Page 5 of 17
OR2.15 | Open Fracture Infection Prevention — SDL Guide
Learning Objectives
- Classify open fractures using the Gustilo-Anderson system (I, II, IIIA, IIIB, IIIC) and identify the key features of each grade, especially that grade IIIC denotes arterial injury requiring repair
- Describe the mechanism of injury and clinical features of open fractures with attention to soft-tissue contamination and devitalisation
- Justify the administration of antibiotics within 1 hour of presentation and tetanus prophylaxis as the immediate non-surgical priorities
- Explain that debridement should be performed early-as-feasible (the old fixed 6-hour rule is now obsolete) and describe the principles of wound management
- Outline the stepwise management approach to open fractures, including skeletal stabilisation and wound-closure decisions
INSTRUCTIONS
An open fracture is a surgical emergency. The exposed bone is contaminated from the moment of injury, and the window to prevent deep infection is measured in hours. A final-year student at the emergency department must know exactly what to do in the first 60 minutes: classify the wound, give antibiotics immediately, assess the vascular status, and arrange urgent surgery. The Gustilo-Anderson classification is not just an academic exercise -- it predicts infection risk, guides antibiotic selection, and determines whether the patient needs a vascular surgeon. This module equips you to act correctly from the moment you see the patient.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch. 6 — Open Fractures (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch. 22 (textbook)
- ATLS Student Course Manual, 10th ed. — Musculoskeletal Trauma (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
An 18-year-old motorcyclist is brought to the emergency department after a road accident. His left leg is bleeding. The bone is visibly protruding through a 4 cm laceration below the knee. The foot is pale and the dorsalis pedis pulse is absent. His tetanus vaccination history is unknown. The clock on the wall reads 22:14. What do you do in the next 60 minutes, and what single decision will most determine whether he keeps his leg?
WHY THIS MATTERS
Open fractures are among the most urgent injuries in orthopaedics because the contaminated wound provides a direct route for bacteria to reach the bone. The consequences of failing to act correctly in the first hour -- missing an absent pulse, delaying antibiotics, or misclassifying the wound -- range from deep bone infection and non-union to gas gangrene and limb loss. In a country where road-traffic accidents account for a substantial burden of orthopaedic admissions, every final-year student must be able to triage, classify, and initiate management of an open fracture before the surgeon arrives.
RECALL
Recall your wound-infection knowledge: bacteria introduced at the time of injury begin adhering to devitalised tissue and implant surfaces within minutes; biofilm formation that resists antibiotic penetration is established within hours. The primary goal of early antibiotics is to suppress the initial inoculum before biofilm is established. From your anatomy training, recall the three-compartment fascial anatomy of the leg and that the anterior compartment is most susceptible to compartment syndrome. From your physiology training, recall that capillary refill time >2 seconds, absent Doppler signal, and an ankle-brachial index <0.9 all indicate compromised arterial perfusion.
Open Fracture -- Clinical Presentation and Emergency Assessment
An open fracture is defined as any fracture in which the overlying skin and soft tissues are breached, allowing the fracture haematoma to communicate with the external environment. This communication need not mean that bone is visibly protruding -- even a puncture wound of 1 cm overlying a fracture is an open fracture by definition, because the skin barrier is broken and the wound is contaminated. The history should document: the mechanism of injury (high-energy mechanisms such as road-traffic accidents, gunshots, and industrial crush injuries produce the most contaminated and devitalised wounds); the time elapsed since injury (relevant to antibiotic timing and viability assessment); the patient's tetanus immunisation status; and any pre-hospital intervention (tourniquet application, wound dressing). On clinical examination, the wound should be inspected once with a sterile dressing and NOT repeatedly re-exposed, because each re-exposure introduces additional contamination. The six cardinal features to document are: (1) wound size (length in cm); (2) degree of soft-tissue contamination (clean, moderately contaminated, heavily contaminated with soil, faecal, or aquatic material); (3) degree of soft-tissue and muscle devitalisation; (4) periosteal stripping; (5) neurovascular status of the limb distal to the fracture -- this is the most critical assessment; and (6) whether the fracture pattern is segmental, comminuted, or simple.
