Page 4 of 14
OR14.3 | Referral Counselling for Orthopaedic Warning Signals — SDL Guide
Learning Objectives
- Identify the orthopaedic warning signals (red flags) that mandate urgent referral to a higher centre for acute osteomyelitis, septic arthritis, neurovascular injuries, and low back pain
- Explain to a patient why referral is necessary in terms they can understand, using language that conveys appropriate urgency without inducing panic
- Counsel a patient who initially refuses referral to accept transfer to a higher centre, addressing their specific concerns respectfully
- Distinguish between warning signals that require immediate referral and those where a monitored outpatient review is acceptable
- Document a referral communication including the clinical reason, urgency level, findings transmitted, and arrangements made
INSTRUCTIONS
Every year, limbs are lost and lives are shortened because warning signals were missed — or were recognised but not communicated to the patient in a way that convinced them to accept referral. In primary care and district hospital settings, you will frequently encounter orthopaedic conditions that exceed your local management capacity. Your most critical skill in those moments is not the diagnosis itself, but the ability to persuade the patient to accept referral quickly and safely. A patient who leaves your clinic saying 'I will think about it' is a patient at risk. This module develops your ability to detect orthopaedic red flags, understand why each signals a management emergency, and communicate that urgency clearly, honestly, and compellingly.
References
- Maheshwari's Essential Orthopaedics, 6th ed, Ch 15 (Bone and Joint Infections) and Ch 33 (Low Back Pain) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 2 (Infection) (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed, Ch 11 (Osteomyelitis) and Ch 28 (Spine) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 10-year-old boy is brought to your primary health centre with a three-day history of fever and right thigh pain. He is limping badly, and his mother reports he refused to walk this morning. His temperature is 38.9°C, the thigh is tender, and he looks systemically unwell. You have no X-ray machine and limited intravenous antibiotic supplies. You suspect acute osteomyelitis. The nearest tertiary centre is 80 km away and the family has spent their savings on the journey to reach you. The father looks at you and says, 'Can't you give him an injection and we will see how he is tomorrow?' What do you say?
WHY THIS MATTERS
Timely referral for orthopaedic emergencies is a patient-safety imperative, not an administrative nicety. Acute osteomyelitis treated with a delay of even 24–48 hours risks progression to chronic osteomyelitis, pathological fracture, or septicaemia. Septic arthritis untreated within hours causes enzymatic cartilage destruction that leads to permanent joint stiffness and avascular necrosis. Neurovascular injuries in fractures missed at the district level lead to limb loss. Low back pain with red flags may represent cord compression, malignancy, or spinal infection — delays in diagnosis allow irreversible neurological damage. As a primary care doctor, your referral counselling skill — your ability to identify these situations and then convince the patient to act — is a direct determinant of patient outcomes. The technical quality of the higher centre's care cannot reverse the harm caused by a day's hesitation.
RECALL
Before proceeding, activate your existing knowledge of the orthopaedic conditions in this module. Recall the classical clinical presentation of acute haematogenous osteomyelitis in a child — the typical age, the presenting features, and the most common causative organism (Staphylococcus aureus in most age groups; Group B Streptococcus in neonates). Recall the four cardinal signs of septic arthritis and how they differ from a reactive arthritis. Review your understanding of neurovascular assessment in a limb with a fracture — the six P's of compartment syndrome, the significance of absent distal pulses, and the nerve injuries associated with specific fractures. Recall the red flags for serious spinal pathology (tumour, infection, cauda equina) that distinguish them from mechanical low back pain. These are the clinical anchors for the warning-signal detection that this SDL makes explicit.
Clinical Indications for Urgent Referral: The Orthopaedic Warning Signals
Provided image
A warning signal (synonymous with 'red flag' in the spinal literature, and with 'limb-threatening sign' in trauma) is a clinical finding that indicates a pathological process likely to cause irreversible harm if managed with standard primary care resources or with delayed specialist review. The ability to systematically check for these signals during every relevant consultation — rather than waiting until the patient deteriorates — is the foundation of safe orthopaedic practice at all levels.
