Page 2 of 22
OR2.10 | Patella and Peri-knee Fracture Management — SDL Guide (Part 2)
Investigation — Radiography and Advanced Imaging
Provided image
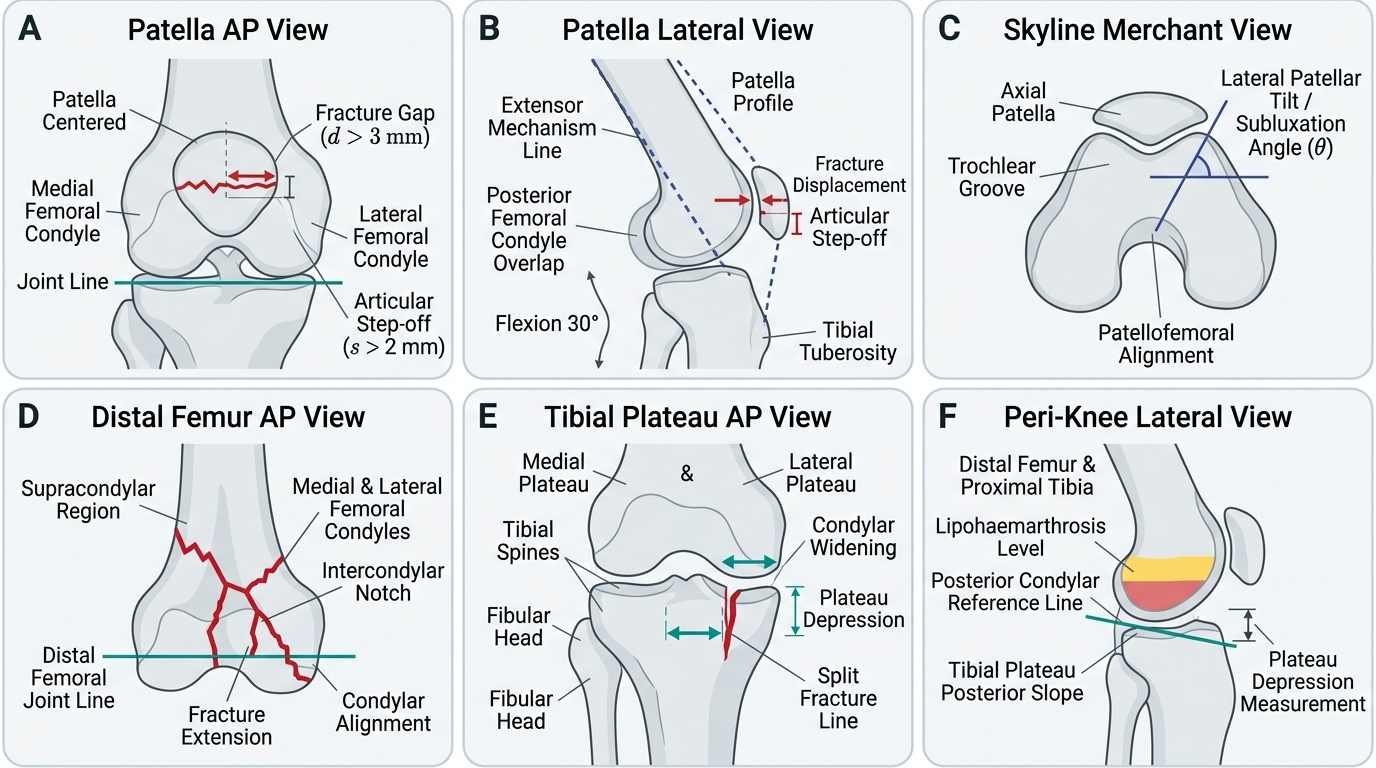
The initial imaging protocol for all peri-knee fractures begins with plain radiographs in two orthogonal planes: anteroposterior (AP) and lateral projections of the knee, including the full distal femur and proximal tibia on the same film where possible. For the patella, a skyline (tangential, Merchant's) view is invaluable to assess comminution and displacement in the axial plane. The AP radiograph of a tibial plateau fracture may underestimate the degree of articular depression — the classic teaching is that depression is always worse on CT than it appears on plain film. Computed tomography (CT) with coronal, sagittal, and 3D reconstructions is now standard for all distal femur fractures with intra-articular extension and all Schatzker III–VI tibial plateau fractures, because the articular surface reconstruction is crucial for operative planning: surgeons must know the exact extent, location, and depth of depression before choosing a fixation strategy.
