Page 6 of 22
OR2.12 | Leg and Foot Fracture Management — SDL Guide (Part 2)
Calcaneus Fracture Management and Associated Injuries
Provided image
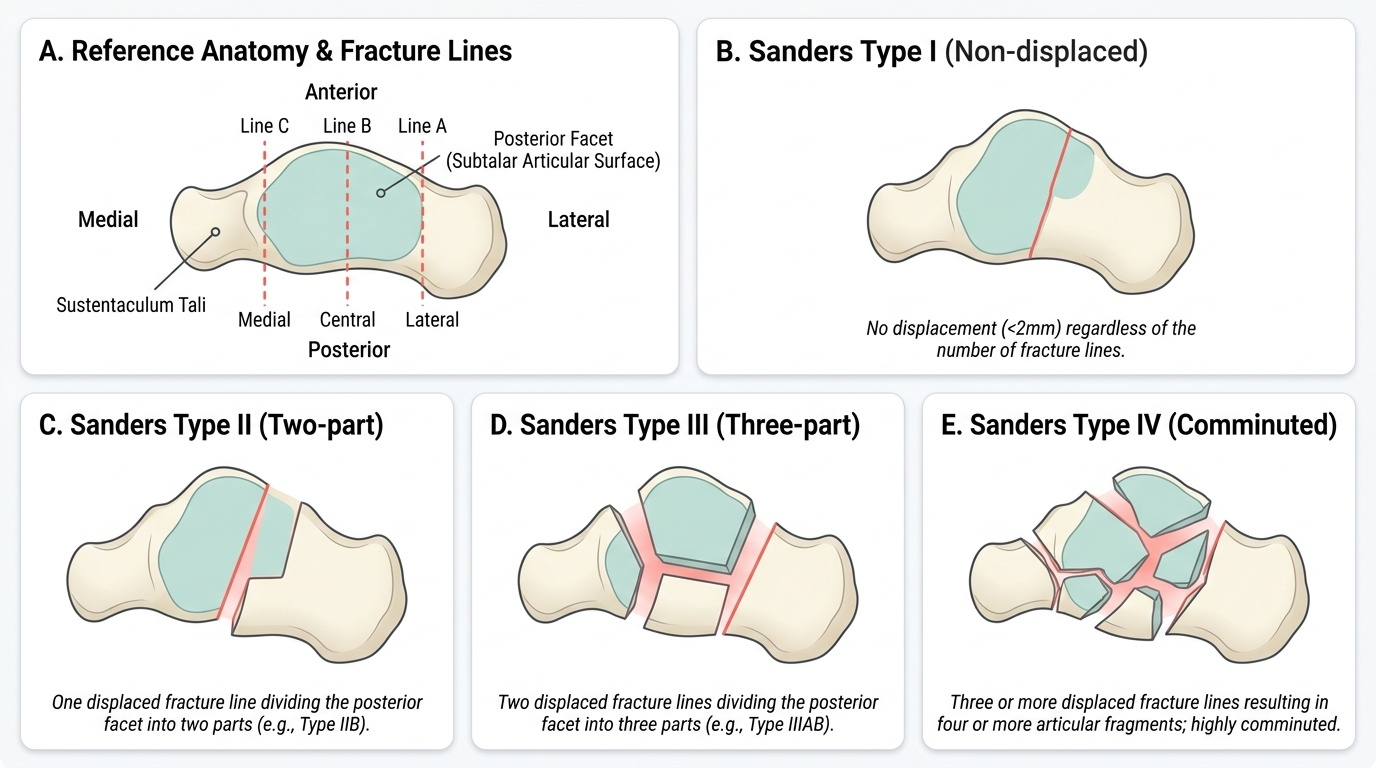
Non-operative management (below-knee cast, non-weight-bearing for 8–12 weeks) is appropriate for non-displaced fractures (Sanders Type I) and for patients who are poor surgical candidates (elderly, diabetic with peripheral vascular disease, heavy smokers). However, for displaced intra-articular fractures in young active patients, non-operative management leads to subtalar arthritis, widened heel, peroneal tendon impingement, and a shortened Achilles lever arm — all contributing to long-term pain and disability.
