Page 3 of 18
OR3.1 | Bone and Joint Infection Assessment — SDL Guide (Part 3)
Management of Chronic Osteomyelitis
The management of chronic osteomyelitis is invariably surgical because the sequestrum — the dead, avascular nidus of infection — cannot be sterilised by antibiotics alone. Medical management alone is destined to fail. The surgical principles are source control, debridement, and dead space management.
Sequestrectomy is the removal of the dead bone (sequestrum). This must be complete — leaving behind even small fragments perpetuates infection. The sequestrum is often visible on preoperative CT scan (which is superior to MRI for defining the extent of dead bone).
Saucerisation (or saucerization) refers to the surgical creation of a shallow saucer-like cavity in the bone by removing infected, necrotic, and sclerotic bone — essentially converting the enclosed cavity of infection into an open, well-vascularised shallow dish. This improves drainage, allows wound care, and enables granulation tissue ingrowth. The term is particularly used when a large cortical area is removed to convert a closed cavity into an open one.
After sequestrectomy and debridement, the remaining dead space must be managed. Options include: (1) cancellous bone grafting (once infection is controlled, autologous cancellous graft — from iliac crest — fills the cavity and revascularises); (2) antibiotic-impregnated beads (polymethylmethacrylate [PMMA] beads loaded with gentamicin or tobramycin, which provide high local antibiotic concentrations at the infected site while the bead acts as a temporary spacer — removed and replaced with bone graft in a staged procedure); (3) muscle flap coverage for exposed bone and soft-tissue defects; (4) Ilizarov techniques (distraction osteogenesis) for bone loss and deformity.
Systemic antibiotic therapy is an adjunct to surgery — ideally guided by culture and sensitivity of the intraoperative specimen — continued for 4-6 weeks post-operatively. The Cierny-Mader host grade influences the complexity of the reconstruction plan.
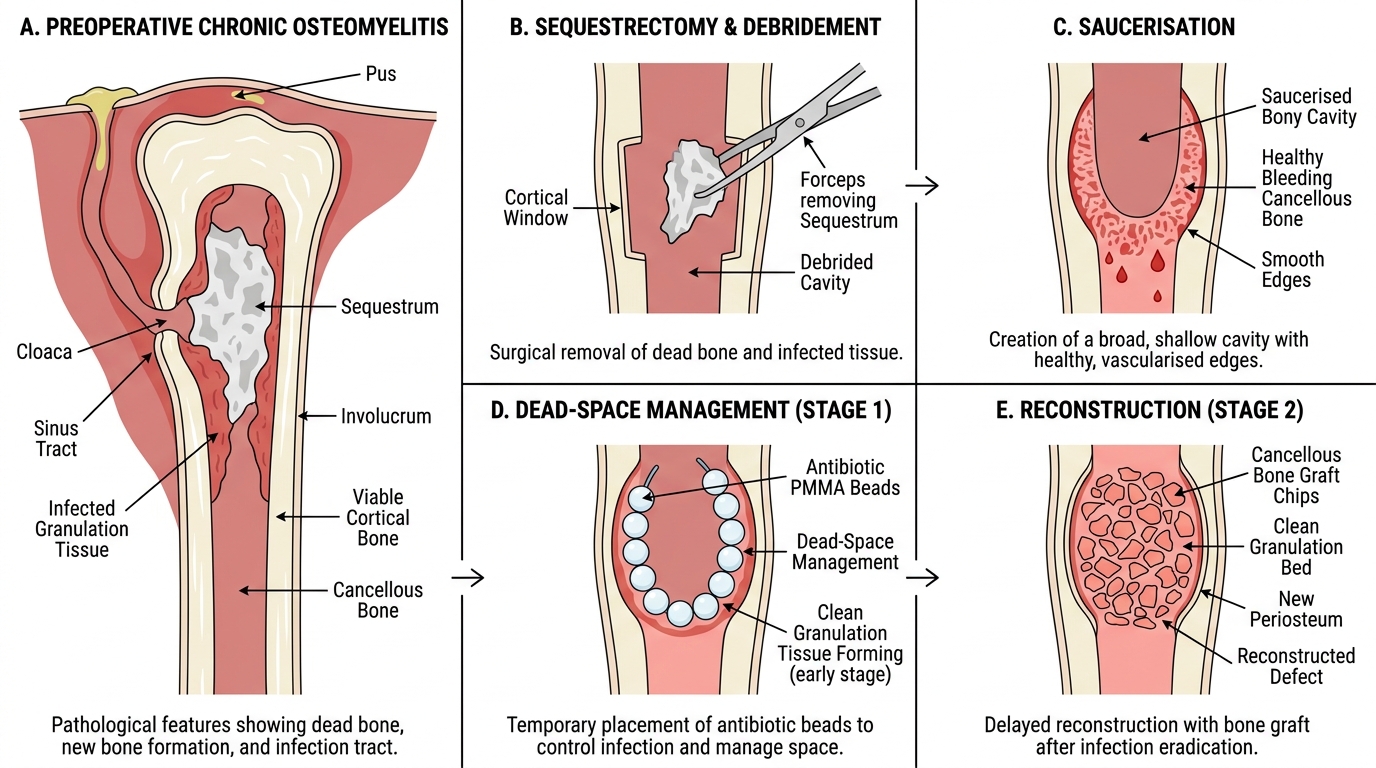
Staged Sequestrectomy and Saucerisation in Chronic Osteomyelitis
Septic Arthritis: Aetiopathogenesis and Clinical Features
Septic arthritis (pyogenic arthritis) is an infection of a synovial joint, representing an orthopaedic emergency because pus within a joint can destroy articular cartilage within hours to days. The joint is invaded by bacteria via three routes: (1) haematogenous seeding — bacteraemia seeds the synovium, which, unlike cartilage, has a rich blood supply and is therefore vulnerable to haematogenous seeding; (2) direct extension from adjacent osteomyelitis — particularly in joints where the metaphysis is intracapsular (e.g., the hip, where the proximal femoral metaphysis lies inside the joint capsule, making septic arthritis a frequent complication of neonatal/infant hip osteomyelitis); and (3) direct inoculation from a penetrating wound, joint injection, or arthroscopy.