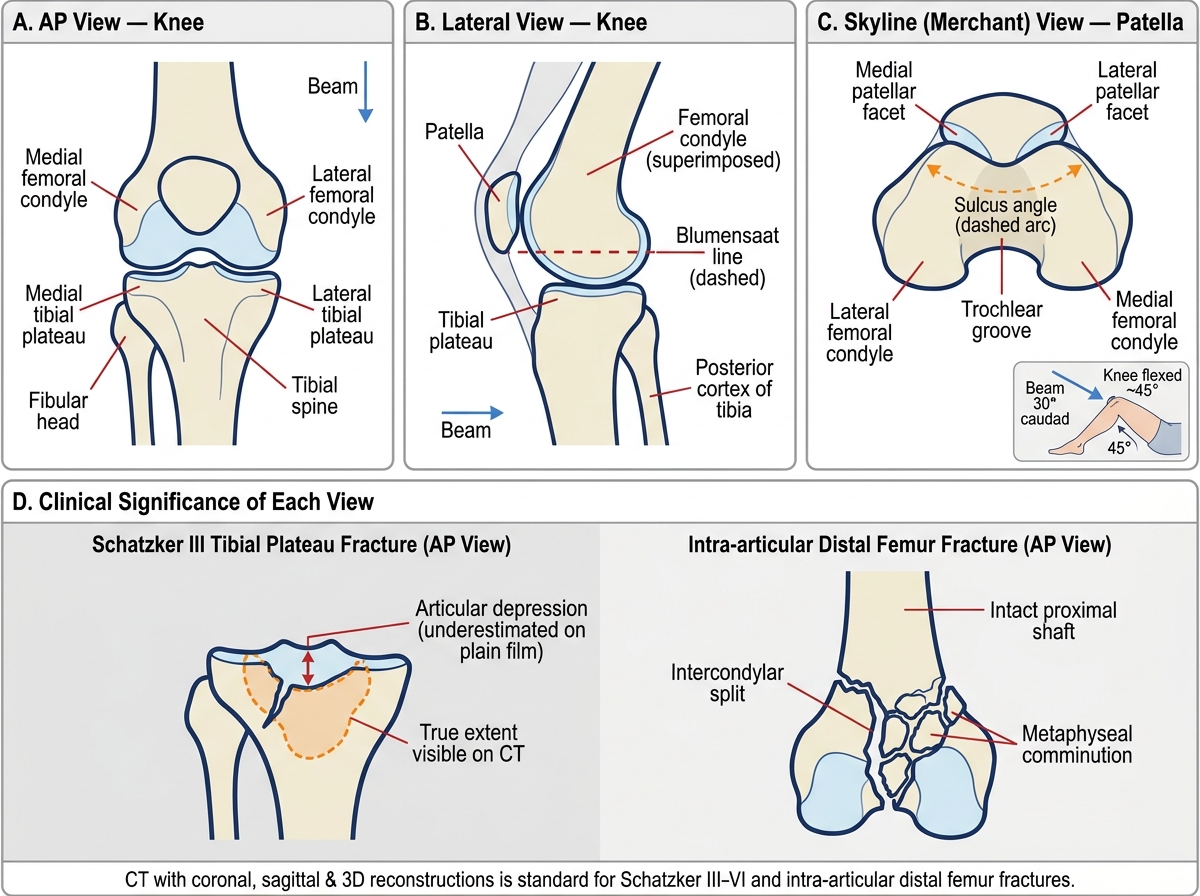
Radiographic Views for Peri-Knee Fractures with Key Measurement Landmarks
Vascular investigation: any clinical suspicion of popliteal artery injury (absent or diminished pulses, ABI <0.9, expanding haematoma, bruit) mandates CT angiography or formal angiography and emergency vascular surgery consultation. Duplex Doppler alone is insufficient when the index of suspicion is high.
MRI is rarely used acutely but is valuable for assessing concomitant ligamentous and meniscal injuries in tibial plateau fractures — particularly important for Schatzker Types I–III where definitive fixation is being planned and associated soft tissue injury changes the surgical approach.
Management of Patellar Fractures
The management decision for patellar fractures hinges entirely on two factors: the degree of displacement (a gap >3 mm between fragments) and the integrity of the extensor mechanism (ability to perform active straight-leg raise). Non-displaced or minimally displaced fractures (<3 mm gap) with an intact extensor mechanism are managed non-operatively with a cylinder plaster cast or knee immobiliser in full extension for 4–6 weeks, followed by physiotherapy. Operative indications are a gap >3 mm, articular step-off >2 mm, or a failed straight-leg raise test indicating extensor mechanism disruption.
The standard operative technique for transverse fractures is tension band wiring (TBW): two parallel 2 mm K-wires are passed longitudinally through both fragments, and a figure-of-8 cerclage wire is added anterior to the K-wires, converting the tensile force of the quadriceps into compression at the fracture site. This converts a distracting force to a compressive force — a principle universally applicable in orthopaedic fixation of tension-side injuries. Comminuted fractures may require circumferential wiring, partial patellectomy with advancement of the retinaculum, or in severe cases total patellectomy (reserved as a last resort, as it permanently weakens the extensor mechanism). Early mobilisation is encouraged after internal fixation.