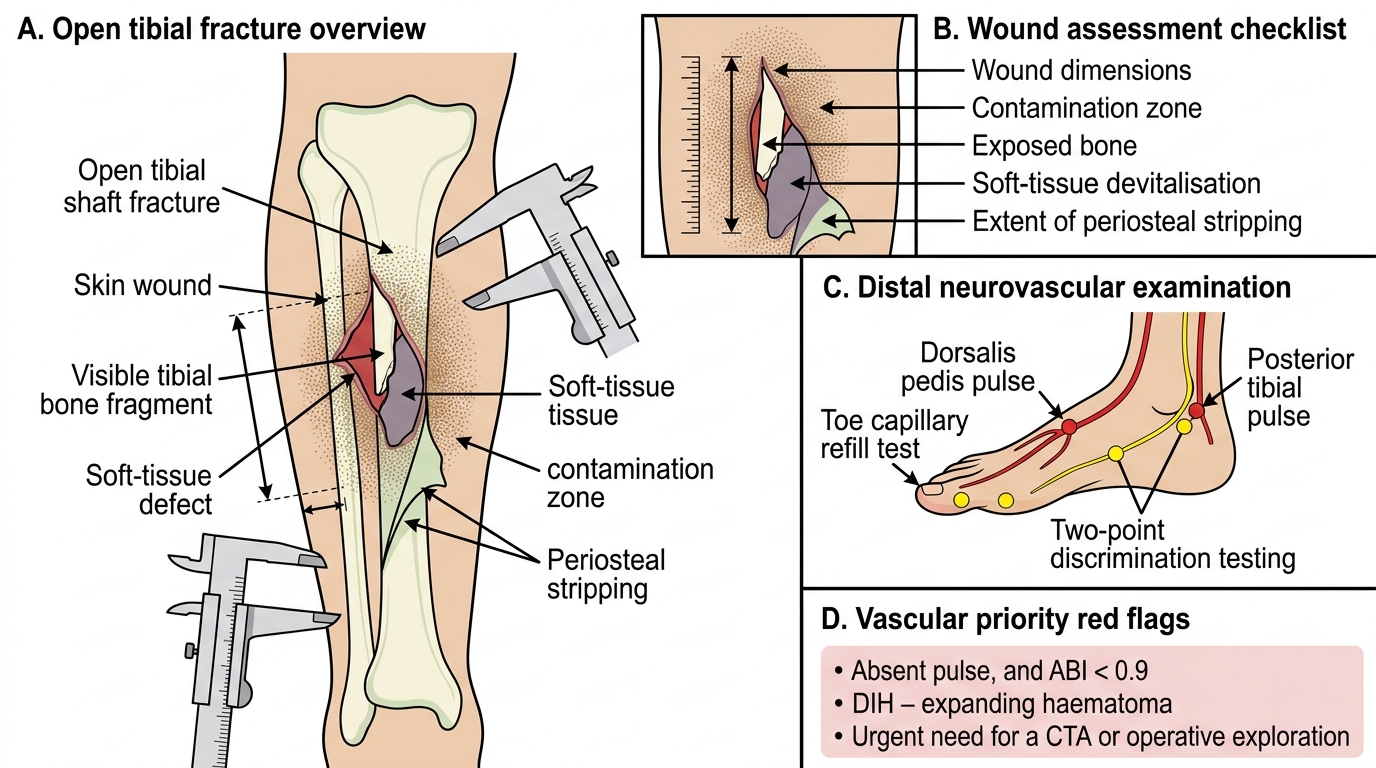
Open Tibial Fracture: Wound and Neurovascular Assessment
Vascular assessment is the highest priority because Gustilo-Anderson grade IIIC requires immediate vascular surgery involvement. The presence of a palpable distal pulse does NOT exclude a vascular injury -- an intimal tear can be present with a normal pulse initially, only to thrombose over the following hours. Any absent pulse, ankle-brachial index <0.9, or expanding haematoma mandates urgent CT angiography or direct operative exploration depending on the haemodynamic stability of the patient. A warm pink foot with normal two-point discrimination and present pulses makes significant arterial injury unlikely but does not completely exclude it in high-energy mechanisms.
