Page 3 of 17
OR2.14 | Fracture Complication Investigation — SDL Guide (Part 3)
Principles of Management of Non-union and Malunion
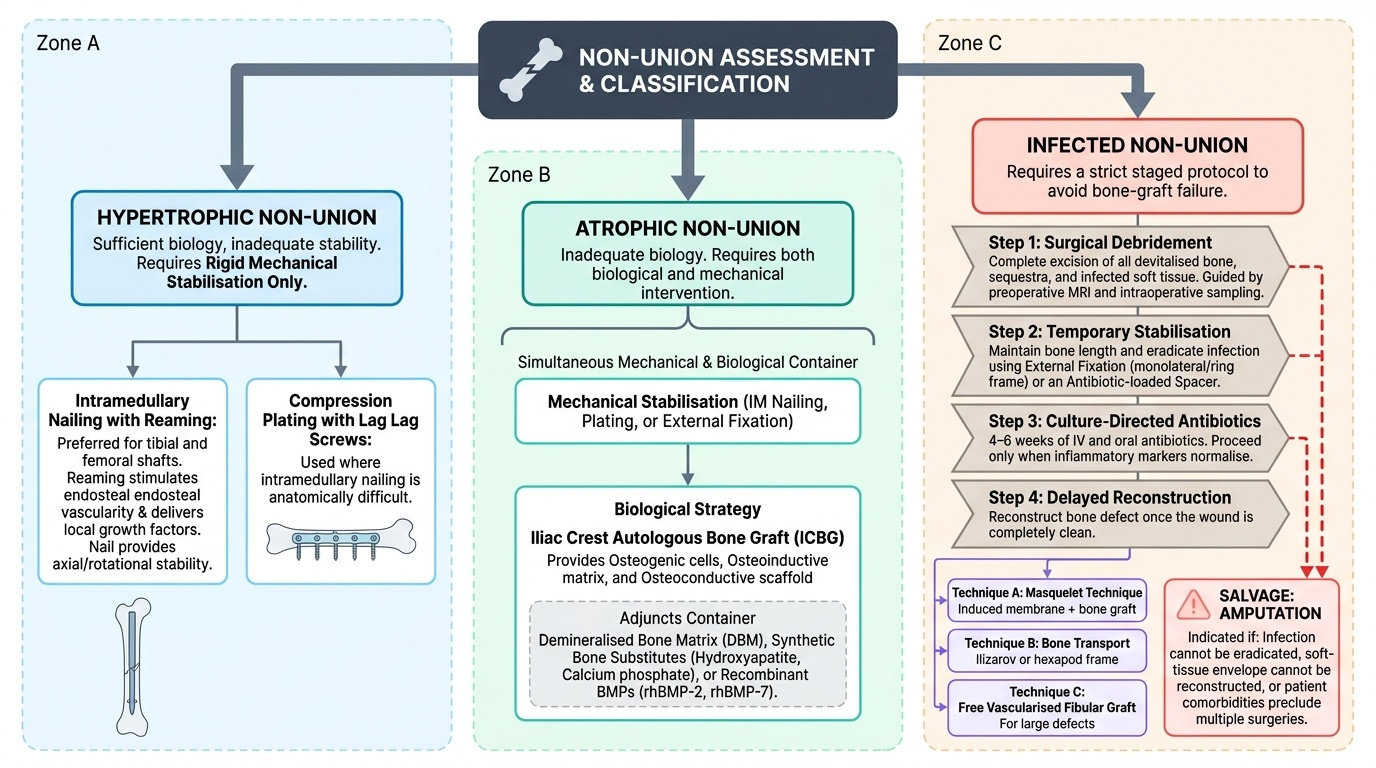
Management of non-union is governed by the Weber–Cech type. Hypertrophic non-union responds predictably to rigid mechanical stabilisation alone. Intramedullary nailing with reaming is the preferred technique for tibial and femoral shaft hypertrophic non-unions — reaming stimulates endosteal vascularity and delivers local growth factors while the nail provides axial and rotational stability. Compression plating with lag screws is used where nailing is anatomically difficult. Atrophic non-union requires both biological and mechanical intervention. The standard biological strategy is iliac crest autologous bone graft (ICBG), which provides osteogenic cells, osteoinductive matrix proteins, and osteoconductive scaffold — all three components that atrophic bone lacks. Adjuncts include demineralised bone matrix (DBM), synthetic bone substitutes (hydroxyapatite, calcium phosphate), and recombinant bone morphogenetic proteins (rhBMP-2, rhBMP-7) for difficult cases. Mechanical stabilisation by intramedullary nailing, plating, or external fixation is simultaneously required. Infected non-union demands a strict staged protocol to avoid bone-graft failure: (1) surgical debridement — complete excision of all devitalised bone, sequestra, and infected soft tissue, guided by preoperative MRI and intraoperative sampling; (2) stabilisation of the debrided segment by external fixation (ring fixator or monolateral fixator) or antibiotic-loaded spacer to maintain length while eradicating infection; (3) culture-directed intravenous and oral antibiotics for 4–6 weeks until inflammatory markers normalise; (4) reconstruction of the bone defect once the wound is clean — Masquelet technique (induced membrane + bone graft), bone transport by Ilizarov/hexapod frame, or free vascularised fibular graft for large defects. Amputation remains a salvage for cases where the infection cannot be eradicated, the soft-tissue envelope cannot be reconstructed, or the patient's comorbidities preclude multiple reconstructive surgeries. Malunion is managed by corrective osteotomy at the apex of the deformity, combined with stabilisation by plate, nail, or external fixator. The aim is to restore normal mechanical axis, limb length, and rotational alignment. In children, partial remodelling potential allows conservative observation for mild angular malunions — the rule of thumb is that remodelling is more likely when the deformity is in the plane of joint motion, the child is younger, and residual growth is substantial.