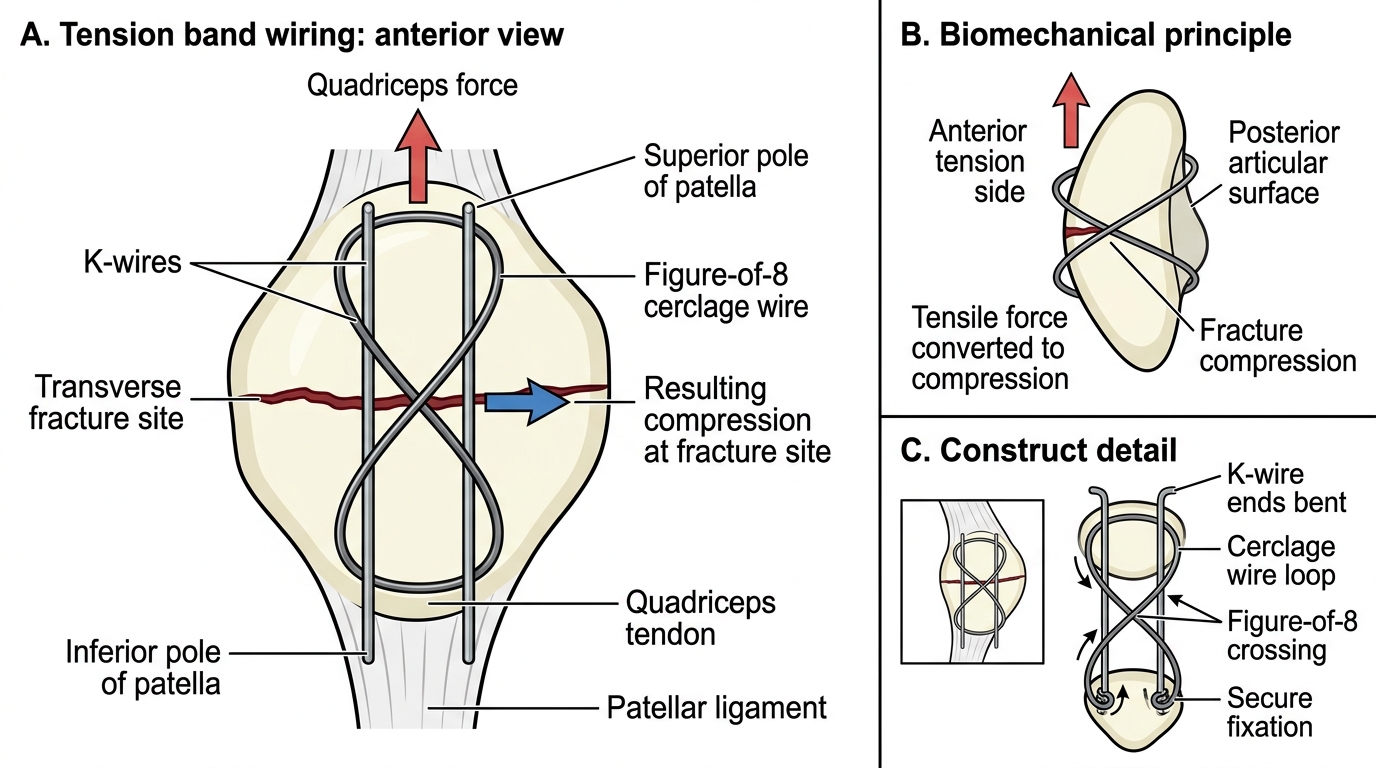
Tension Band Wiring of Transverse Patellar Fracture
Management of Distal Femur and Tibial Plateau Fractures
Distal femur fractures in young adults with displaced or intra-articular patterns are managed operatively. The principle of management follows the AO protocol: anatomic reduction of the articular surface first, then restoration of length, alignment, and rotation of the metaphyseal-diaphyseal component. The retrograde intramedullary nail (IMN) is the workhorse for AO type A (extra-articular) fractures; locking plate systems (lateral or medial locking condylar plates) are preferred for complex articular (type C) fractures because they allow simultaneous fixation of condylar fragments and the shaft. Temporary external fixation ('damage control orthopaedics') is used when the patient is physiologically unstable or soft tissue swelling prohibits definitive fixation. Non-operative management (traction, cast-bracing) is acceptable only in elderly non-ambulatory patients or those unfit for anaesthesia.