Four clinical scenarios generate the majority of urgent orthopaedic referral needs in primary and district hospital settings in India.
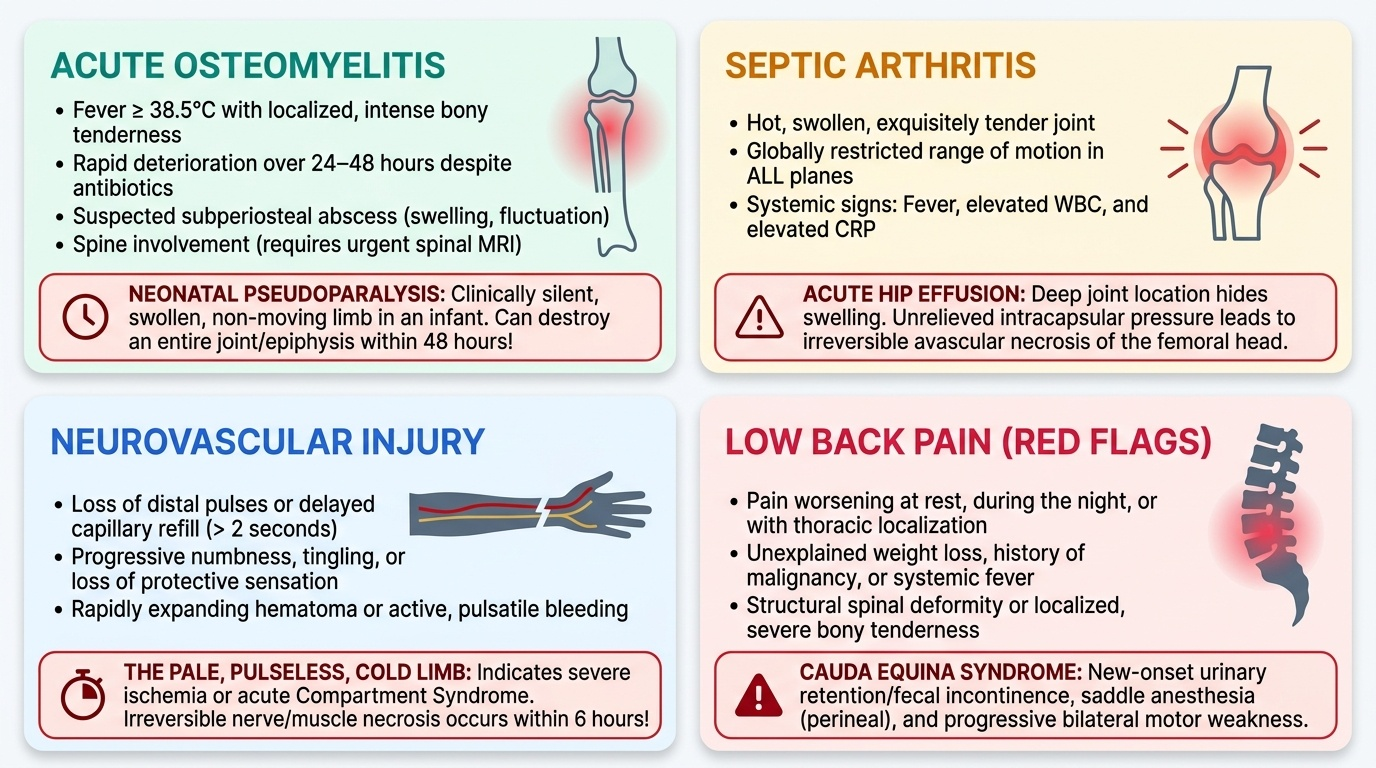
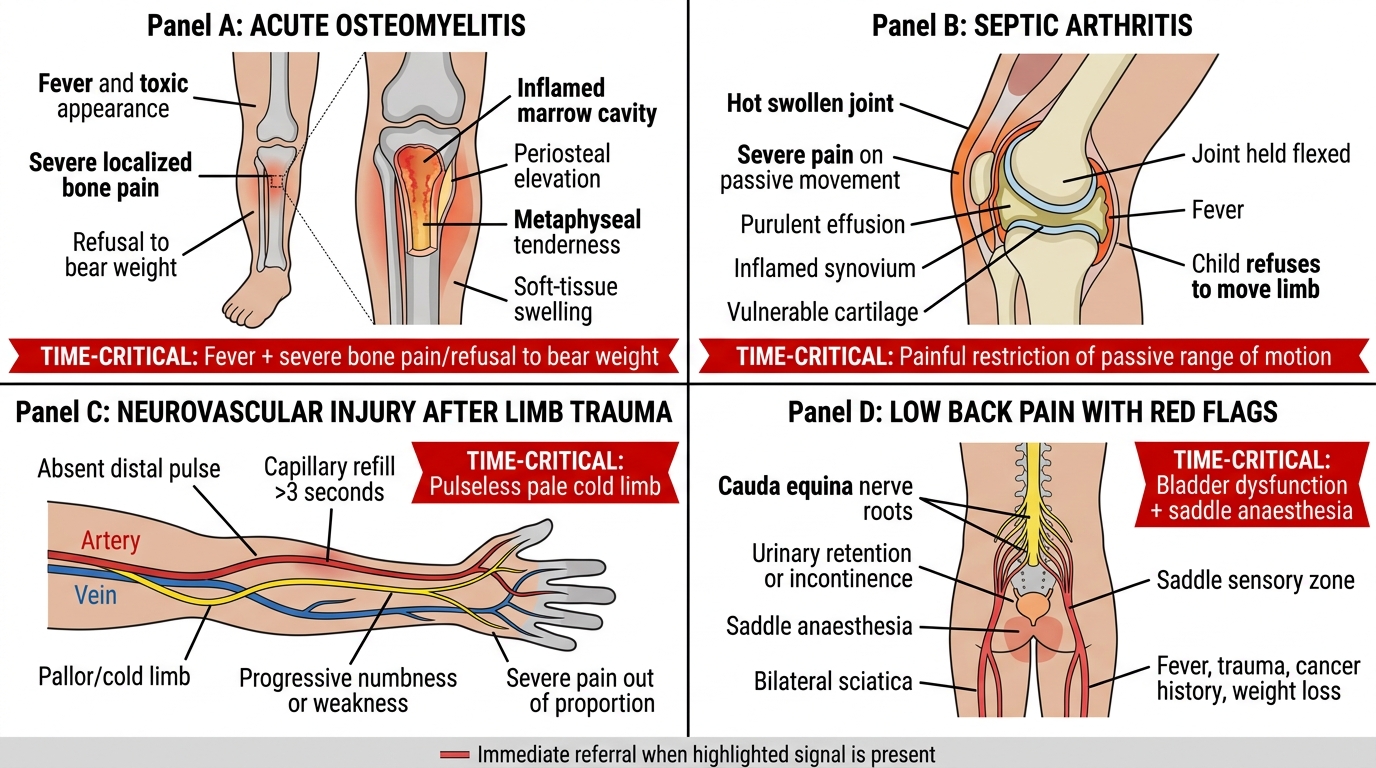
Acute osteomyelitis presents most commonly in children between 2 and 12 years, although it can affect any age group. Warning signals that mandate immediate higher-centre referral include: fever >38.5°C with localised bony tenderness (especially metaphyseal), rapid deterioration over 24–48 hours despite empirical antibiotics, suspicion of subperiosteal abscess formation (swelling, fluctuation), involvement of a vertebra (spinal osteomyelitis requires urgent MRI), and the toxic, systemically unwell child who is refusing to weight-bear. Neonatal osteomyelitis is a particular emergency — it is clinically silent (the infant is 'pseudoparalysed', not crying in pain) and can destroy an entire epiphysis within 48 hours. Any neonate with a swollen, non-moving limb is an emergency.
