Page 2 of 14
OR14.1-2 | Orthopaedic Prognosis and Consent Counselling — SDL Guide (Part 2)
Reading Patient Cues and Adapting the Consultation
The ability to 'read' a patient's cognitive and emotional state during a prognosis or consent consultation — and to adapt accordingly — is what distinguishes a skilled communicator from a technically competent one. This interpretive skill is not instinctive; it is learnable through deliberate observation and practice.
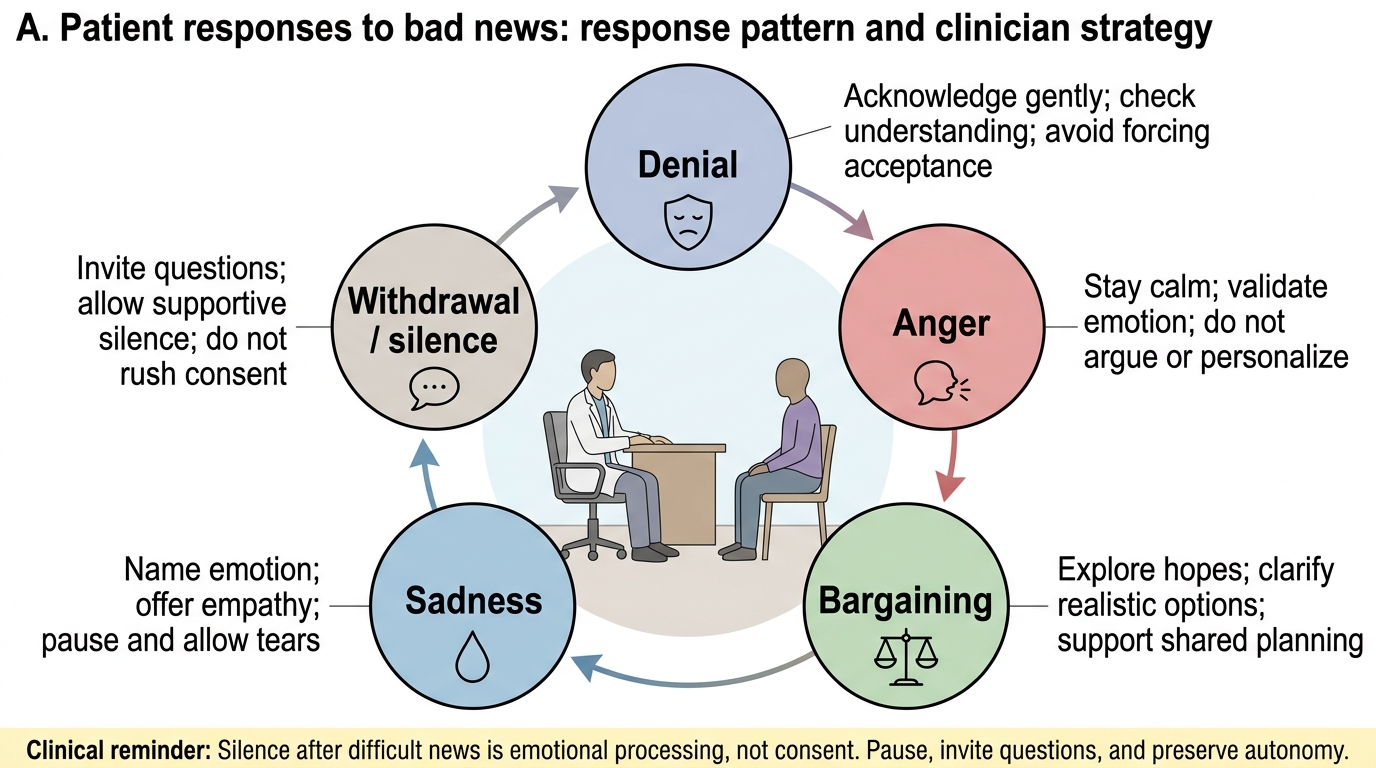
Patient responses to difficult news cluster into five recognisable patterns, each requiring a distinct response. Denial ('Are you sure? Can we run more tests?') is a protective mechanism, not a cognitive failure. Acknowledge the disbelief without reinforcing it: 'I understand this is very hard to accept. I wish I had different news. We have reviewed all the investigations carefully and this is what they show.' Anger (directed at the clinician, the referring doctor, or 'the system') often masks profound fear or grief. Avoid defensiveness. A quiet, non-retaliatory acknowledgment ('I can hear how angry you are, and I am sorry this has happened to you') typically de-escalates far more effectively than a factual correction of the patient's grievance. Bargaining ('If I just try this treatment first, maybe we can avoid amputation') should be engaged factually and respectfully — present why the alternative the patient is proposing is not appropriate in their case. Sadness and tearfulness require the clinician to stop, offer a moment of silence, and use a verbal empathy statement — not physical touch (which can be misread) and not a box of tissues as a substitute for engagement. Withdrawal (the patient who goes very quiet and stops asking questions) is the most dangerous pattern because it can be misread as acceptance. Explicitly invite further questions: 'This is a lot to take in. What questions do you have right now?' and 'Is there anything you did not understand that you would like me to explain again?'
