Page 9 of 17
OR2.16 | Paediatric Orthopaedic Injury Patterns — SDL Guide (Part 2)
Supracondylar Fracture -- Management
Management is guided by the Gartland grade and neurovascular status. Gartland I: collar-and-cuff immobilisation for 3 weeks; no reduction needed. Gartland II: closed reduction under general anaesthesia followed by K-wire fixation is now standard practice even for most Grade II injuries, because maintaining reduction in a cast alone is unreliable; previously, Grade II was managed by closed reduction and casting, but K-wire fixation has substantially reduced the incidence of iatrogenic cubitus varus. Gartland III: urgent closed reduction and percutaneous K-wire fixation (two lateral wires is the preferred technique to avoid iatrogenic ulnar nerve injury from a medial wire); if closed reduction fails or neurovascular compromise persists after reduction, open reduction via an anterior approach is performed. A pink pulseless hand that fails to reperfuse after reduction requires immediate exploration of the brachial artery. The child should be admitted for overnight neurovascular observation after any Grade II or III supracondylar fracture.
SELF-CHECK
A 7-year-old girl with a Grade III supracondylar humerus fracture has a pink, warm hand with absent radial pulse after closed reduction and K-wire fixation under general anaesthesia. What is the correct next step?
A. Apply a well-padded backslab and observe for 24 hours -- the pulse usually returns spontaneously
B. Perform urgent CT angiography to confirm arterial injury before any further intervention
C. Immediate operative exploration of the brachial artery through an anterior elbow approach
D. Administer intravenous heparin and observe for reperfusion
Reveal Answer
