Page 9 of 22
OR2.13 | Ankle Fracture Management — SDL Guide
Learning Objectives
- Describe the anatomy of the ankle mortise and the role of the medial, lateral, and posterior malleoli and the syndesmosis in ankle stability
- Apply the Weber (AO/Danis) and Lauge-Hansen classifications to ankle fractures and explain the clinical relevance of each
- Use the Ottawa Ankle Rules to clinically determine when radiographs are indicated after ankle injury
- Differentiate stable from unstable ankle fractures and outline the management principles for each
- Describe the anatomy, diagnosis, and management of syndesmotic injuries in the context of ankle fractures
INSTRUCTIONS
Ankle fractures are the most common fractures managed by orthopaedic surgeons, and ankle sprains are the most common acute musculoskeletal injury seen in any emergency department. The clinical challenge is to identify, from the large number of patients who present with a 'twisted ankle', the subset who have a fracture or unstable injury requiring operative intervention, without subjecting the majority to unnecessary radiation. The Ottawa Ankle Rules, the Weber and Lauge-Hansen classifications, and the concept of ankle mortise stability are the intellectual tools that organise this decision-making. Mastery of these frameworks equips every MBBS graduate to manage ankle injuries confidently at the initial clinical contact.
References
- Maheshwari's Essential Orthopaedics, Ch 31 (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 31 (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old netball player inverts her ankle while landing. She comes to casualty with lateral ankle pain and swelling. She can partially weight-bear. On examination, there is tenderness over the tip of the lateral malleolus and the anterior talofibular ligament, but no tenderness over the medial malleolus, the navicular, or the base of the fifth metatarsal. Should you order an X-ray? What clinical rule guides your decision, and what specific bony tenderness points are its triggers? Now imagine that the X-ray shows a small avulsion at the tip of the fibula below the level of the syndesmosis — does this fracture require operative fixation?
WHY THIS MATTERS
Ankle fractures represent the most common fractures treated operatively by orthopaedic surgeons, and ankle sprains are probably the most common acute soft tissue injury seen in any clinical setting globally. The distinction between a sprain, a stable fracture, and an unstable fracture-dislocation requires understanding three linked concepts: the anatomy of the ankle mortise; the Ottawa Ankle Rules, which prevent unnecessary radiographs; and the fracture classifications (Weber and Lauge-Hansen), which predict stability and guide management. Getting these right prevents two common errors: over-treating benign fibular avulsions with unnecessary surgery, and under-treating unstable fractures by sending patients home in a plaster without appreciation for the medial-side or syndesmotic injury.
RECALL
The ankle joint (tibiotalar joint) is a mortise-and-tenon hinge joint. The mortise is formed by the medial malleolus (medial pillar, tibial), the tibial plafond (roof), and the fibula in the fibular notch (lateral pillar); the talus is the tenon. The stability of the mortise depends on bony congruence AND soft tissue constraints: the deltoid ligament complex (medial: deep and superficial layers) resists lateral talar shift; the lateral collateral ligament complex (anterior talofibular ligament — ATFL; calcaneofibular ligament — CFL; posterior talofibular ligament — PTFL) resists inversion/internal rotation; the syndesmosis (the distal tibiofibular joint, held by anterior and posterior inferior tibiofibular ligaments, the interosseous membrane, and the inferior transverse ligament) maintains the mortise width. Any fracture classification that does not account for the syndesmotic and deltoid ligament status misrepresents the true injury complexity.
Ottawa Ankle Rules — Evidence-Based Triage
The Ottawa Ankle Rules (OAR), developed and validated by Stiell et al. in Ottawa in 1992, are an evidence-based clinical decision tool that specifies exactly when plain radiographs are required after ankle or foot injury — a question that arises in virtually every emergency department encounter. They were derived from a prospective cohort study designed to reduce the high rate of unnecessary ankle X-rays (which in the pre-OAR era were performed for 60–100% of ankle injury presentations, of which only approximately 15% had any fracture) while maintaining 100% sensitivity for clinically significant fractures. The rules have been validated across multiple international populations, age groups, and emergency settings, and are the global standard of care for ankle injury triage.