For tibial plateau fractures, non-operative management (long-leg cast or hinged brace, non-weight-bearing) is appropriate for Schatzker Types I–III with <3 mm articular depression and <5° varus/valgus instability, provided neurovascular status is normal. Operative management (open reduction and internal fixation, ORIF) is indicated for: >3 mm articular depression, unstable patterns, neurovascular injury, compartment syndrome (fasciotomy is the priority), and Schatzker Types IV–VI. Bone grafting of the depressed articular segment is standard — the subchondral void left after elevating the depression must be filled with autograft or synthetic bone substitute to prevent re-depression.
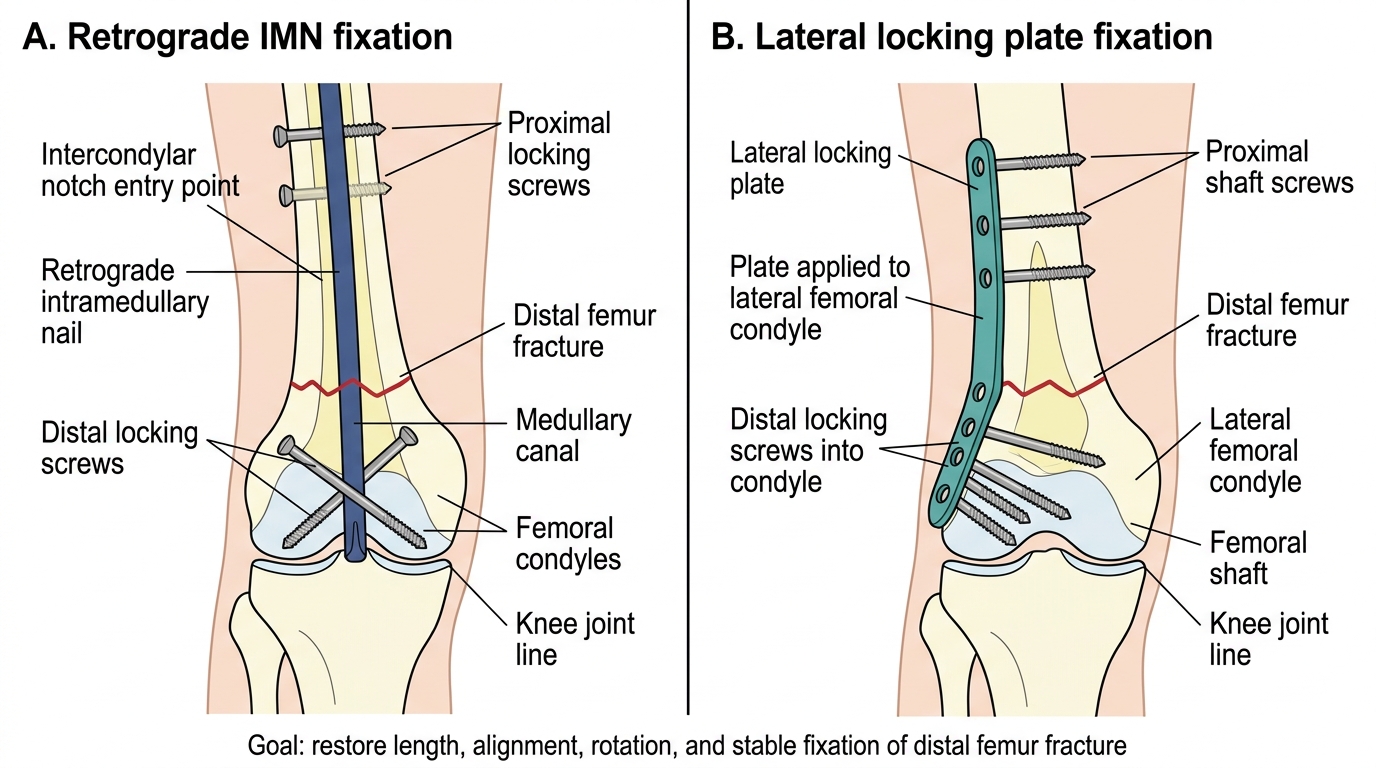
Distal Femur Fracture Fixation: Retrograde IMN vs Locking Plate
SELF-CHECK
A 45-year-old woman sustains a Schatzker Type II tibial plateau fracture (lateral split-depression, 6 mm articular depression). She has no neurovascular deficit. Which management is most appropriate?
A. Long-leg cast in full extension for 8 weeks
B. Open reduction and internal fixation with bone grafting of the depressed segment
C. Immediate total knee arthroplasty
D. Percutaneous K-wire fixation without addressing the articular depression
Reveal Answer
Answer: B. Open reduction and internal fixation with bone grafting of the depressed segment
Articular depression >3 mm in a tibial plateau fracture is an operative indication. ORIF involves elevating the depressed articular segment, filling the subchondral void with bone graft or substitute, and securing the lateral fragment with buttress plating and lag screws. Failure to address the depression leads to valgus deformity, early post-traumatic osteoarthritis, and knee instability.