Page 4 of 22
OR2.2 | Proximal Humerus Fracture Management — SDL Guide
Learning Objectives
- Describe the mechanisms of proximal humerus fractures and the relevant anatomy of the proximal humeral blood supply
- Apply the Neer four-part classification to identify part-number and displacement status
- Recognise the axillary nerve as the key nerve at risk and describe its course and testing
- Differentiate non-operative from operative management indications, including arthroplasty for four-part fractures
- Identify complications including avascular necrosis, axillary nerve palsy, and post-traumatic stiffness
INSTRUCTIONS
Proximal humerus fractures are the third most common fracture in adults, with a strong predilection for elderly women with osteoporosis. As a final-year student you will see these in casualty and fracture clinics; the majority are managed non-operatively, but identifying the minority requiring surgery -- particularly the four-part fracture in a young patient versus the elderly patient better served by arthroplasty -- is a core clinical decision. The Neer classification and the concept of head-splitting and blood-supply disruption are the conceptual foundations for this module.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch 20 -- Fractures of the Shoulder Girdle (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 29 -- Injuries of the Shoulder (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 72-year-old woman with known osteoporosis falls on her outstretched right arm while descending stairs. She presents with a swollen, bruised right shoulder, inability to abduct the arm, and severe pain. Plain radiographs show a four-part proximal humerus fracture with displacement of all four fragments. Neurological examination reveals anaesthesia over the regimental badge area of the right deltoid. How do you classify this fracture, what is the nerve injury, and how does the patient's age and fracture pattern influence management?
WHY THIS MATTERS
Proximal humerus fractures account for approximately 5% of all fractures and are the third most common fracture site in adults, exceeded only by hip and wrist fractures. They are predominantly an osteoporotic injury of older women, but high-energy fractures occur in younger patients. The key decision in management -- non-operative immobilisation versus operative fixation versus primary arthroplasty -- depends on understanding the Neer classification, the blood supply to the humeral head, and the patient's physiological age and functional demands. Missed axillary nerve injury leads to permanent deltoid paralysis and a flail shoulder; understanding its anatomy and testing it routinely prevents this outcome.
RECALL
Before proceeding, recall from your anatomy studies that the proximal humerus comprises four segments described by Neer: the articular segment (head), the greater tuberosity, the lesser tuberosity, and the shaft. The axillary nerve arises from the posterior cord of the brachial plexus (C5-C6), winds around the surgical neck of the humerus in the quadrilateral space, and supplies the deltoid and teres minor, with a cutaneous branch to the regimental badge area. The anterior humeral circumflex artery (arcuate artery) is the main blood supply to the humeral head, entering through the intertubercular groove; disruption in four-part fractures explains the risk of avascular necrosis.
Mechanism of Injury and Applied Anatomy
The proximal humerus fractures occur by two dominant mechanisms. In the elderly, a low-energy fall on an outstretched hand (FOOSH) transmits force through the extended elbow and wrist to the shoulder; the osteoporotic cancellous bone of the humeral head fails at relatively low loads, producing the characteristic impacted or displaced fractures seen in this age group. In younger patients, the mechanism is high-energy direct trauma (motor vehicle accidents, falls from height), producing comminuted or multi-part patterns. Direct impact to the lateral shoulder (fall on the side) can also produce isolated greater tuberosity fractures. The anatomy of the proximal humerus determines the displacement pattern: the supraspinatus, infraspinatus, and teres minor pull the greater tuberosity posterosuperiorly; the subscapularis pulls the lesser tuberosity anteromedially; the pectoralis major displaces the shaft anteromedially. These muscle vectors create the characteristic displacement seen in each fracture type. The anterior humeral circumflex artery (the arcuate artery of Laing) enters the intertubercular groove and is the principal blood supply to the articular segment; the posterior humeral circumflex contributes secondarily. In four-part fractures all soft-tissue attachments to the head are disrupted, interrupting this supply and creating the substrate for avascular necrosis (AVN) of the humeral head.