An ankle X-ray is required ONLY if there is pain in the malleolar zone AND at least one of the following:
1. Bone tenderness at the posterior edge or tip of the lateral malleolus (distal 6 cm of fibula)
2. Bone tenderness at the posterior edge or tip of the medial malleolus (distal 6 cm of tibia)
3. Inability to weight-bear both immediately after injury and in the emergency department (defined as taking 4 steps, even if limping)
A foot X-ray is required ONLY if there is pain in the midfoot zone AND at least one of the following:
1. Bone tenderness at the base of the fifth metatarsal
2. Bone tenderness at the navicular (medial midfoot, proximal)
3. Inability to weight-bear (same criterion)
The OAR do NOT apply to children under 18 years (physeal injuries are more common), patients with diminished sensation (diabetes, neuropathy), or patients who are intoxicated or uncooperative with the examination. Sensitivity approaches 100% for clinically significant fractures; applying the OAR saves approximately 30–40% of ankle X-rays in emergency settings.
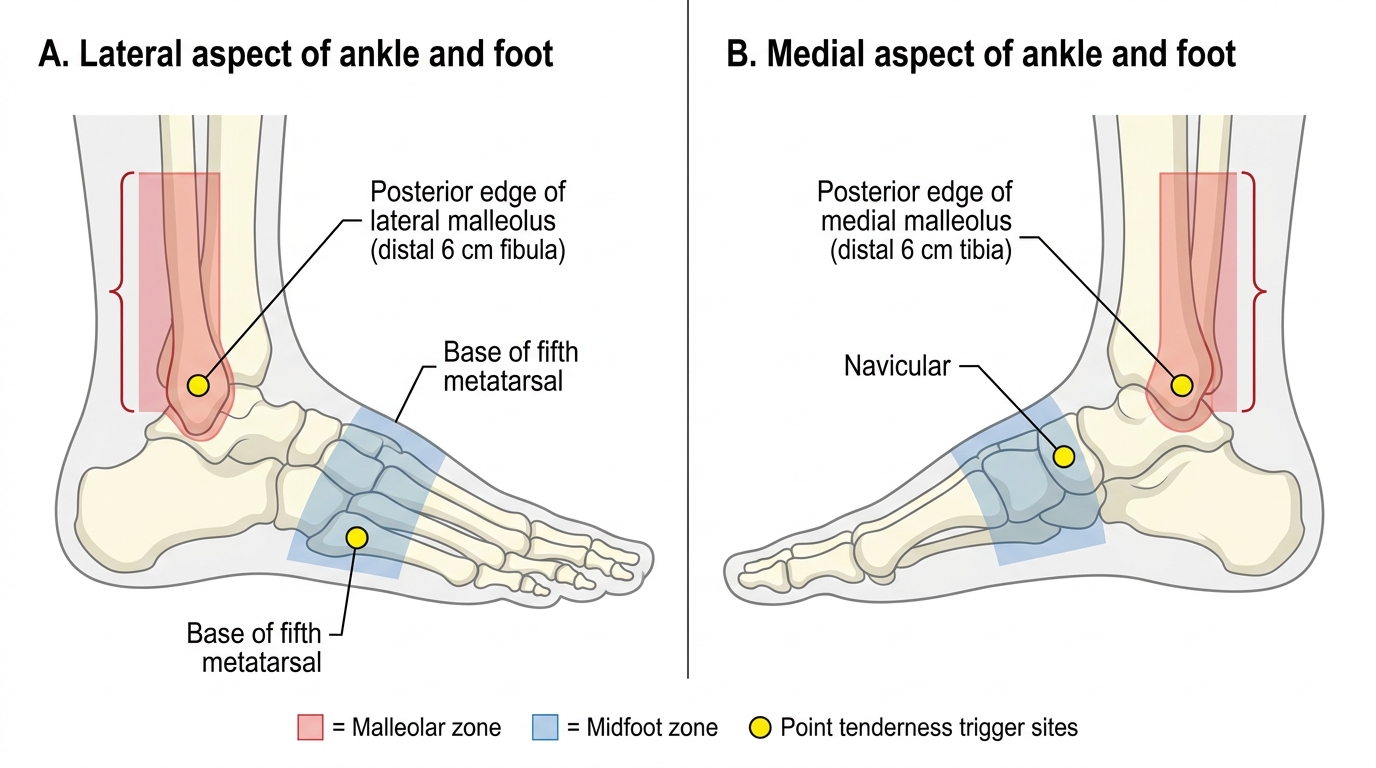
Ottawa Ankle Rule Trigger Zones
Weber (AO/Danis) Classification — Fibular Fracture Level
The Weber (AO/Danis) classification classifies ankle fractures based on the level of the fibular fracture relative to the syndesmosis. It is simple, universally understood, and has direct management implications because the fibular fracture level predicts the likelihood of syndesmotic injury and medial-sided involvement. The classification was developed by Danis and popularised by Weber, and remains the most widely used system in clinical practice.