Gustilo-Anderson Classification of Open Fractures
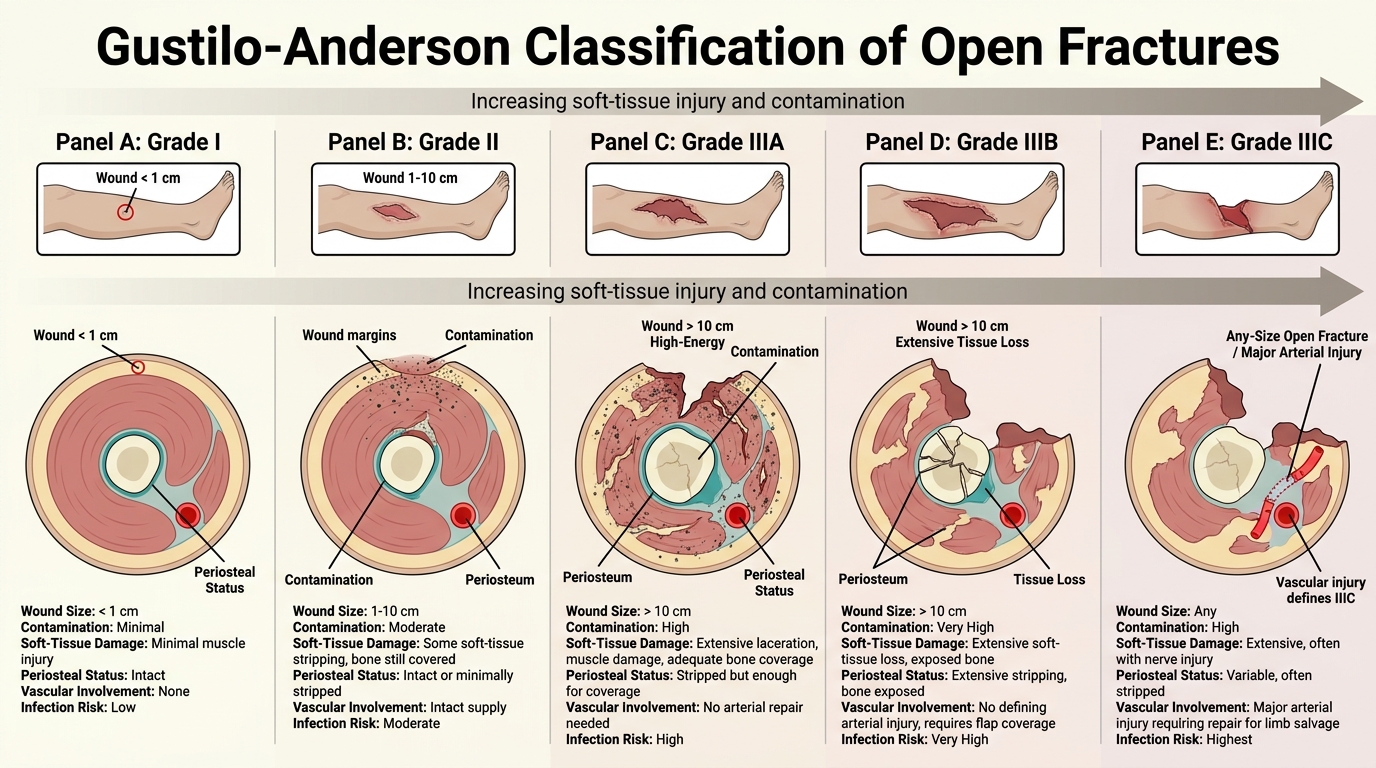
The Gustilo-Anderson classification is the universally used system for grading open fractures, originally described in 1976 and subsequently revised in 1984 to subdivide the heterogeneous Grade III category into three mechanistically distinct sub-groups. The classification is based on five clinical parameters: the wound size measured in centimetres; the degree of contamination of the wound and the surrounding tissue; the extent of soft-tissue devitalisation and periosteal stripping from the bone; the fracture pattern (simple, comminuted, or segmental bone loss); and the presence or absence of a vascular injury requiring surgical repair. Understanding this classification is not merely academic -- the grade directly drives antibiotic selection (single agent for Grade I/II; combination regimen for Grade III; antifungal/clostridial additions for specific contamination patterns), predicts the likelihood of deep infection (ranging from under 2% for Grade I to over 25% for Grade IIIC), and determines which additional surgical specialists must be involved at the time of initial debridement. Importantly, the classification should be finalised in the operating theatre after thorough debridement, not in the emergency department, because emergency wound assessment consistently underestimates the true grade -- what appears Grade II in the ED frequently proves to be Grade IIIA or IIIB once devitalised tissue has been excised and the true extent of periosteal stripping is visible.