Septic arthritis is an orthopaedic emergency because joint cartilage begins to be destroyed by bacterial proteases within 8 hours of infection. The warning signals are: a hot, swollen, exquisitely tender joint with globally restricted movement in all planes (unlike a soft-tissue injury where movement in one plane is preserved), fever, and an elevated white cell count or CRP. The hip joint is the most dangerous location because it is deep, effusion is not visually apparent, and avascular necrosis of the femoral head occurs rapidly if the intracapsular pressure is not relieved. Any child or adult with a painful, flexed, externally rotated hip and fever should be treated as septic arthritis until proven otherwise, and referred immediately for joint aspiration and culture.
Neurovascular injuries in orthopaedic trauma generate warning signals that are time-critical. The key signals for immediate referral are: absent or diminished distal pulses after a fracture or dislocation (especially after knee dislocation — popliteal artery injury; or supracondylar fracture — brachial artery); progressive neurological deficit (numbness, weakness worsening over minutes to hours); the 6 P's of compartment syndrome (pain out of proportion to injury, pain on passive stretch of muscles in the compartment, pallor, paraesthesia, pulselessness, paralysis — noting that pulselessness and paralysis are late signs). The critical trap: a patient with compartment syndrome can have a palpable distal pulse in the early stages. A normal pulse does NOT exclude compartment syndrome — pain on passive stretch is the earliest reliable sign.
Low back pain with red flags is the spinal equivalent of the warning-signal framework. Mechanical low back pain (the vast majority of low back pain in adults) does not require referral. However, the following red flags indicate potentially serious spinal pathology and mandate urgent evaluation at a centre capable of MRI and specialist review: age >50 years with new-onset back pain; history of cancer (metastatic spinal disease); unexplained weight loss (malignancy or TB spine); fever with back pain (spinal infection — Pott's disease or pyogenic osteomyelitis); progressive bilateral leg weakness (cord compression or cauda equina); bladder or bowel dysfunction (cauda equina syndrome — sphincter disturbance is an emergency requiring same-day referral); back pain not relieved by rest (inflammatory, infective, or malignant aetiology); and night pain that wakes the patient (alarming for tumour).
Orthopaedic Emergency Warning Signals
Governing Principles: Why These Signals Demand Higher-Centre Resources