Weber A: Fibular fracture below the level of the syndesmosis (infrasyndesmotic). The syndesmosis is intact; the medial side is rarely injured. These are typically caused by supination-adduction injuries and are inherently stable. Management is almost always non-operative (below-knee cast or walking boot for 4–6 weeks).
Weber B: Fibular fracture at the level of the syndesmosis (transsyndesmotic). The syndesmosis may or may not be disrupted — the critical question is whether the medial side (deltoid ligament or medial malleolus) is injured. If the medial side is intact, the fracture is stable and can be managed non-operatively; if the medial side is disrupted, the mortise is unstable and requires operative fixation. Weber B is the most common type and the most clinically nuanced.
Weber C: Fibular fracture above the level of the syndesmosis (suprasyndesmotic). The interosseous membrane and syndesmotic ligaments are partially or completely disrupted up to the level of the fibular fracture. The medial side is almost always injured (medial malleolus fracture or deltoid ligament rupture). These fractures are unstable and require operative fixation. The extreme of Weber C is the Maisonneuve fracture — a spiral fracture of the proximal fibula, often without any visible fracture on ankle radiographs, associated with complete syndesmotic disruption and medial-side injury; it is diagnosed only if the full fibula (including the knee) is radiographed when ankle instability is found without a visible fracture on standard ankle views.
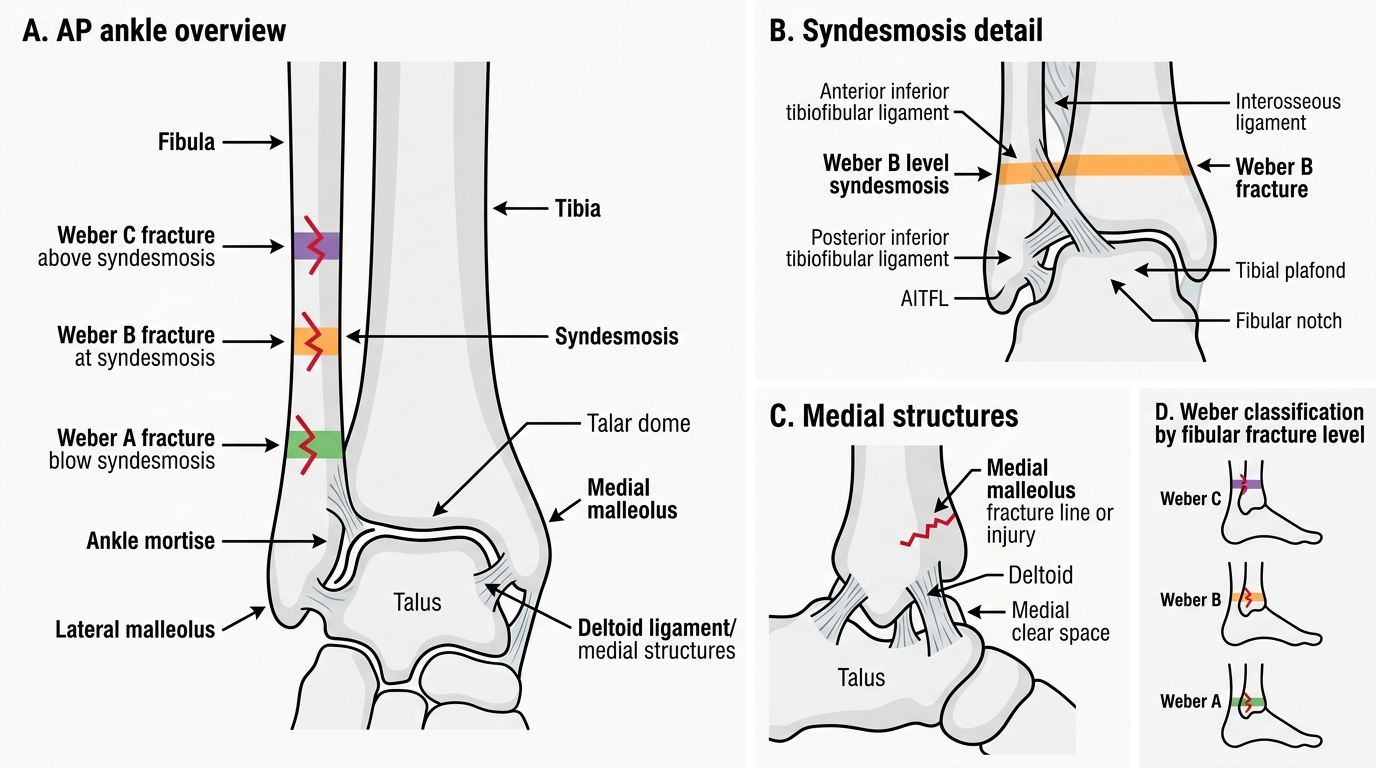
Weber Classification of Ankle Fractures
Lauge-Hansen Classification — Mechanism-Based Injury Stages
