Page 1 of 18
OR3.1 | Bone and Joint Infection Assessment — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis and routes of infection in acute, subacute, and chronic osteomyelitis and septic arthritis
- Differentiate the clinical presentations of pyogenic osteomyelitis (acute and subacute) from tuberculous bone and joint infection based on tempo, systemic features, and imaging
- Interpret investigations including blood cultures, plain radiographs, MRI, and bone scans to stage and classify musculoskeletal infection
- Outline the principles of antibiotic therapy, surgical drainage, sequestrectomy, and saucerisation in managing bone and joint infections
- Identify pathological hallmarks — Brodie's abscess, sequestrum, involucrum — and explain their clinical significance in chronic osteomyelitis
INSTRUCTIONS
Bone and joint infections remain a significant cause of morbidity in India, affecting all age groups from neonates to the elderly. Early recognition and appropriate management can prevent the transition from acute to chronic osteomyelitis — a much harder-to-treat state. As a future clinician you will encounter these conditions in district hospitals and emergency rooms; understanding the aetiopathogenesis, diagnostic approach, and treatment principles is essential to prevent long-term disability.
References
- Maheshwari's Essential Orthopaedics, Ch 20 — Infections of Bone and Joints (textbook)
- Apley and Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 2 — Infection (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 9-year-old boy is brought to the emergency department with a three-day history of high fever and severe pain in his right thigh. He refuses to bear weight and cries when the limb is gently touched. His mother reports that he had a skin boil on his knee two weeks ago. On examination his temperature is 39.2°C, the right distal femoral metaphysis is warm, swollen, and exquisitely tender. Blood tests reveal a white cell count of 18,000 cells/μL and a CRP of 140 mg/L. What is happening in his bone, and why did a skin boil trigger this cascade?
WHY THIS MATTERS
Musculoskeletal infections — acute osteomyelitis, septic arthritis, subacute osteomyelitis, and chronic osteomyelitis — are among the most time-critical orthopaedic diagnoses. A 24-hour delay in draining septic arthritis can cause permanent articular cartilage destruction. A missed acute osteomyelitis can evolve into chronic osteomyelitis, which requires multiple surgeries spanning months to years. India's high burden of TB means that every chronic bone or joint infection must be considered tuberculous until proven otherwise. A well-trained clinician must recognise the clinical fingerprints of each form and initiate the correct treatment pathway on the day of presentation.
RECALL
Before proceeding, recall the following from your anatomy and physiology modules: (1) The blood supply of long bones — the nutrient artery branches into the medullary sinusoids; the metaphyseal region in children has sluggish capillary flow and lacks phagocytic lining cells, making it vulnerable to bacterial seeding. (2) Articular cartilage has no blood supply and receives nutrition by diffusion from synovial fluid — pus in a joint immediately threatens this diffusion. (3) The periosteum in children is thick and loosely attached — it strips easily when subperiosteal pus accumulates. (4) The immune system: neutrophils are the first responders; their degranulation enzymes destroy both bacteria AND host tissue, including cartilage.