Operative management via open reduction and internal fixation (ORIF) through an extensile lateral approach is the standard for displaced Sanders Type II and III fractures in suitable patients. The goals are restoration of Bohler's angle, anatomic reduction of the posterior facet, correction of heel height, width, and varus/valgus alignment, and fixation with a low-profile calcaneal locking plate. Primary subtalar arthrodesis is preferred for Type IV fractures or extensively comminuted injuries where articular reconstruction is not feasible. Timing of surgery is critical: waiting 10–14 days for soft tissue swelling to subside (the 'wrinkle test' — skin wrinkles when pinched = swelling resolved) is standard practice because the extensile lateral approach carries a high wound-complication rate if performed through oedematous tissue.
Associated injuries in falls from height are well-established and must be actively sought: bilateral calcaneus fractures occur in 10–15% of cases (always X-ray both heels); compression fractures of the lumbar spine (L1–L2 most common) are present in approximately 10% of high-energy calcaneus fractures (the so-called 'Don Juan' injury pattern — lumbar spine radiography is mandatory); tibial plateau fractures may also occur in the same fall mechanism.
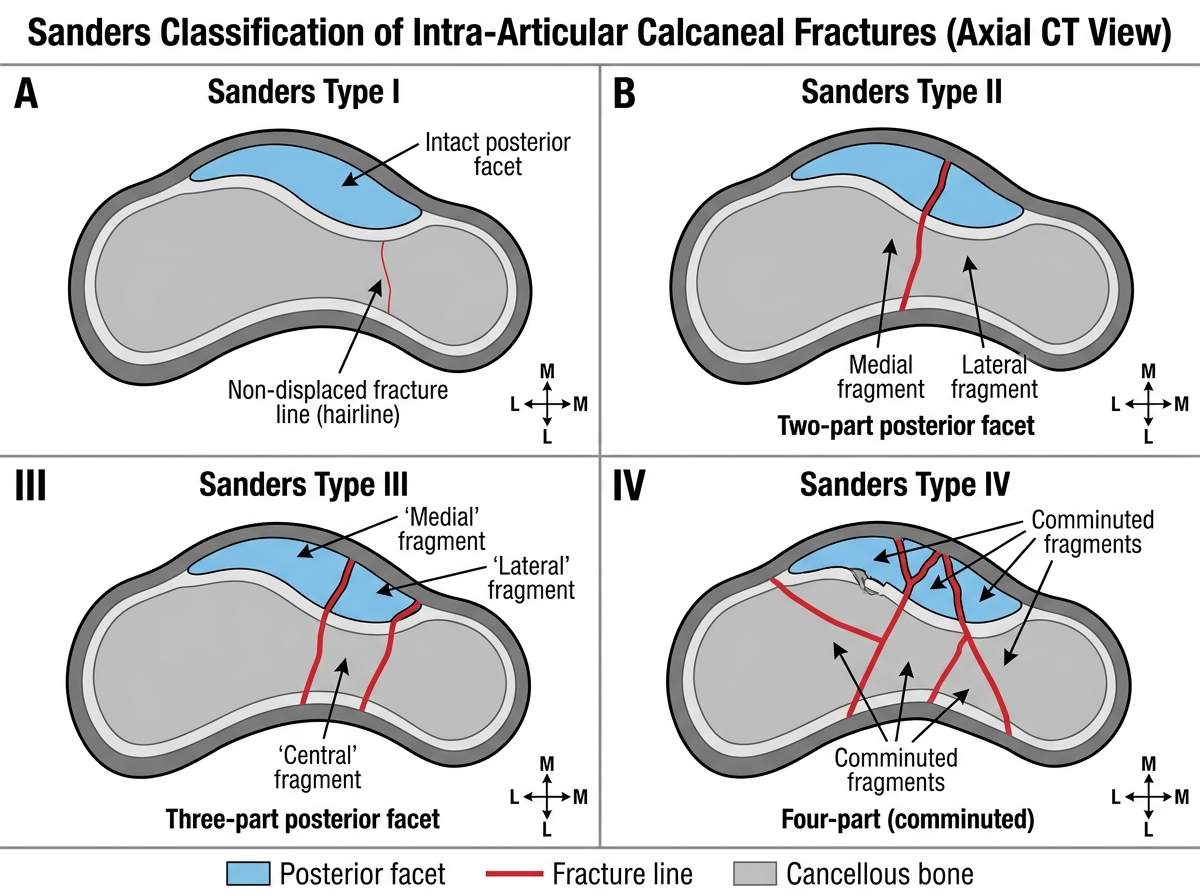
Sanders Classification of Intra-Articular Calcaneal Fractures (Axial CT)
Small Bones of the Foot — Metatarsals and Phalanges