Non-verbal cues carry more information than verbal content. Leaning forward, maintaining eye contact, and matching the patient's speech pace signals presence and attentiveness. A clinician who remains standing, glances at their phone, or uses jargon while the patient's face shows confusion has failed the consultation regardless of the accuracy of the information delivered. Train yourself to observe: furrowed brows (confusion), lip-biting (anxiety), avoidance of eye contact (shame or cultural deference), and the family member who keeps interrupting (often indicating they have already been told information the patient has not).
Cultural and family dynamics in the Indian context: In many Indian families, senior family members (parents, in-laws, spouse) expect to be informed before or simultaneously with the patient. This creates a tension with the Western bioethical principle of individual autonomy. The legally correct position under Indian law is that competent adult patients have the right to receive their own information first and to decide what their family is told. However, the clinician must navigate this sensitively. Ask the patient privately before the family meeting: 'How much would you like your family to know, and how much do you want to manage yourself?' This respects autonomy while acknowledging the relational context in which most Indian patients live their medical decisions.
Language and literacy: In India's linguistically diverse healthcare settings, assuming that a patient who nods understands is a dangerous practice. Use a trained interpreter (not a family member, who may editorially filter distressing information) when the patient does not share a language with the clinician. Validate comprehension using the 'teach-back' method: 'Can you tell me in your own words what we decided today?' — not 'Do you understand?' (to which patients almost always say yes).
Patient Responses to Bad News and Communication Strategies
SELF-CHECK
During a consent conversation for below-knee amputation, the patient goes completely silent after you explain the procedure. The most appropriate next action is:
A. Hand the patient the consent form to sign since continuing is distressing
B. Invite further questions explicitly and allow silence before speaking
C. Move on to explaining rehabilitation to give the patient something positive to focus on
D. Call the family in immediately to help persuade the patient
Reveal Answer
Answer: B. Invite further questions explicitly and allow silence before speaking
Patient silence after difficult news most likely represents emotional processing, not acceptance or agreement. The correct response is to invite explicit questions and hold a moment of supportive silence before speaking — this signals presence and gives the patient agency to re-enter the conversation. Signing the form at this moment would not constitute valid informed consent (the emotional state may impair processing). Moving to rehabilitation prematurely shuts down the patient's emotional response. Calling in the family without the patient's permission undermines autonomy and may introduce pressure.
Applied and Supervised Practice: Conducting Prognosis and Consent Conversations
Competence in prognosis and consent counselling is built through supervised practice with real patients and structured debriefing — reading about the SPIKES protocol cannot substitute for the moment of sitting across from a patient whose face you must watch while delivering news that will change their life. This section provides the framework for structured clinical practice that you should pursue during your orthopaedic posting.
Observed ward round participation: In your orthopaedic posting, identify opportunities to observe your consultant or registrar delivering prognosis information or obtaining consent for major procedures. Position yourself in the room where you can observe both the clinician and the patient simultaneously. After the consultation, note: Did the clinician use SPIKES steps, even implicitly? How did the patient respond? Which step was handled least smoothly? What would you have done differently? Discuss with your supervisor.