Provided image
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
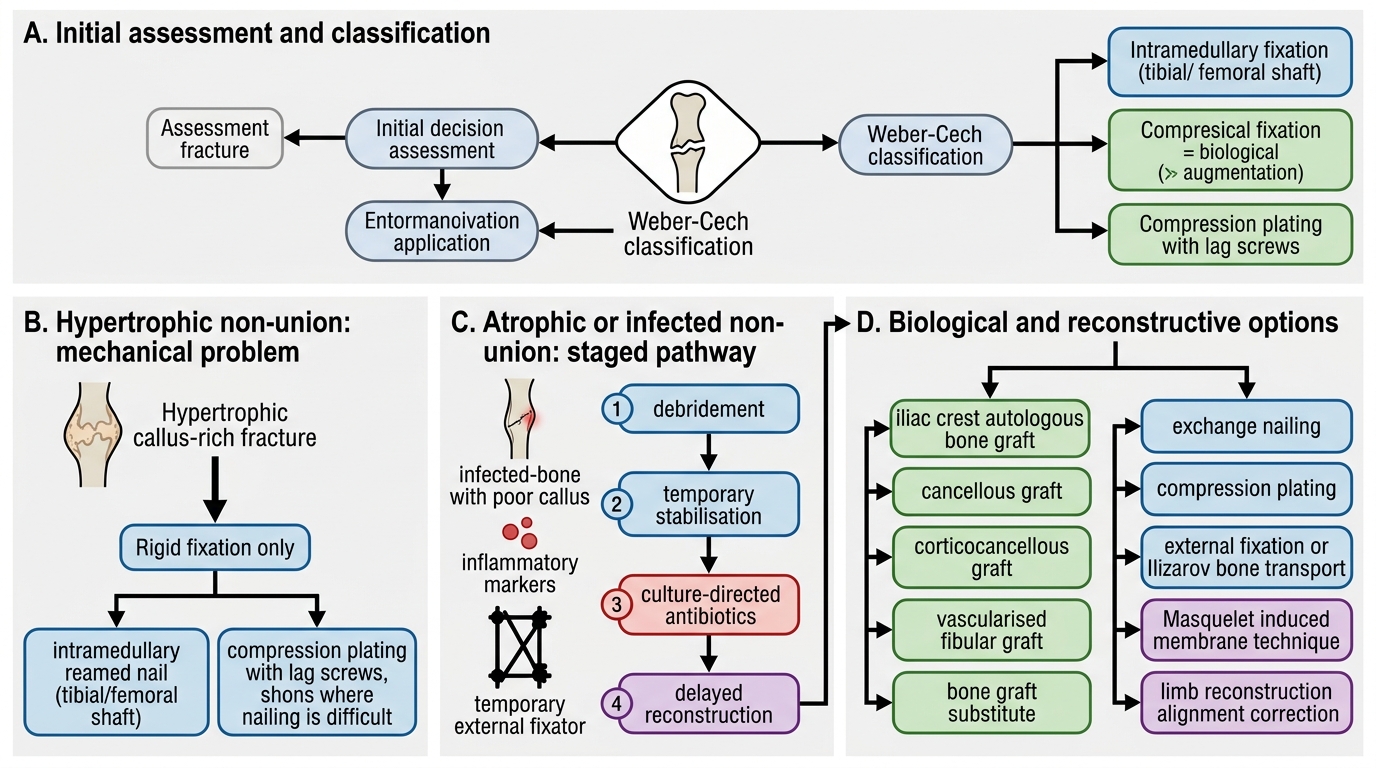
Management of Non-union
Self-Assessment: Key Concepts in Fracture Complication Investigation
This section consolidates the diagnostic framework you have built across the module. When you encounter a patient with a suspected fracture complication, your investigative approach should follow a clear logical sequence rather than ordering every available test. Begin with the clinical history and plain radiograph to determine the complication type; this alone dictates the next steps. For malunion, plain radiographs (long-leg standing views) combined with CT scanogram define the deformity precisely enough to plan corrective osteotomy. For non-union, the Weber-Cech classification derived from radiograph callus pattern determines whether bone graft is needed: hypertrophic non-union needs rigidity (no graft); atrophic non-union needs both rigidity and graft; infected non-union needs debridement before anything else. For suspected infected non-union, order ESR and CRP as inflammatory screen, but plan intraoperative deep bone biopsy (minimum 5 specimens, separate containers, prolonged culture) as the definitive diagnostic step -- do not rely on sinus-tract swabs. MRI is the imaging of choice when infection is suspected early or when metalwork artefact on CT limits interpretation.