Metatarsal fractures are among the most common foot injuries and range from the nearly trivial (stress fractures of the 2nd metatarsal neck in a marathon runner) to the potentially limb-threatening (Lisfranc complex fracture-dislocation). The fifth metatarsal deserves special attention because it has two distinct fracture zones with different management implications: the avulsion fracture at the base (tip of the styloid process, pulled off by the peroneus brevis tendon — commonly called a 'pseudo-Jones fracture'), which is benign and managed with a firm shoe or boot for 4–6 weeks; and the Jones fracture, a transverse fracture at the metaphyseal-diaphyseal junction of the fifth metatarsal (approximately 1.5–2 cm distal to the base), which occurs in the zone of the 'watershed area' with poor blood supply and carries a high risk of non-union — operative fixation with an intramedullary screw is required in athletes and active patients. These two fractures are frequently confused and must be distinguished on radiograph.
Stress fractures of the metatarsals (March fractures, most common in the 2nd and 3rd shafts) present with insidious onset pain, localised tenderness, and swelling after an increase in activity; plain radiographs may be normal in the first 2 weeks, after which periosteal reaction appears. Management is activity modification and protected weight-bearing.
Phalangeal fractures are common minor injuries from stubbing or direct trauma. The great toe (hallux) phalanx fractures are more significant because of the hallux's role in toe-off during gait; displaced intra-articular fractures of the proximal phalanx may need ORIF. Lesser toe phalangeal fractures are treated symptomatically with buddy taping to the adjacent toe for 3–4 weeks.
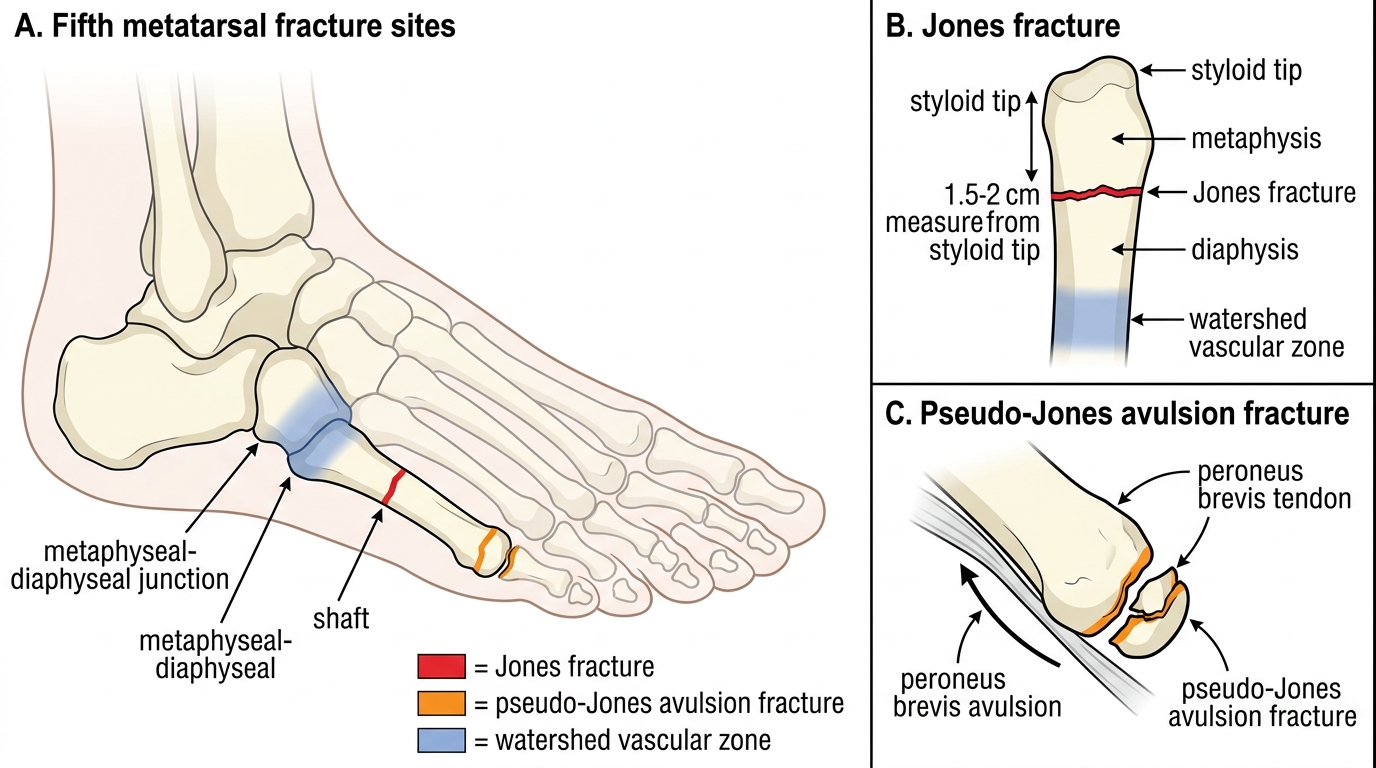
Jones vs Pseudo-Jones Fracture of the Fifth Metatarsal