Supervised consent taking: Under supervision of a registrar or consultant, take the consent for an elective orthopaedic procedure (total knee replacement, elective plating) from a patient who has already had the initial prognosis discussion with the operating surgeon. This is the standard training pathway: you conduct the consent documentation process while the treating surgeon remains available. You are responsible for answering questions about the procedure, confirming understanding, and completing the form correctly. Your supervisor should debrief you on your communication style, not just the completeness of the form.
Simulated patient practice with role-play is used in many medical schools for exactly this scenario. If your department has a clinical skills facility with standardised patients, request a session specifically for 'breaking bad news in orthopaedics'. Use the SPIKES structure, record if possible (with consent), and review your non-verbal communication.
Documentation practice: Review blank consent forms used in your hospital for orthopaedic procedures. Identify the deficiencies — do they name specific risks? Is there a space for the patient's questions? Is the language accessible? Compare with the ideal elements of valid consent discussed in arc step 2. Write a sample consent documentation note for a patient undergoing below-knee amputation for severe crush injury, including what you disclosed, the patient's questions and your answers, and how you confirmed understanding.
Self-monitoring tools used in communication training include the SPIKES adherence checklist (available from the Oncology-related literature of Baile et al.) and the Calgary-Cambridge Communication Guide. Even in your clinical practice post-internship, periodic use of these frameworks as self-assessment tools helps prevent the communication shortcuts that accumulate over years of clinical practice.
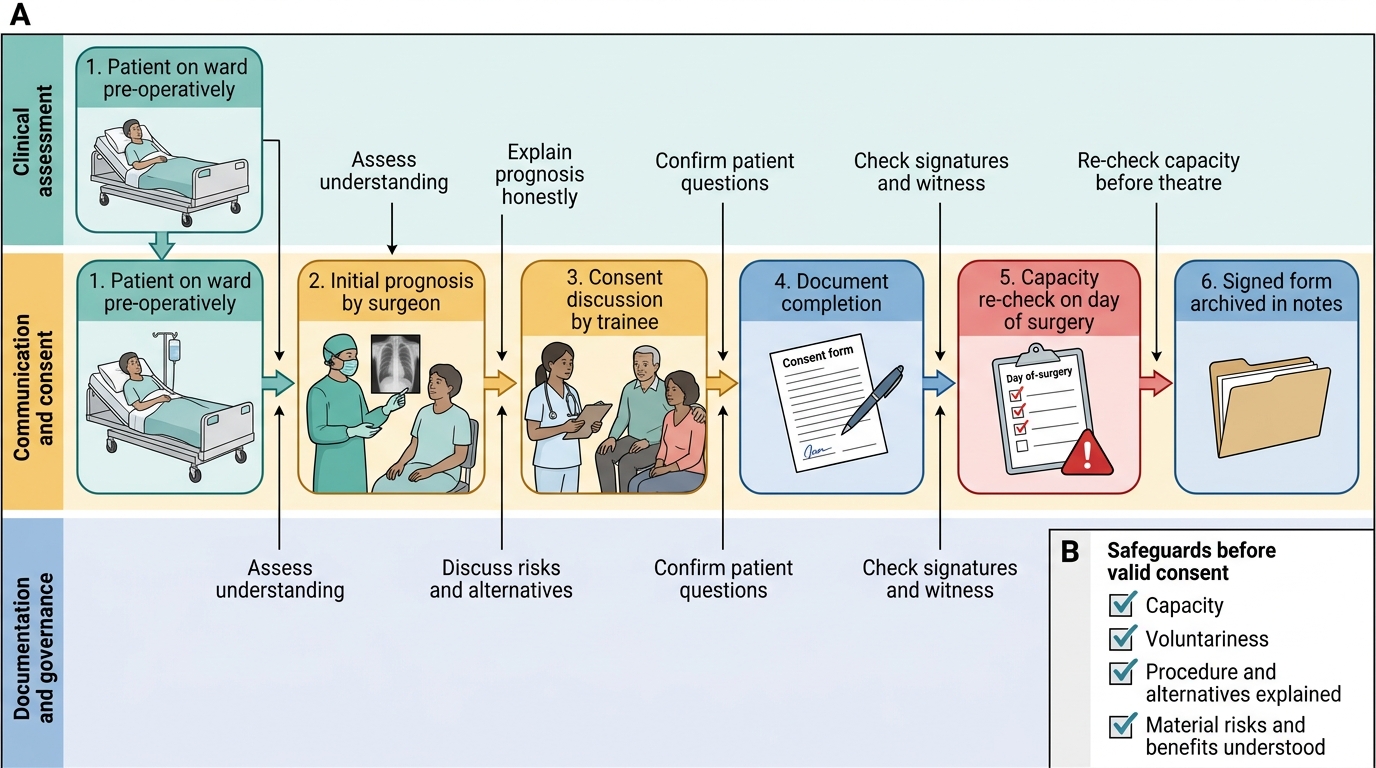
Orthopaedic Procedure Consent Pathway
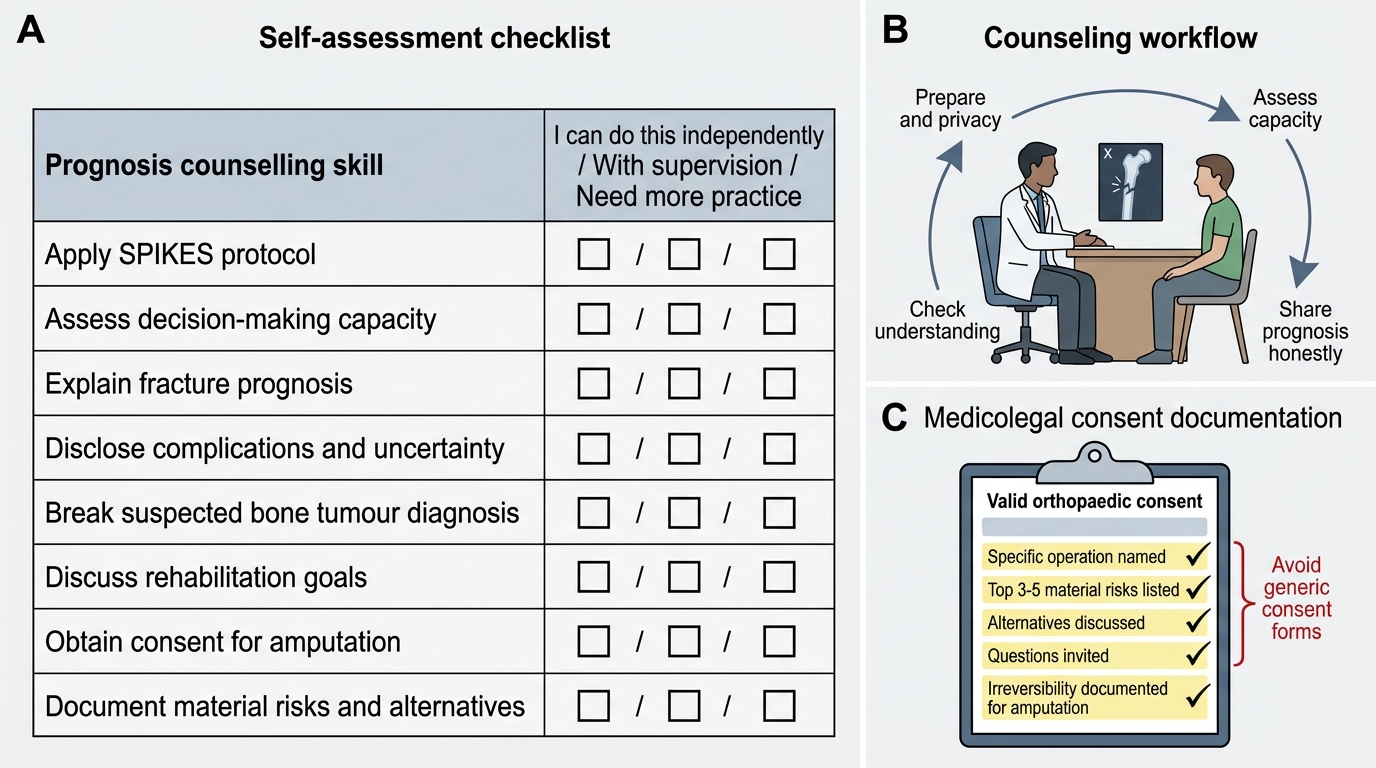
Self-Assessment: Consolidating Prognosis and Consent Skills
Self-assessment in communication skills requires a different methodology from factual recall — you cannot verify your counselling competence through a written test alone. The following structured self-assessment tasks use reflective practice and simulated scenarios to help you identify gaps before entering unsupervised clinical practice.