The Lauge-Hansen classification is based on the cadaveric experimental work of Niels Lauge-Hansen, who simulated ankle fractures by applying defined deforming forces to cadaveric ankles. Each pattern is described by two words: the first describes the foot position at the time of injury (supination or pronation); the second describes the direction of the deforming force (adduction, external rotation, or abduction). The classification predicts the sequential injury pattern — each stage builds on the previous — and thus tells you exactly which ligamentous and bony structures are injured in a given pattern.
The four main patterns:
1. Supination-Adduction (SAD): Stage I = lateral collateral ligament rupture (or lateral malleolus avulsion below the level of the joint); Stage II = vertical medial malleolus fracture. This corresponds to Weber A.
2. Supination-External Rotation (SER) — the most common pattern (60–70% of ankle fractures): Stage I = anterior inferior tibiofibular ligament (AITFL) rupture; Stage II = spiral/oblique fibular fracture at the level of the syndesmosis; Stage III = posterior malleolus fracture or posterior inferior tibiofibular ligament (PITFL) rupture; Stage IV = medial malleolus fracture or deltoid ligament rupture. Stages I–III = Weber B stable; Stage IV = Weber B unstable.
3. Pronation-Abduction (PAB): Stage I = medial malleolus fracture or deltoid ligament rupture; Stage II = syndesmotic disruption; Stage III = high fibular fracture with comminution. This corresponds to Weber C.
4. Pronation-External Rotation (PER): Stage I = medial malleolus fracture or deltoid rupture; Stage II = AITFL rupture; Stage III = interosseous membrane tear to the level of the fibular fracture; Stage IV = high spiral fibular fracture. Maisonneuve fracture = PER Stage IV.
The practical value of the Lauge-Hansen system: it tells you to look for associated injuries you might otherwise miss. In an SER Stage IV injury, if you see only a Weber B fibular fracture but the medial side seems intact, the medial malleolus may be intact but the deltoid ligament may still be ruptured — which is equally destabilising. A stress radiograph (manual external rotation view) or MRI can confirm medial-side disruption.