Lisfranc Fracture-Dislocation — Anatomy, Mechanism, Diagnosis, and Management
The Lisfranc joint complex is the tarsometatarsal (TMT) joint region, comprising the articulations between the five metatarsal bases and the cuneiforms plus cuboid. The stability of this region depends on a network of dorsal, plantar, and interosseous ligaments, of which the Lisfranc ligament (the interosseous ligament from the medial cuneiform to the base of the second metatarsal) is the strongest and the key stabiliser. The second metatarsal is recessed between the medial and lateral cuneiforms, forming a 'keystone' that locks the transverse arch; disruption of this keystone allows dorsal or lateral subluxation of the metatarsals.
Mechanism: high-energy (direct crush, road traffic accident) or low-energy (indirect twisting, foot plantarflexed and axially loaded — the 'cleat-catching' mechanism in athletes). The classic low-energy mechanism is a windsurfer or horse-rider whose foot is caught while falling. Indirect injuries produce the characteristic pattern of the first metatarsal separating medially while the remaining metatarsals displace laterally (homolateral) or the metatarsals diverge in a divergent pattern.
Clinical diagnosis is often delayed because the injury may look deceptively minor on plain X-ray. Red flags: midfoot pain after any twisting or loading mechanism; inability to bear weight; plantar ecchymosis (pathognomonic — bruising in the plantar arch signifying plantar capsule tear); swelling and tenderness localised to the TMT joints. The piano-key test: longitudinal pressure on each metatarsal head while the ankle is held — pain at the TMT level is highly specific.