Work through each scenario below and formulate your response before reading the discussion:
Scenario A: A 60-year-old farmer with non-union of a mid-shaft femur fracture (three years after conservative treatment elsewhere) attends your outpatient clinic. He has been walking with a painful, mobile non-union site and has been told by his village-level practitioner that 'the bone will set eventually'. His family have brought him reluctantly. What prognosis do you give, and how do you structure the consent conversation for internal fixation + bone grafting?
Discussion: This scenario requires breaking the patient's false prior belief (the 'it will set eventually' expectation) before disclosing the actual prognosis. Use SPIKES Step P (assessing Perception) first — explore what the patient currently understands. The prognosis for established non-union with operative intervention is good (union rates >85% with appropriate fixation + grafting), so this is a scenario where honesty is reassuring, not distressing. Consent for this procedure must cover the risks of surgery under regional/general anaesthesia, implant failure, infection (especially relevant for a delayed case), and the possibility that the graft donor site (usually iliac crest) will be sore postoperatively.
Scenario B: A 14-year-old girl and her parents are told that she has a 7 cm osteosarcoma of the distal femur. The parents want to know the diagnosis but ask you not to tell their daughter until 'she is ready'. The patient herself looks at you and asks, 'Is it cancer?' How do you respond?
Discussion: A 14-year-old who is asking directly has demonstrated a desire to know. Under Indian law, a competent adolescent above 12 years has evolving capacity to be included in medical decisions, and most legal commentators hold that actively deceiving a direct question — particularly when the patient is aware something serious is wrong — undermines the therapeutic relationship and may later constitute a breach of duty. The correct approach is to ask the parents' permission to speak with the patient privately, then to honour her direct question honestly (using age-appropriate language), while remaining sensitive to the family's protective instinct. A social worker or child counsellor should be involved.
Scenario C: A 35-year-old bus driver with a crushing foot injury is told that Syme's amputation at the ankle joint is the recommended treatment. He refuses, saying his livelihood depends on driving. Using the four elements of valid consent, analyse what your obligations are in managing this refusal.
Discussion: A competent adult patient has the absolute right to refuse treatment, including life-altering surgery, provided the refusal is made with capacity, adequate information, and without coercion. Your obligation is to ensure the refusal is truly informed — that the patient understands what will happen if the limb is not amputated (likely persistent sepsis, pain, and potential systemic compromise), that alternatives were genuinely considered and found unsatisfactory, and that the patient is not making the decision under an emotional state that impairs capacity. Document the refusal conversation meticulously. Arrange follow-up. The patient may change their mind as consequences become clearer — do not interpret a refusal as a permanent decision.
Use these scenarios as benchmarks. If you found Scenario B or C difficult, revisit arc steps 2 and 4 of this module before your next clinical posting in orthopaedics.
Orthopaedic Prognosis Counselling Self-Assessment
CLINICAL PEARL
The single most common medico-legal error in orthopaedic consent is using a generic form that does not name the specific operation or disclose the material risks. Courts in India have consistently held that a signature on a form reading 'operation and anaesthesia as deemed necessary' does not constitute valid informed consent. Every consent form for a major orthopaedic procedure must name the operation specifically, list at minimum the top three to five material risks (with their approximate frequencies where known), state that alternatives were discussed, and record that the patient was given the opportunity to ask questions. In limb amputation cases, the documentation must additionally record that the patient was explicitly told the procedure is irreversible. A correctly completed consent form is your most important medicolegal protection — more reliable than memory of what was said in the consultation.