Aetiopathogenesis of Acute Haematogenous Osteomyelitis
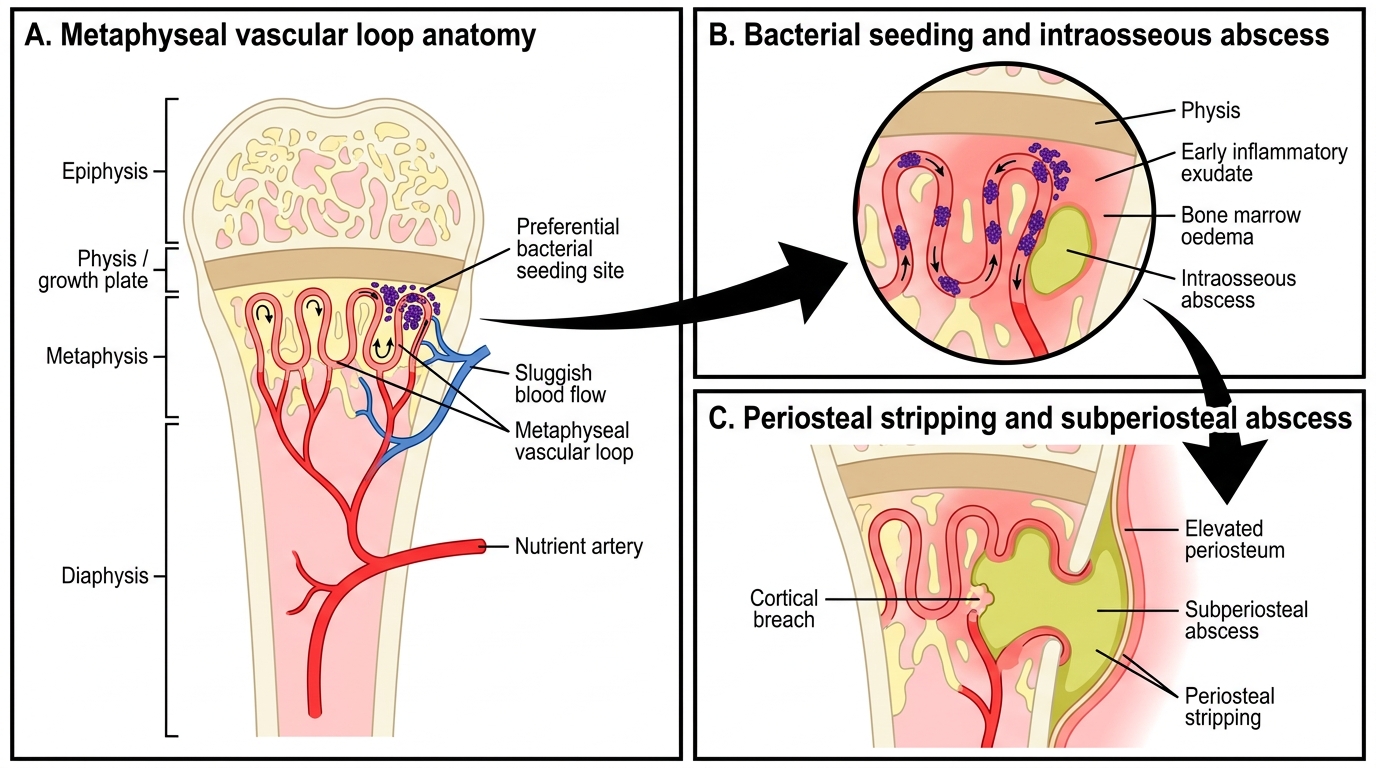
Acute haematogenous osteomyelitis (AHO) is the most common form of bone infection in children, and understanding its pathogenesis explains almost every clinical and radiological finding. Bacteria enter the bloodstream — from a distant focus such as a skin boil, furuncle, upper respiratory tract infection, dental abscess, or even a trivial abrasion — and are carried to bone by the arterial circulation. The metaphysis of rapidly growing long bones (distal femur, proximal tibia, proximal humerus) is preferentially affected because of a unique vascular anatomy: the terminal capillary loops in the metaphysis are wide, sluggish, and make sharp bends, creating turbulence and relative stasis. These capillaries also lack phagocytic endothelial lining cells, so bacteria can adhere and multiply without early immune clearance. In neonates, terminal capillaries actually cross the growth plate (physeal vessels), which means infection can spread directly to the epiphysis and joint, explaining why neonatal osteomyelitis so frequently causes concurrent septic arthritis and physeal destruction.
Once bacteria establish a focus, an acute inflammatory response begins — neutrophil migration, oedema, and exudate accumulate within the rigid osseous cavity, causing a rapid rise in intraosseous pressure. This pressure rise is the primary mechanism of bone pain. As pus accumulates, it strips the periosteum (which in children is loosely attached), creating a subperiosteal abscess. Stripping the periosteum deprives the cortex of its periosteal blood supply, contributing to cortical necrosis. If left untreated, the sequence progresses: intraosseous abscess → subperiosteal abscess → soft-tissue abscess → eventual skin perforation (sinus tract in chronic disease).
The commonest causative organism across all age groups is Staphylococcus aureus, responsible for approximately 60-70% of cases in children. In neonates, group B streptococcus and gram-negative organisms (Klebsiella) are important pathogens. In sickle-cell disease patients, Salmonella species are a well-known cause — the sickling of red cells creates ischaemic niches that favour Salmonella survival. In immunocompromised patients and those with HIV, opportunistic organisms and disseminated TB must be considered.
The Cierny-Mader classification of osteomyelitis stratifies by anatomy (medullary, superficial, localised, diffuse) and host physiology (A = normal, B = compromised locally or systemically, C = treatment risk exceeds benefit), guiding the complexity of surgical management.
Acute Haematogenous Osteomyelitis in the Metaphysis
Clinical Presentation and Examination Findings
The clinical presentation of acute osteomyelitis follows directly from the pathogenesis described above. In children, the classic triad is fever (often 38-40°C), localised bone pain, and pseudoparalysis (refusal to use the limb). The onset is typically abrupt, evolving over 24-72 hours. Parents may report a preceding skin infection or respiratory illness one to two weeks earlier. The child is often systemically unwell — irritable, anorexic, and febrile.