Answer: C. Immediate operative exploration of the brachial artery through an anterior elbow approach
A pink pulseless hand that fails to reperfuse after adequate closed reduction of a supracondylar fracture requires immediate operative exploration of the brachial artery. The pink colour indicates collateral flow is adequate -- the hand is viable -- but the absent pulse indicates the main artery is compromised (kinked, spasmodic, or lacerated). In the paediatric elbow, urgent exploration and repair (or release of vascular spasm) is performed. CT angiography adds time without changing management -- if the pulse is absent after reduction the decision to explore is clinical. Observation risks propagating thrombosis and ischaemic muscle necrosis.
Forearm Fractures and Pulled Elbow in Children
Provided image
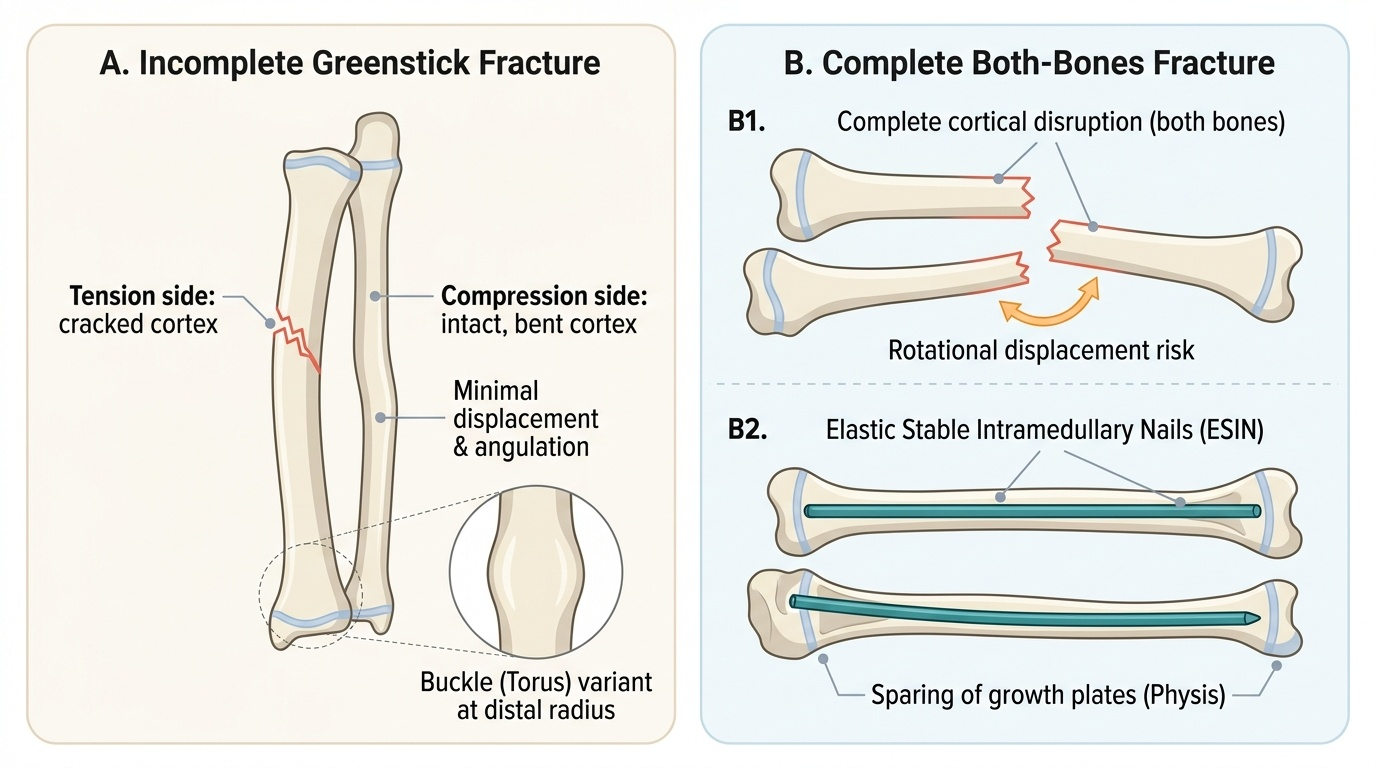
Forearm fractures in children have distinct patterns not seen in adults because of the relative flexibility of immature cortical bone and the remodelling potential of the growing skeleton. The three most important paediatric forearm injury patterns are: greenstick fractures, complete forearm shaft fractures, and pulled elbow (radial head subluxation). Understanding each requires knowledge of the biological basis of paediatric bone.
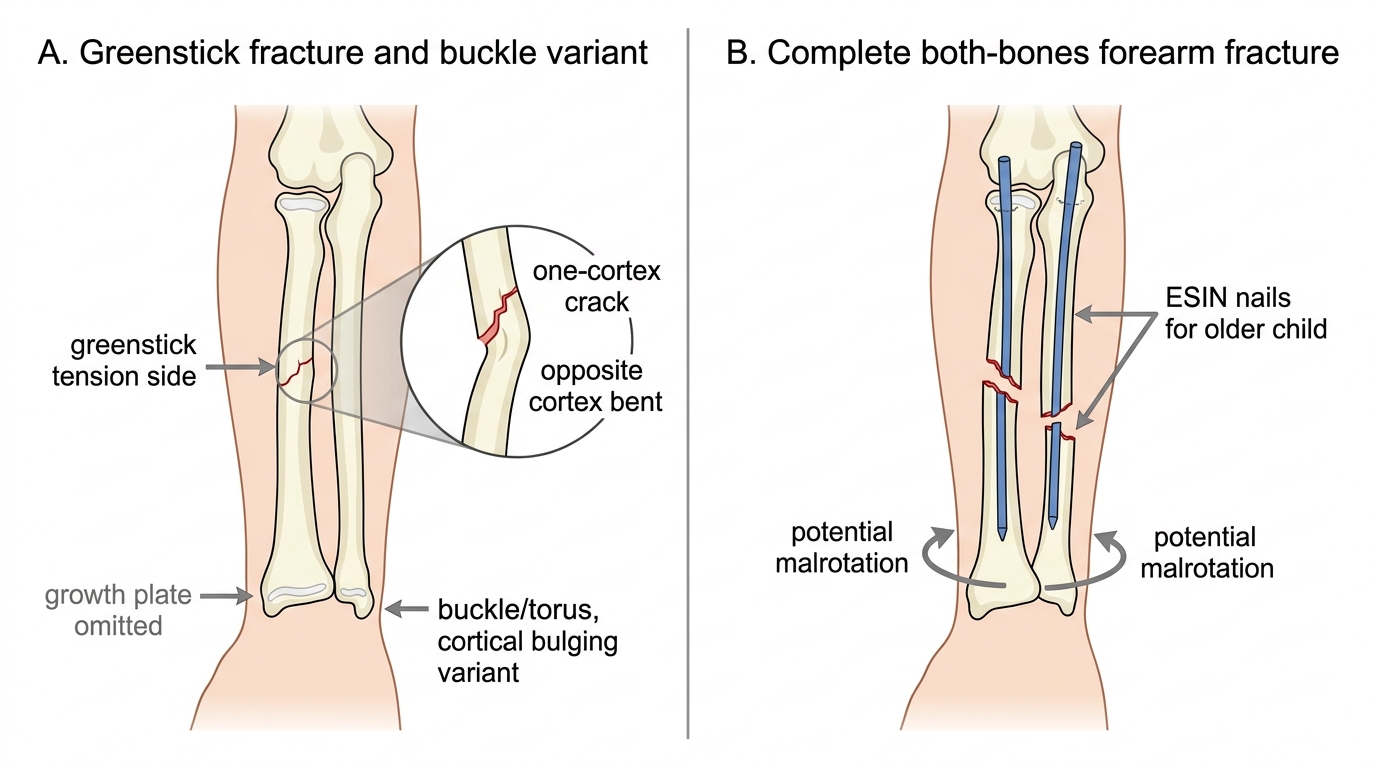
A greenstick fracture occurs because immature bone is more plastic and less brittle than adult bone -- when a bending force is applied, the tension side of the bone cracks (producing an incomplete fracture line) while the compression side bends without breaking. Clinically, there is localised tenderness, mild swelling, and pain on loading of the forearm, but the limb is not grossly deformed because the bone is partially intact. Radiologically, the fracture line is visible on one cortex