Effective referral counselling requires that you genuinely understand — not merely memorise — why each warning signal exceeds the capabilities of your setting. A clinician who knows the red flags but cannot explain the underlying pathophysiology to a patient (or to themselves) will be unconvincing in the referral conversation. This section establishes the mechanistic basis for each group of referrals.
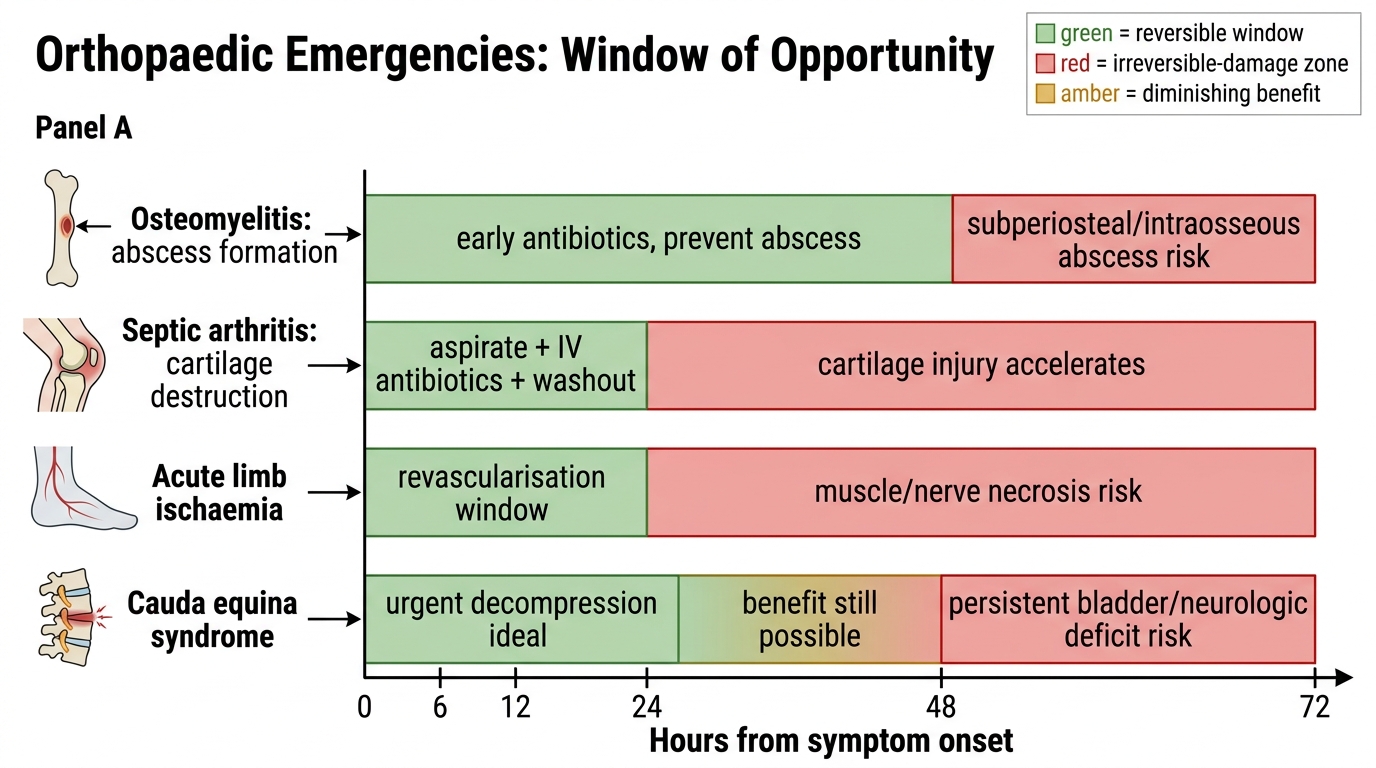
For acute osteomyelitis, the crisis point is the development of subperiosteal pus under raised pressure. Once pus accumulates beneath the periosteum, blood supply to the underlying cortex is compromised, leading to cortical necrosis and the formation of a sequestrum — a fragment of dead bone that cannot be treated with antibiotics alone and requires surgical sequestrectomy. At the primary care level, intravenous antibiotics in appropriate doses, blood culture before antibiotic administration, and surgical drainage of abscesses all require inpatient tertiary resources. Additionally, MRI — available only at higher centres — is required to delineate the extent of infection and plan surgery. A delay of even 48 hours in the systemically unwell child with suspected subperiosteal abscess converts a potentially curable infection into chronic osteomyelitis.
For septic arthritis, the mechanism of urgency is enzymatic destruction of articular cartilage. Bacteria (especially Staphylococcus aureus) release proteases and cytokines that degrade proteoglycans in hyaline cartilage within hours. Once cartilage is destroyed, it does not regenerate — the result is permanent joint stiffness, post-infective arthritis, or in the hip, avascular necrosis of the femoral head from elevated intracapsular pressure. The definitive management — joint aspiration for diagnosis and pressure relief, followed by washout if confirmed — requires an orthopaedic team, proper equipment, and anaesthesia support that is absent at most primary care centres.
For neurovascular injuries, the ischaemia time is the governing principle. Skeletal muscle tolerates approximately 6 hours of warm ischaemia before irreversible necrosis begins. An unrecognised arterial injury (popliteal artery after knee dislocation, brachial artery after supracondylar fracture) entering a primary care facility at hour 2 of ischaemia has only 4 hours to reach a vascular surgical team and undergo revascularisation. Compartment syndrome similarly requires fasciotomy within 6–8 hours of onset to prevent muscle necrosis, rhabdomyolysis, renal failure, and myonecrosis requiring amputation. These procedures cannot be performed at the primary care level — the patient needs emergency transfer.