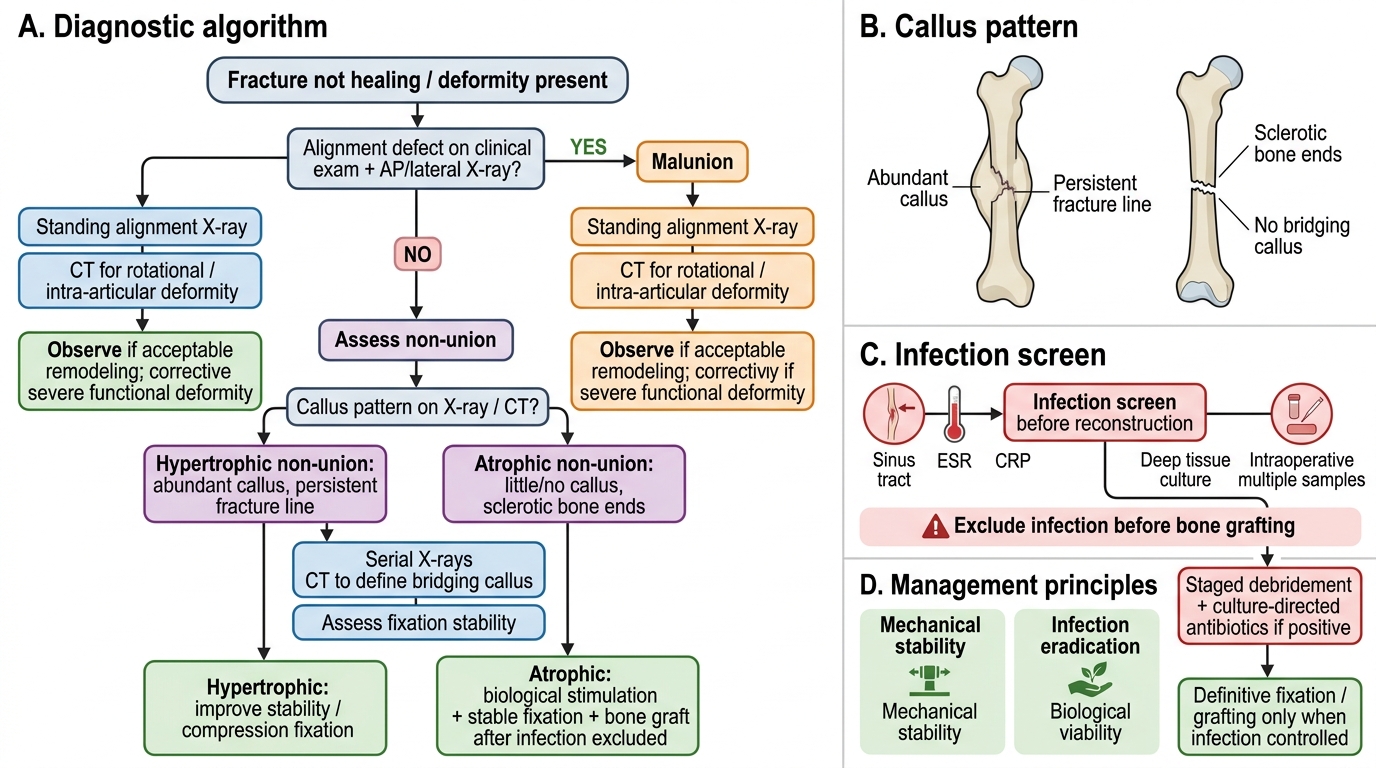
Fracture Complication Investigation Algorithm
Test your understanding with these self-check questions: (1) A tibial fracture at 7 months shows abundant callus but persistent fracture line. CRP is normal. What is the Weber-Cech type, what investigation confirms the callus pattern detail, and what is the treatment? (2) A femoral non-union has no callus, sclerotic bone ends, ESR 85 mm/h, CRP 42 mg/L, and a discharging sinus. What is the priority before bone grafting, and what specific investigation must be performed intraoperatively? (3) A child has a Colles-type fracture of the distal radius malunited in 20 degrees of dorsal angulation at 6 months post-injury. The child is 8 years old. What factors favour conservative observation over osteotomy?
CLINICAL PEARL
The single most important clinical pearl in fracture complication investigation is: always exclude infection before planning bone-grafting surgery for non-union. A sinus tract, even one that has been present for years and appears quiescent, mandates deep tissue culture before any reconstructive procedure. CRP and ESR should be obtained at baseline and the patient counselled that if cultures are positive, the reconstruction will be staged — debridement and stabilisation first, bone grafting only after the infection is controlled. Proceeding to bone grafting in the presence of occult infection predictably results in graft failure and a far more complex defect than was present originally.