only with opposite cortex intact but bent. Treatment is closed reduction (straightening of the deformity) and plaster immobilisation; importantly, the intact cortex must be broken (completing the fracture) during reduction so that the fracture can be fully corrected -- an incompletely corrected greenstick fracture reangulates in plaster because the intact elastic cortex springs back.
Complete both-bones forearm fractures (radius and ulna) in children are managed by closed reduction and plaster for ages under 10, where remodelling potential is high. The acceptable degree of residual angulation is age-dependent: up to 10-15 degrees angulation is acceptable under age 10 but essentially zero under 6. In children over 10, elastic intramedullary nailing (ESIN, e.g. Nancy nails) achieves stable fixation without sacrificing the ability to close the growth plate. A key anatomical feature of children's forearm fractures is the potential for anterior interosseous nerve (AIN) injury -- the nerve runs in the interosseous space and can be trapped in fractures of the proximal third of the radius. Always assess the 'OK sign' in children with forearm fractures.
Greenstick vs Complete Both-Bones Forearm Fracture in a Child
Pulled Elbow (Radial Head Subluxation)
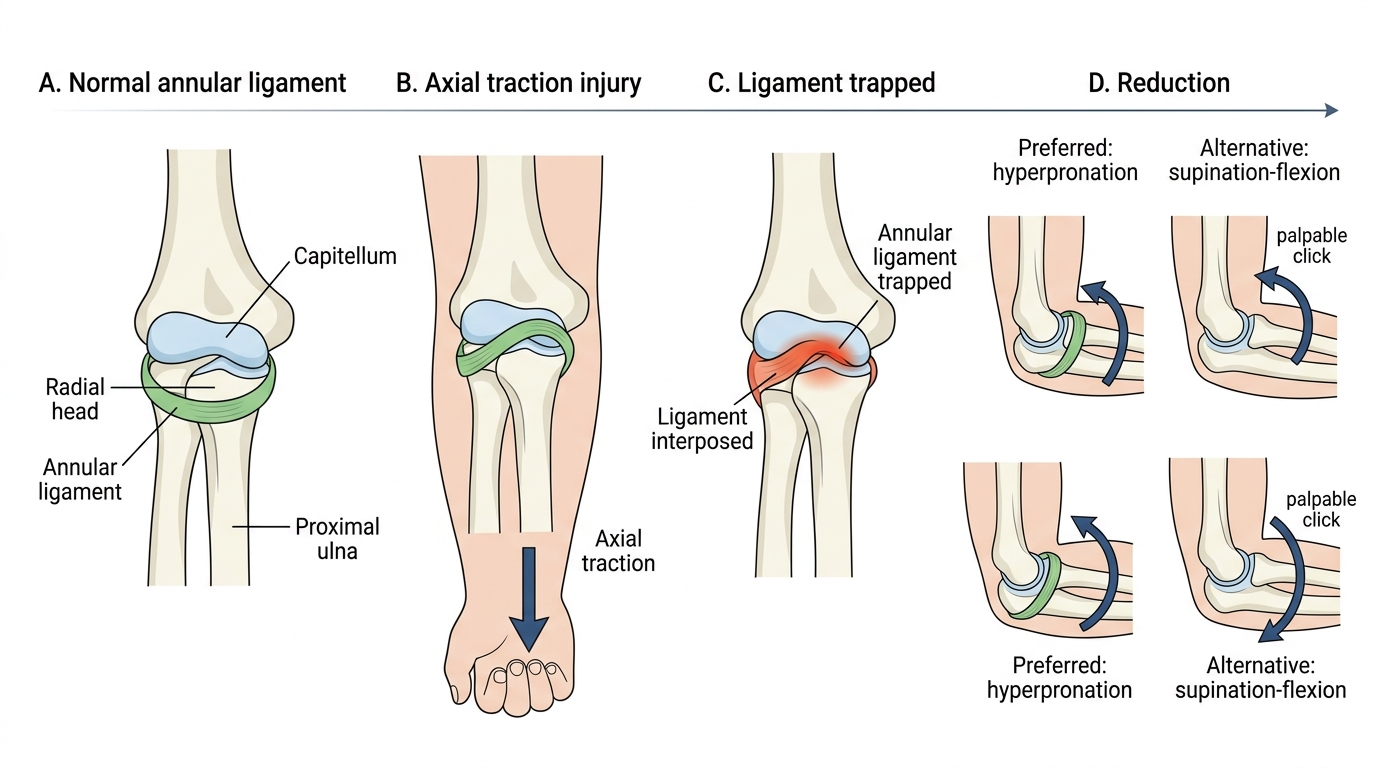
Pulled elbow (also called nursemaid's elbow or radial head subluxation) is a specific injury unique to young children, most commonly occurring between 1 and 5 years of age, caused by a sudden axial traction force on the extended, pronated forearm -- classically when an adult lifts a child by the hand or swings a young child by the arms. The mechanism causes the annular ligament (which encircles the radial head to hold it in the proximal radioulnar joint) to slip over the radial