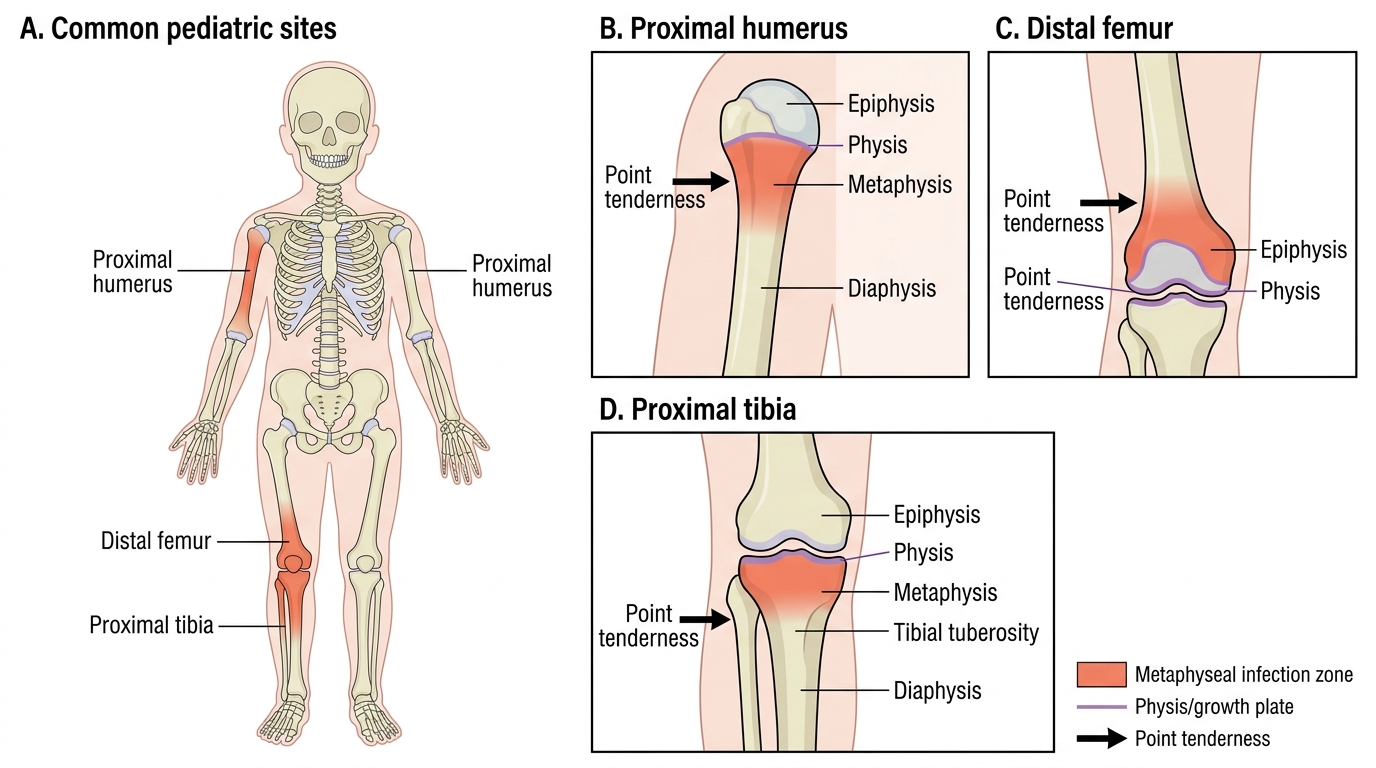
On physical examination, the hallmarks are point tenderness over the metaphysis, overlying soft-tissue oedema and warmth, and restriction of adjacent joint movement due to pain. At the distal femur, tenderness is maximal just above the knee; at the proximal tibia, just below the knee; at the proximal humerus, just below the shoulder. Crucially, the joint itself may move with less pain than the metaphysis — this distinguishes early osteomyelitis from septic arthritis, where joint movement is acutely painful in all directions.
In adults, haematogenous osteomyelitis is less common but does occur, particularly in the vertebrae (vertebral osteomyelitis, which affects the disc space and adjacent vertebral bodies), in intravenous drug users (unusual sites like clavicle and pubis), and following septicaemia in the elderly. The presentation in adults tends to be more indolent — weeks of back pain rather than acute fever.
In neonates, the presentation is often subtle: fever may be absent, the baby is simply irritable, reluctant to move a limb (pseudoparalysis), and the limb may be held in a characteristic position. Joint involvement is common in neonates because the physis is not yet a barrier.
Common Metaphyseal Sites of Acute Osteomyelitis in Children
Subacute Osteomyelitis and Brodie's Abscess
Subacute osteomyelitis represents a low-grade, indolent form of bone infection in which the host's immune response partially contains the infection without eradicating it. The organism — typically a less virulent strain of S. aureus — is not eliminated but is sequestered within a walled-off cavity. The result is a Brodie's abscess: a well-defined, oval or round lytic cavity within the metaphysis, typically surrounded by a rim of sclerotic (reactive) bone. The wall of sclerosis represents the body's containment barrier — a mix of reactive new bone and fibrous tissue.