For low back pain with red flags, the governing principle is that these presentations are surrogates for potentially serious structural pathology — cord compression, cauda equina syndrome, malignant infiltration, or vertebral destruction — each of which requires advanced imaging (MRI, CT) and specialist management (neurosurgery, oncology, spinal surgery). Cauda equina syndrome in particular is a surgical emergency: bladder dysfunction caused by cauda equina compression is reversible if operated within 24–48 hours of onset, but becomes permanent if surgery is delayed beyond 72 hours. The difference between continence and permanent incontinence is a same-day referral.
Emergency Windows of Opportunity
SELF-CHECK
A 7-year-old girl presents with a three-day history of right knee pain and fever. The knee is warm, swollen, and movement in all planes is severely restricted. Her CRP is 85 mg/L. The most appropriate action is:
A. Start oral amoxicillin and review in 48 hours
B. Aspirate the joint under sterile technique in the outpatient clinic and refer if the fluid is cloudy
C. Refer immediately to a centre capable of joint aspiration, culture, and operative washout
D. Arrange an X-ray and begin physiotherapy for possible soft tissue injury
Reveal Answer
Answer: C. Refer immediately to a centre capable of joint aspiration, culture, and operative washout
This presentation — warm swollen joint with globally restricted movement and elevated CRP in a febrile child — is septic arthritis until proven otherwise. Septic arthritis is an orthopaedic emergency requiring same-day joint aspiration (diagnostic and pressure-relieving), culture, and washout if confirmed. Oral antibiotics are insufficient — parenteral antibiotics must follow culture and are not a substitute for drainage. Outpatient aspiration without operative backup is inappropriate for a knee where the extent of infection is unknown. Physiotherapy for a hot swollen joint with fever is contraindicated. The correct action is immediate referral.
Counselling Technique: Convincing the Patient to Accept Referral
The referral counselling conversation is a negotiation between the patient's reasonable fears and practical constraints on one side, and the clinical imperative for timely higher-care on the other. Done well, it is one of the highest-impact clinical interactions you will have — done poorly, it leads to the delayed presentations that dominate district hospital case morbidity.
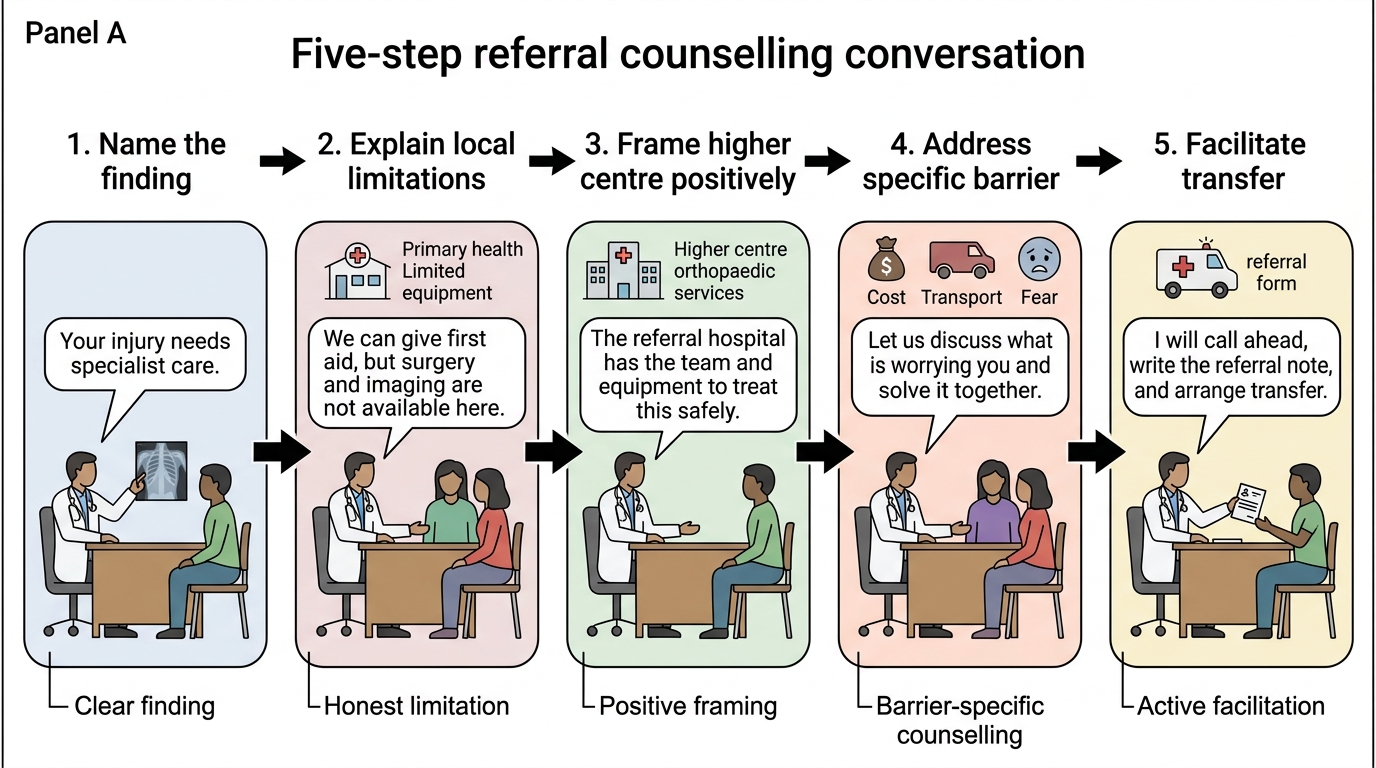
The referral conversation has a predictable five-part structure, which you should internalise and execute in this sequence:
Step 1 — Name the finding and its significance: Begin by being explicit about what you have found. Do not obscure the urgency with hedging language. 'I have examined your son carefully, and I am concerned that he may have an infection inside the bone of his thigh. This type of infection, if it spreads, can cause permanent damage to the bone and make him seriously ill.' Patients who are not told why they are being referred frequently minimise the urgency themselves ('Oh, the doctor said to go, but it can wait till Monday').
Step 2 — Explain what you cannot do here: Be honest about your facility's limitations without undermining your own competence or the patient's confidence in district-level care. 'We do not have the equipment here to do the specialised test (MRI/blood culture/joint aspiration under proper conditions) that this needs. This is not something that can wait — he needs this test today.'
Step 3 — Explain what the higher centre can do: Frame the referral positively. 'At the medical college hospital, they have an orthopaedic team and an operation theatre available now. If they confirm this infection, they can start the right intravenous antibiotics immediately and, if needed, do a small procedure to drain the infection before it causes permanent harm.'
Step 4 — Address the specific barrier the patient names: The commonest barriers to referral acceptance are financial cost, distance and transport, fear of losing work or income, distrust of large hospitals, and the belief that 'injections here will be enough'. Each barrier requires a targeted, empathic response — not dismissal. For financial barriers: 'I understand this is difficult. Let me write a referral letter that says this is an emergency — under Ayushman Bharat/government scheme he may be covered. Do you have a family member who can accompany him?' For the 'we'll wait and see' response: 'I hear that this seems like a lot of trouble. I want to be honest with you — if this infection spreads into the joint, which can happen in the next few hours, the damage becomes permanent. I cannot undo that. But the team at the higher centre can, if we go now.'
Step 5 — Facilitate the transfer actively: A referral counselling conversation that ends with 'go to this address' is incomplete. Write the referral letter before the patient leaves your clinic. Call ahead to the receiving centre if possible (particularly for vascular or compartment emergencies where a team needs to be prepared). Give the patient the letter in their hand and check they know where to go. If the patient has no transport, identify whether local ambulance services (108 in most Indian states) are available. In extremis — if a patient with an arterial injury or cauda equina syndrome is hesitating — ask a senior colleague to re-enforce the message; a second voice often tips the decision.
Referral Counselling Conversation: Five-Step Structure