head and become trapped between the radial head and the capitellum. This is a soft-tissue injury, not a fracture -- the radial head is not displaced from the elbow joint itself, but the annular ligament is interposed and prevents normal radial head rotation. The clinical presentation is characteristic: the child holds the arm in mild elbow flexion with the forearm in pronation, refuses to use the arm, and cries when any attempt is made to supinate the forearm or flex the elbow. There is minimal swelling and no point bony tenderness. The history of a traction mechanism in a child of the right age, combined with the clinical picture, is sufficient to make the diagnosis -- radiographs are typically normal and need not be taken if the history and examination are classic. If taken, plain radiographs show no bony abnormality (differentiating from a lateral condyle fracture, which is the main differential and does show radiological changes).
Pulled Elbow: Mechanism and Reduction
Reduction is performed by two methods, both performed without anaesthesia as an outpatient. The hyperpronation method (now preferred for higher first-attempt success rate approximately 90%) involves firm hyperpronation of the forearm with the elbow held at 90 degrees. The supination-flexion method (classic technique) involves supinating the forearm while simultaneously flexing the elbow -- a palpable click felt over the radial head confirms reduction. After successful reduction, the child typically begins using the arm within 10-15 minutes. No immobilisation is required. Parents should be counselled to avoid axial traction mechanisms in the future, as recurrence is common (up to 25-30% of cases recur with subsequent traction episodes until the annular ligament matures, typically by age 6).