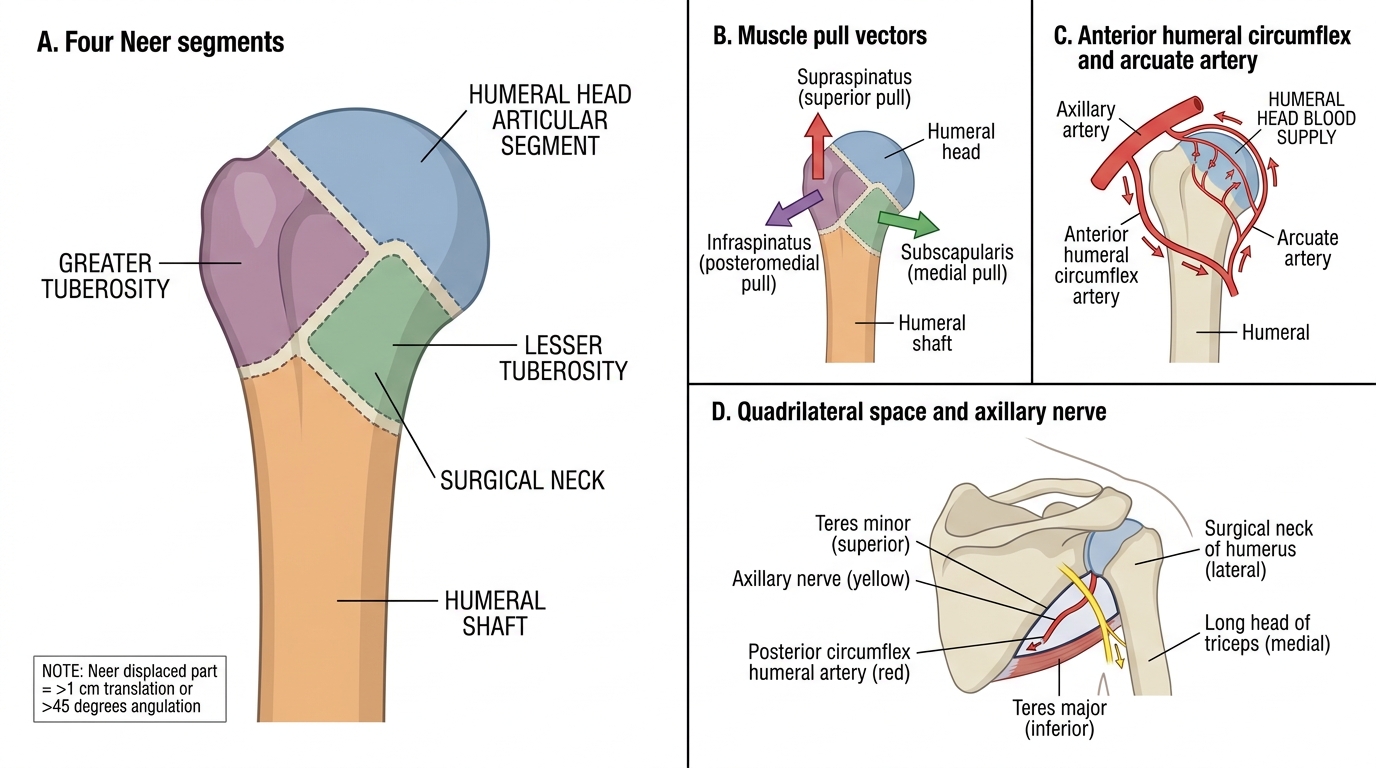
Proximal Humerus: Neer Segments, Muscle Pulls, Blood Supply, and Axillary Nerve
Fracture Classification -- Neer Four-Part System
The Neer classification (1970) is the standard clinical system for proximal humerus fractures. It defines 'parts' not by anatomical segments per se, but by segments that are displaced: displacement is defined as >1 cm of translation or >45 degrees of angulation. A fracture is classified by the number of displaced parts: one-part (no segment displaced -- most common, ~80%); two-part (one segment displaced); three-part (two segments displaced); four-part (all four segments displaced -- head articular segment, greater tuberosity, lesser tuberosity, and shaft). A separate category is the head-splitting fracture, where the articular surface itself is divided. Neer also classified fracture-dislocations (in which the humeral head dislocates anterior or posterior), which carry additional risks of AVN and nerve injury. The prognostic importance of the Neer system is that the number of displaced parts correlates with blood-supply disruption and AVN risk: one-part fractures rarely develop AVN; four-part fractures have an AVN risk of 13-34% even with optimal operative fixation. Understanding these rates is essential for counselling patients about outcomes and implant choice.