Gustilo-Anderson Classification of Open Fractures
The classification is as follows:
- Grade I: wound <1 cm, clean, minimal soft-tissue damage, simple fracture pattern. Infection risk approximately 0-2%.
- Grade II: wound 1-10 cm, moderate contamination, some soft-tissue stripping but adequate coverage of bone, moderate comminution. Infection risk approximately 2-7%.
- Grade IIIA: wound >10 cm OR high-energy mechanism regardless of wound size; extensive soft-tissue laceration and damage; adequate soft-tissue coverage of bone despite the damage; or high-velocity gunshot wounds. Infection risk approximately 7-12%.
- Grade IIIB: extensive soft-tissue loss with periosteal stripping and bone exposure that CANNOT be covered by the local soft-tissue envelope; requires local or free flap coverage. Infection risk approximately 10-50%.
- Grade IIIC: open fracture of any wound size associated with an arterial injury requiring repair for limb salvage. The defining feature is the vascular injury, not the wound size. Amputation rates approach 25-50% even with prompt vascular repair. Infection risk approximately 25-50%.
A critical distinction: Grade IIIB and IIIC both have extensive soft-tissue damage, but the defining feature of IIIC is the arterial injury requiring repair -- without vascular reconstruction, the limb will not survive regardless of the bony or soft-tissue management. The classification should be finalised in the operating theatre after debridement, not in the emergency department, because wound appearances in the ED consistently underestimate the true grade.
SELF-CHECK
A 30-year-old pedestrian has an open femoral fracture from a bus impact. The wound is 12 cm, heavily contaminated with road grime, the quadriceps are extensively lacerated with devitalised muscle, but the femoral artery is intact and the limb is warm with normal capillary refill. What is the Gustilo-Anderson grade, and what does this grade primarily require beyond standard debridement?
A. Grade IIIA -- extensive soft-tissue damage with adequate bone coverage; standard antibiotics and stabilisation are sufficient
B. Grade IIIB -- extensive soft-tissue loss with periosteal stripping requiring flap coverage for bone
C. Grade IIIC -- arterial injury requiring vascular surgical repair
D. Grade II -- wound 1-10 cm with moderate soft-tissue damage
Reveal Answer
Answer: B. Grade IIIB -- extensive soft-tissue loss with periosteal stripping requiring flap coverage for bone
The wound is >10 cm with extensive soft-tissue laceration and devitalised muscle -- this meets the criteria for Grade III. The arterial supply is intact (not IIIC). The key question is whether bone can be covered by local soft tissue. 'Extensively lacerated quadriceps with devitalised muscle' and periosteal stripping in a high-energy mechanism suggest bone will be exposed after debridement -- this is Grade IIIB, requiring soft-tissue reconstruction (flap coverage) in addition to skeletal stabilisation. If adequate soft-tissue coverage were achievable without flap, it would be IIIA.
Investigations for Open Fractures
The investigation workup for open fractures must be completed rapidly without delaying antibiotics or surgery. The first priority is clinical assessment, not imaging. Radiological investigation begins with plain radiographs in two planes of the affected bone, including the joints above and below, to characterise the fracture pattern, level of comminution, and bone loss. In pelvic or complex injuries, CT with three-dimensional reconstruction is requested after initial clinical stabilisation. CT angiography is the investigation of choice for suspected arterial injury when the patient is haemodynamically stable -- it is faster, less invasive, and sufficiently accurate to plan vascular surgical intervention. Formal catheter angiography is reserved for cases where CT angiography is equivocal or unavailable, or where the injury is a knee dislocation (which carries a 20-30% risk of popliteal artery injury and warrants a low threshold for angiography even with a palpable pulse). Bedside ankle-brachial index (ABI) measurement using a Doppler probe is a rapid, non-invasive screen: an ABI <0.9 indicates arterial injury requiring further investigation. Compartment pressure monitoring is indicated when the clinical diagnosis of compartment syndrome is uncertain -- a compartment pressure >30 mmHg, or a differential pressure (diastolic BP minus compartment pressure, the so-called delta P) <30 mmHg, is the fasciotomy threshold. Laboratory investigations include: full blood count (baseline for surgical planning); coagulation screen (coagulopathy common in polytrauma); blood grouping and cross-matching; urea and electrolytes (renal function, especially in crush injuries at risk of rhabdomyolysis); and creatine kinase (CK) if rhabdomyolysis is suspected. Wound cultures from the emergency department are NOT useful for antibiotic guidance because the contaminating flora does not predict the infecting organisms that eventually cause late deep infection.
