reduced SVR) and loss of cardiac chronotropic sympathetic drive. The result is a haemodynamic pattern that is distinctly different from haemorrhagic shock and must be recognised to avoid the treatment error of massive fluid resuscitation.
The classic presentation of neurogenic shock is the triad of hypotension + bradycardia + warm, flushed, dry peripheries. This contrasts with haemorrhagic shock, where hypotension is invariably accompanied by tachycardia, vasoconstriction (cool peripheries, prolonged capillary refill), and pallor. The paradox of a slow heart rate in a hypotensive trauma patient is the single most important distinguishing feature: the sympathetic loss prevents the compensatory tachycardia that haemorrhage would otherwise produce.
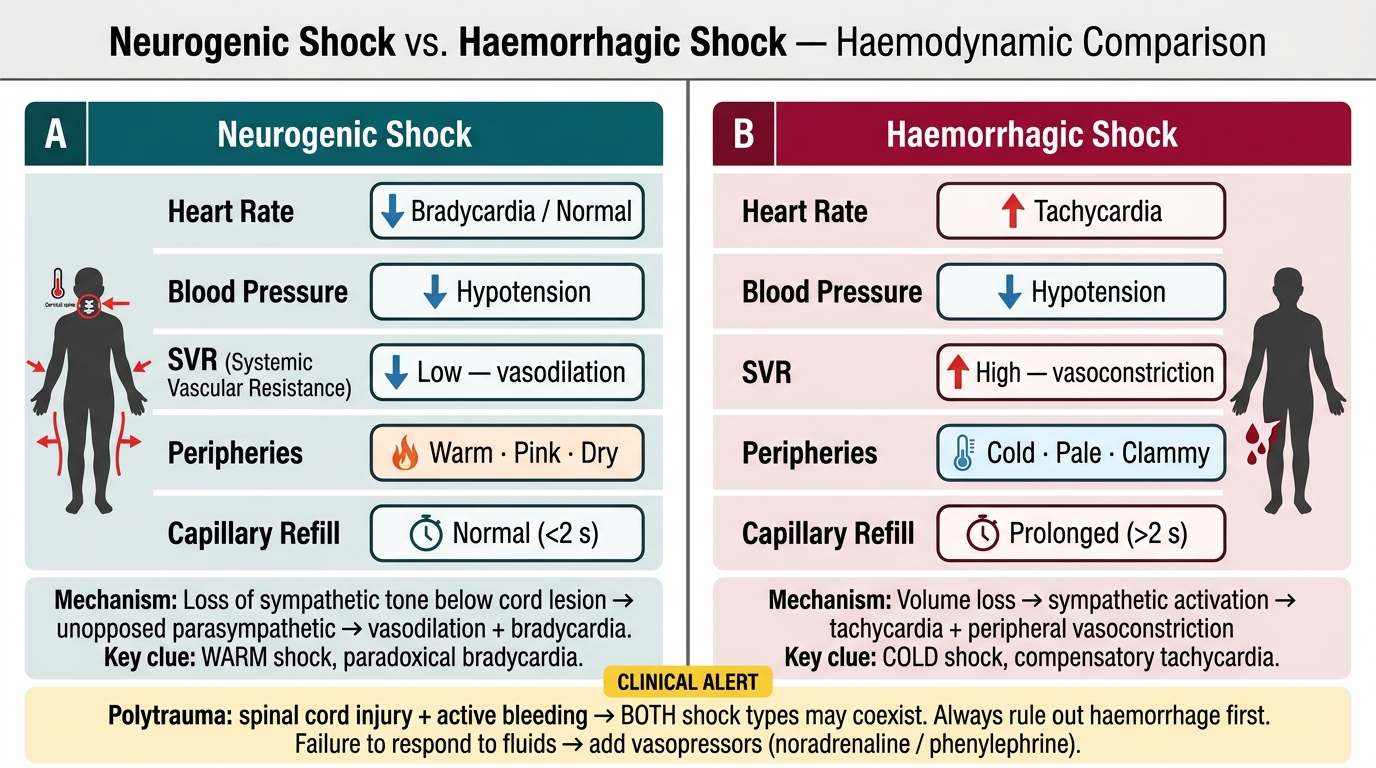
Neurogenic Shock vs. Haemorrhagic Shock — Haemodynamic Parameter Comparison
Practical management of neurogenic shock:
- Rule out haemorrhagic shock first: a spinal cord–injured patient with hypotension may have BOTH neurogenic and haemorrhagic shock (polytrauma is common). Start with fluid resuscitation; if BP does not respond appropriately, consider vasopressors
- Vasopressors (noradrenaline or phenylephrine): to restore SVR and MAP; phenylephrine avoids the bradycardia-worsening effect of agents with no chronotropic activity
- Atropine: if bradycardia is symptomatic or causing further haemodynamic compromise
- Target MAP ≥85–90 mmHg in the acute phase of spinal cord injury to maintain spinal cord perfusion pressure and minimise secondary cord injury
- Avoid hypothermia and hypoxia: both worsen secondary spinal cord injury
Spinal shock is a different concept and must not be confused with neurogenic shock. Spinal shock refers to the transient loss of all spinal cord function (including reflexes) below the level of injury immediately after cord trauma. It lasts hours to weeks and is a neurological rather than haemodynamic phenomenon. The bulbocavernosus reflex (anal sphincter contraction in response to glans penis or clitoris squeeze, or urinary catheter tug) returns first as spinal shock resolves; return of this reflex means the injury is at the final segment and any absent function below is likely permanent.
SELF-CHECK
A 55-year-old man falls from a ladder and is brought in with neck pain. BP 80/50 mmHg, HR 54/min, RR 16/min, GCS 15. His hands are warm and pink. There is no obvious external bleeding. What is the most likely diagnosis and the key management step?
A. Class III haemorrhagic shock — give 2 L crystalloid immediately
B. Neurogenic shock from high spinal cord injury — vasopressor support and targeted MAP ≥85 mmHg
C. Cardiogenic shock — bedside echocardiography urgently
D. Class II haemorrhagic shock — 1:1:1 blood product resuscitation
Reveal Answer
Answer: B. Neurogenic shock from high spinal cord injury — vasopressor support and targeted MAP ≥85 mmHg
The combination of hypotension WITH bradycardia (HR 54/min) and warm, flushed peripheries in a patient with neck trauma is the classic triad of neurogenic shock. Haemorrhagic shock causes TACHYCARDIA (sympathetic compensation), not bradycardia — this distinction is the key diagnostic clue. Management is vasopressors (to restore SVR), maintaining MAP ≥85–90 mmHg for cord perfusion, and excluding concurrent haemorrhagic shock. Fluid resuscitation alone will not correct neurogenic shock and risks pulmonary oedema.