Radiographic diagnosis: weight-bearing AP, lateral, and 30° oblique views of the foot are mandatory. Key radiographic signs: loss of alignment between the medial border of the second metatarsal and the medial border of the intermediate cuneiform (the normal 'straight-line' relationship on AP view); diastasis >2 mm between the bases of the first and second metatarsals; avulsion fracture of the base of the second metatarsal (a 'fleck sign' adjacent to the Lisfranc ligament — diagnostic when present). If plain films are equivocal but clinical suspicion is high, CT is the investigation of choice to identify subtle malalignment and associated fractures.
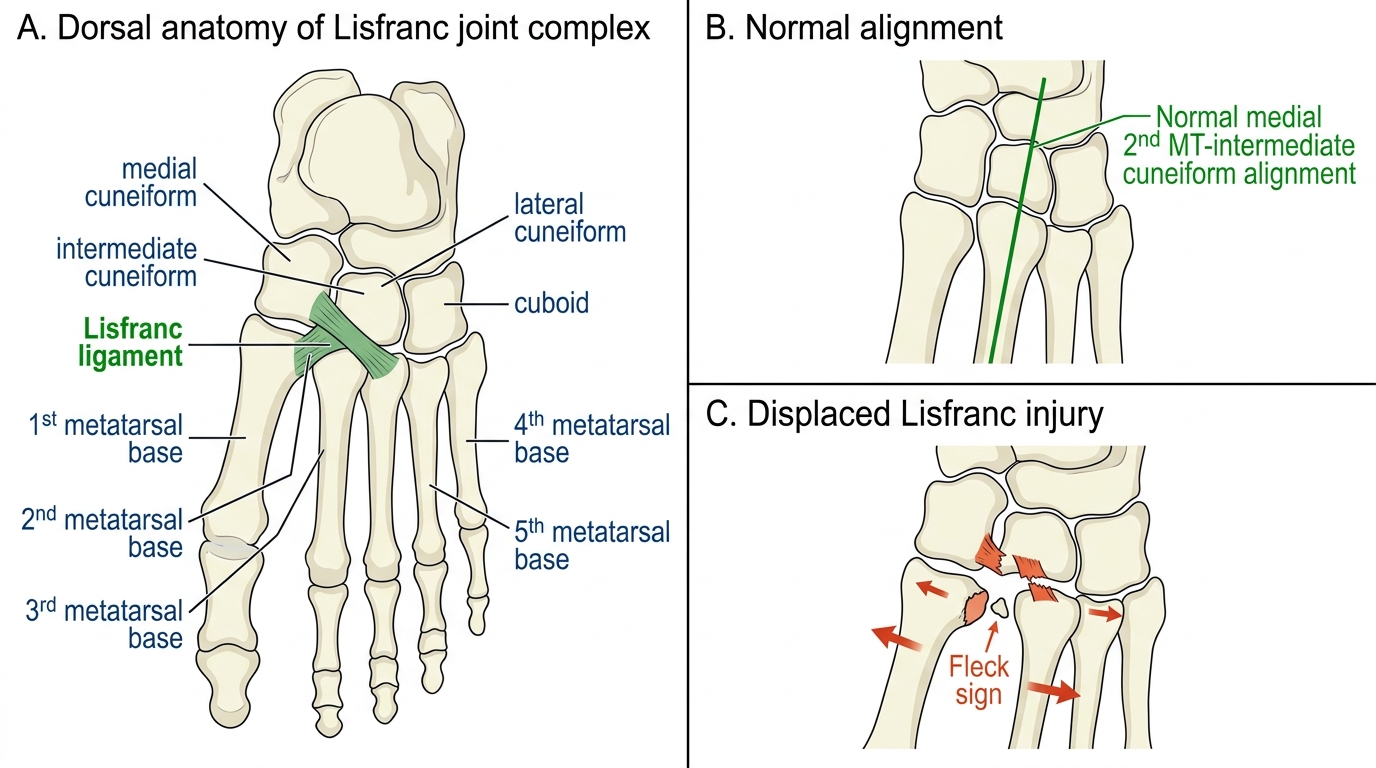
Lisfranc Joint Complex: Normal Anatomy and Displaced Injury