Brodie's abscess was described by Sir Benjamin Brodie in 1832. It most commonly occurs at the proximal or distal tibia in adolescents and young adults. The clinical presentation is characteristically subacute and misleadingly benign: the patient reports weeks to months of intermittent, dull aching pain over the metaphysis, which may be worse at night. Systemic features (fever, toxicity) are typically absent or mild. Laboratory inflammatory markers (ESR, CRP, WBC) may be normal or only mildly elevated.
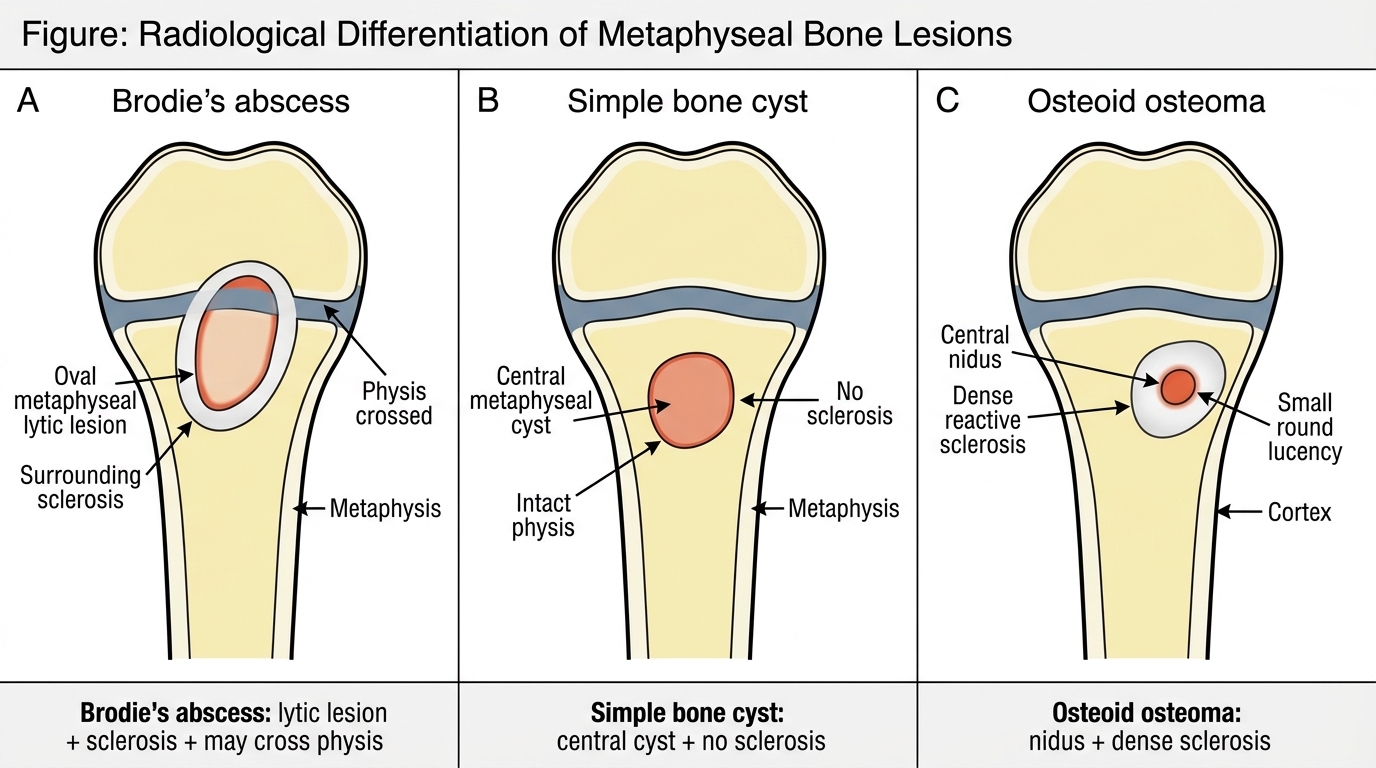
On plain radiograph, Brodie's abscess appears as a well-defined, oval lytic lesion in the metaphysis with surrounding sclerosis — it may extend across the physis into the epiphysis, a feature that helps distinguish it from bone tumours (which rarely cross the physis). The differential diagnosis includes bone cyst, osteoid osteoma (which has a nidus and more dense sclerosis), chondroblastoma, and eosinophilic granuloma. The Gledhill classification categorises Brodie's abscess radiologically by the extent and type of involvement (Types I-VI), which guides management.
Treatment of Brodie's abscess is surgical: curettage of the abscess cavity, removal of fibrous and infected tissue, and appropriate antibiotic cover. Because the cavity is walled off, IV antibiotics alone are rarely effective. After curettage, the cavity may be bone-grafted if large.
Radiological Differentiation of Metaphyseal Bone Lesions