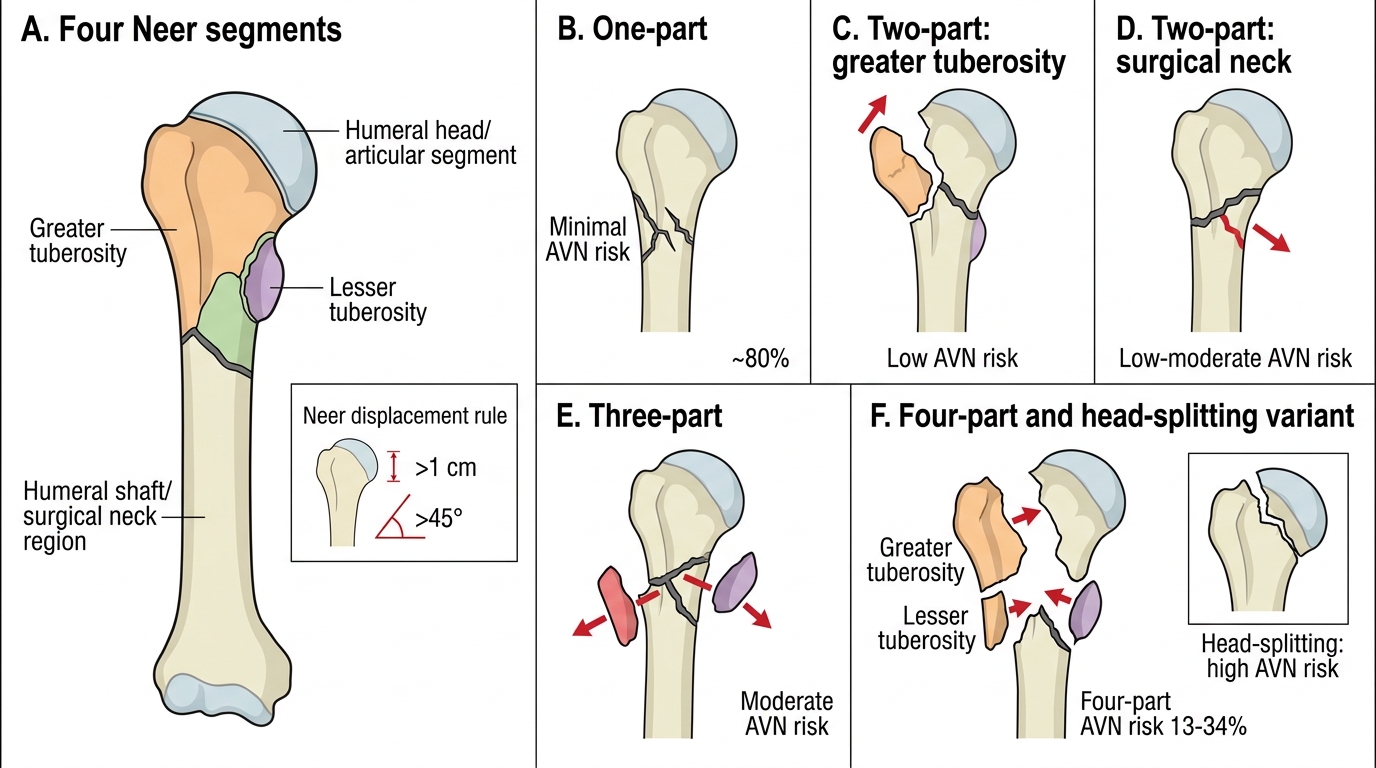
Neer Classification of Proximal Humerus Fractures
| Neer type | Description | Frequency | AVN risk |
|---|---|---|---|
| One-part | No segment displaced >1 cm or >45 degrees | ~80% | Minimal |
| Two-part (GT) | Greater tuberosity displaced | Common | Low |
| Two-part (SN) | Surgical neck displaced | Common | Low-moderate |
| Three-part | Two segments displaced | Less common | Moderate |
| Four-part | All four segments displaced | Uncommon | 13-34% |
| Head-splitting | Articular surface cleft | Rare | Very high |
Clinical Examination and Investigations
The clinical presentation of a proximal humerus fracture is usually straightforward: the patient cradles the injured arm, the shoulder is swollen and bruised, and there is exquisite tenderness over the proximal humerus and acromion. The bruising characteristically tracks down the lateral chest wall and upper arm over 24-48 hours -- this is a helpful sign distinguishing proximal humerus fracture from AC joint injury or rotator cuff tear where bruising is more localised. Active shoulder movement is impossible and passive range is severely restricted by pain. The critical examination step is the axillary nerve assessment: test sensation over the regimental badge area (a 4 cm circular area over the lateral deltoid, two finger-breadths below the acromion) and assess deltoid contraction (ask the patient to gently push the elbow into the examiner's hand while palpating the deltoid). Axillary nerve injury is present in up to 45% of proximal humerus fractures in some series; most are neuropraxias that recover, but the deficit must be documented before and after reduction/fixation. Also assess the radial, median, and ulnar nerves distally, check brachial and radial pulses (axillary artery injury is rare but occurs in displaced fractures), and screen for shoulder dislocation.
Regimental Badge Area and Axillary Nerve Assessment
Investigations:
- AP and lateral shoulder radiographs (scapular Y view useful for dislocation)
- Axillary view: assesses glenoid and rules out dislocation
- CT with 3D reconstruction: essential for complex multi-part fractures and pre-operative planning; clarifies part-number better than plain films
- MRI: for suspected rotator cuff tear (commonly associated with two-part greater tuberosity fractures)
SELF-CHECK
A 70-year-old woman has a proximal humerus fracture with all four Neer segments displaced. Which complication has the highest incidence with this fracture pattern, even after successful operative fixation?
A. Axillary artery injury requiring vascular repair
B. Avascular necrosis (AVN) of the humeral head (risk 13-34%)
C. Shoulder dislocation requiring immediate reduction
D. Radial nerve palsy causing wrist drop
Reveal Answer
Answer: B. Avascular necrosis (AVN) of the humeral head (risk 13-34%)
Four-part fractures disrupt all soft-tissue attachments to the articular segment, including the anterior humeral circumflex artery (arcuate artery), which is the principal blood supply to the humeral head. This creates the substrate for AVN, occurring in 13-34% of cases even after anatomical fixation. Axillary artery injury is rare; radial nerve is not at risk from proximal humerus fractures (it is endangered at the humeral shaft); and dislocation, while possible, is a separate classification category.