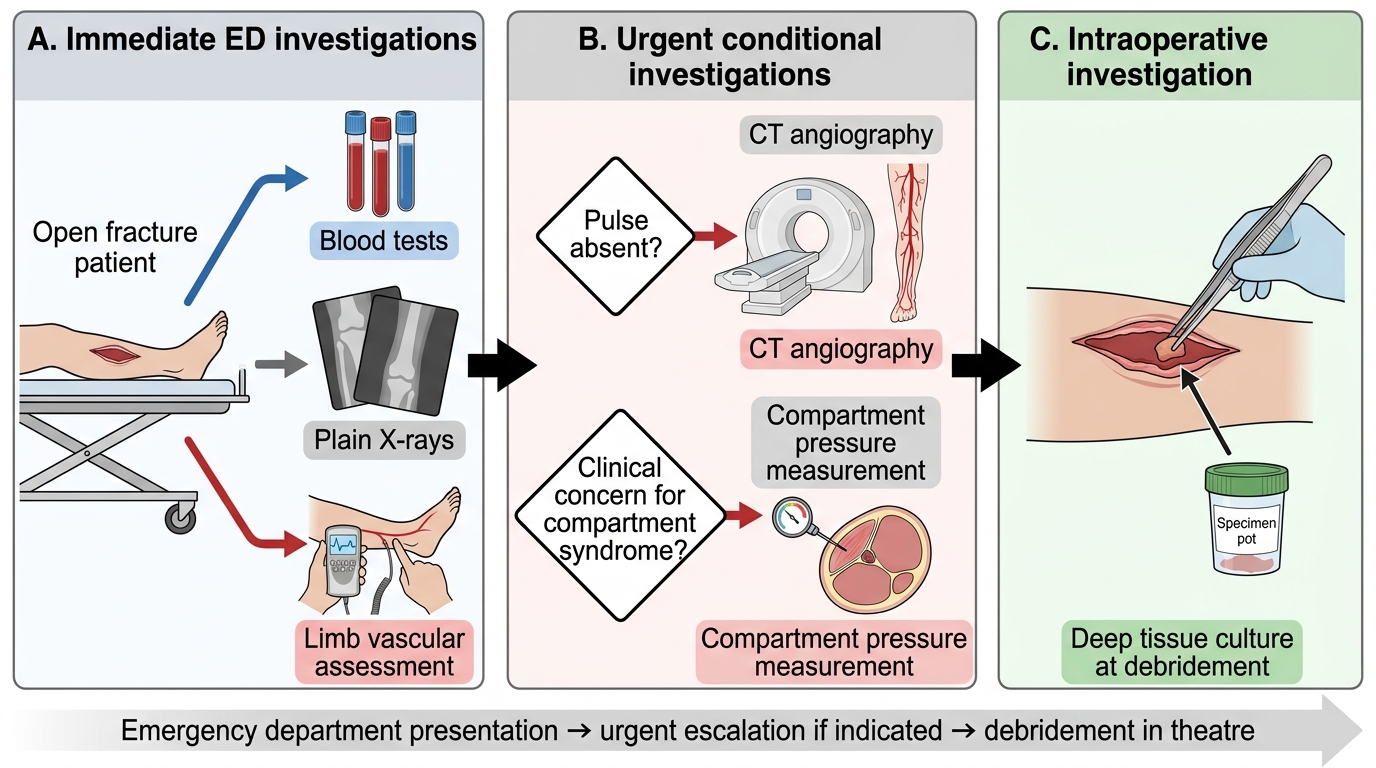
Investigation Sequence for an Open Fracture