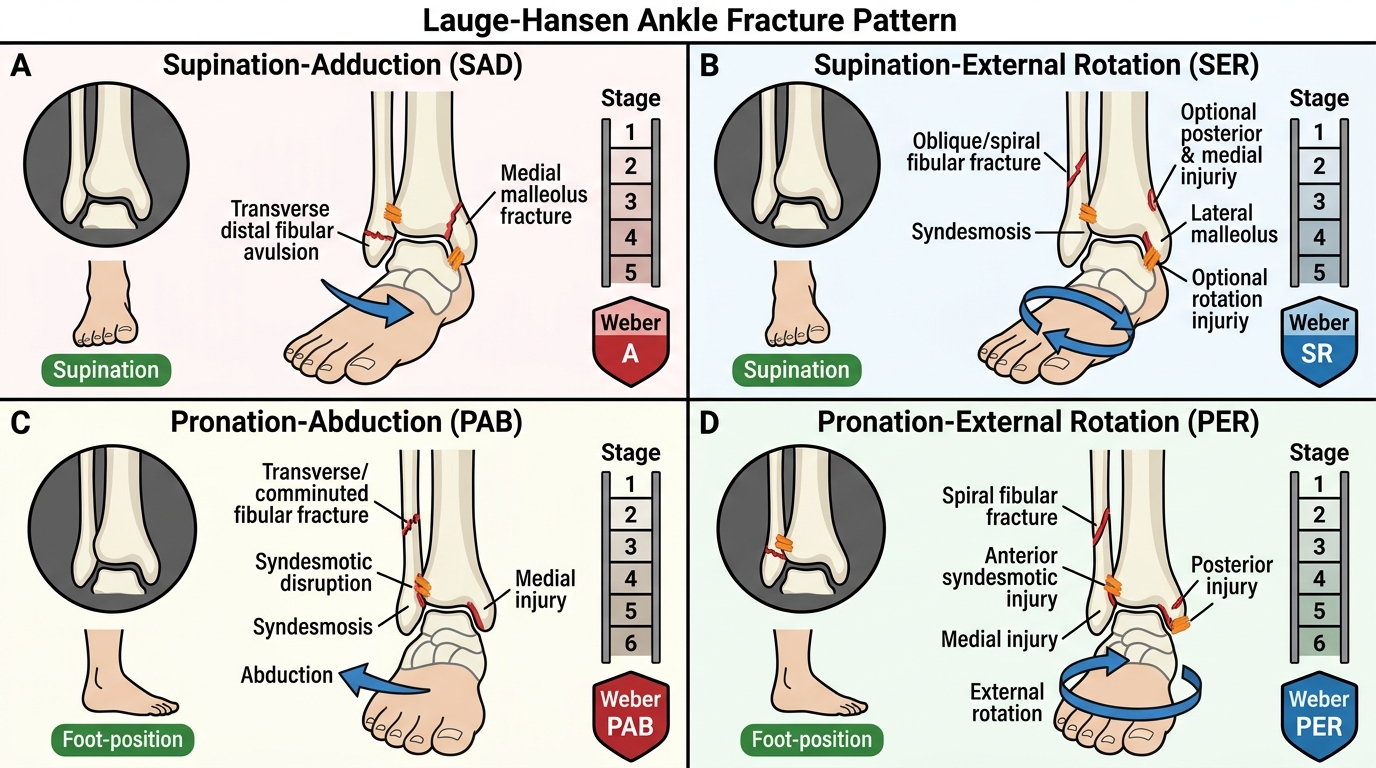
Lauge-Hansen Classification of Ankle Fractures
SELF-CHECK
A 34-year-old woman twists her ankle in external rotation. Radiographs show a spiral fibular fracture at the level of the syndesmosis and a medial malleolus fracture. According to the Lauge-Hansen classification, what pattern is this, and what is its management implication?
A. Supination-Adduction Stage II; non-operative management in cast
B. Supination-External Rotation Stage IV; operative fixation required
C. Pronation-Abduction Stage III; non-operative management in cast
D. Supination-External Rotation Stage II; non-operative management acceptable
Reveal Answer
Answer: B. Supination-External Rotation Stage IV; operative fixation required
A spiral fibular fracture at the syndesmosis level (Weber B) plus a medial malleolus fracture (medial-side injury) is a Supination-External Rotation (SER) Stage IV pattern — a bimalleolar fracture. The medial malleolus fracture makes the mortise unstable (the mortise is held by both medial and lateral pillars; when both are disrupted, the talus can shift). SER Stage IV is an unstable fracture requiring operative fixation with fibular plating and medial malleolus screw fixation.