The pathophysiology of cartilage destruction is rapid and devastating. Bacteria release proteases and toxins; the host inflammatory response generates large quantities of neutrophil-derived lysosomal enzymes (including metalloproteinases and collagenases). Simultaneously, the distended joint capsule may occlude the femoral head blood supply (in the hip), adding avascular necrosis to cartilage destruction. Pus in the joint raises intra-articular pressure, mechanically compressing capillaries and worsening ischaemia. Within 24-48 hours, cartilage may be irreversibly damaged.
The commonest organism in children and adults is S. aureus. In sexually active adults aged 16-35, Neisseria gonorrhoeae is the commonest cause in Western populations (less so in India). In neonates, group B streptococcus and gram-negative organisms are important. In patients with HIV infection, septic arthritis may be caused by S. aureus, opportunistic organisms, Salmonella, or Mycobacterium tuberculosis (the last presenting as an indolent mono-arthritis as part of immune reconstitution or as primary TB arthritis). HIV patients may also develop reactive arthritis as an immune phenomenon unrelated to direct joint infection.
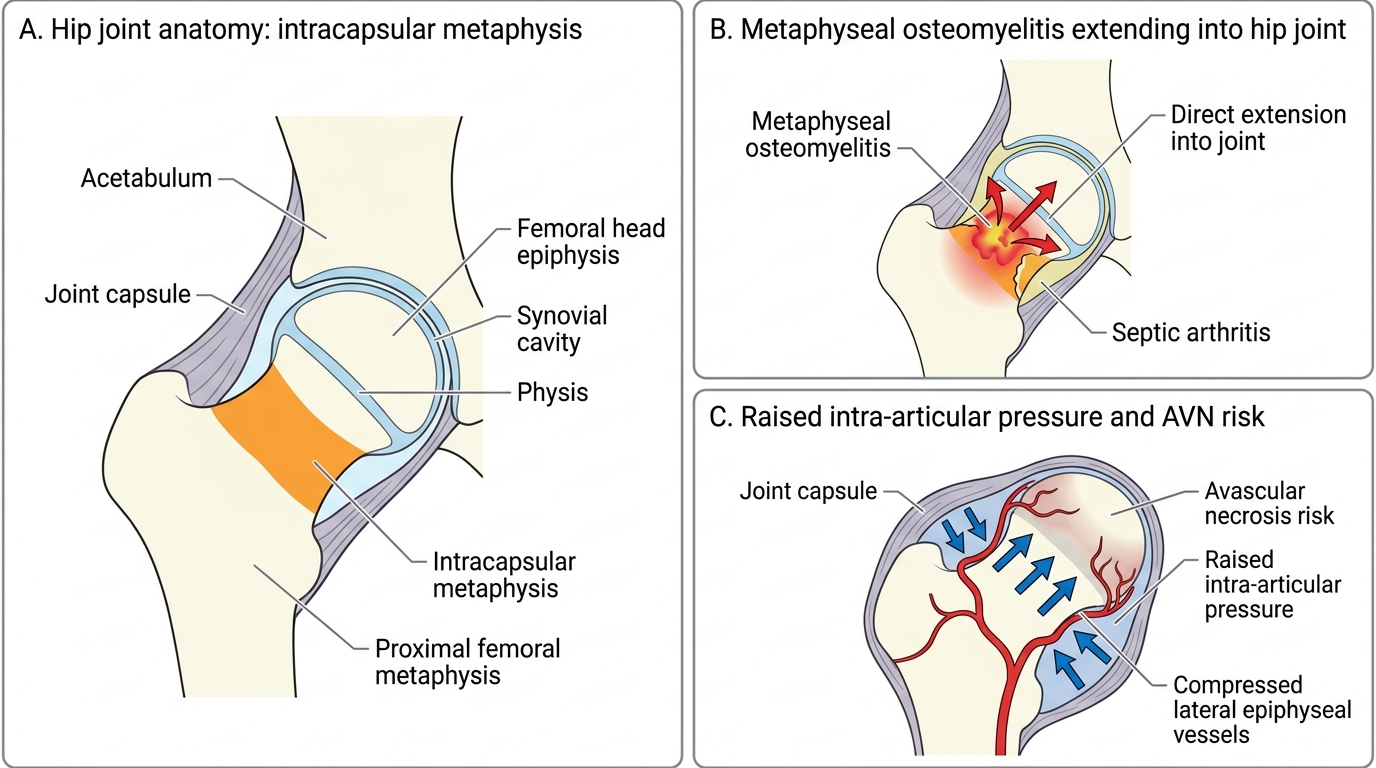
Hip Septic Arthritis: Intracapsular Metaphysis and AVN Risk
Septic Arthritis: Investigations and Management
The diagnosis of septic arthritis is confirmed by joint aspiration (arthrocentesis) — this is both diagnostic and initially therapeutic by reducing intra-articular pressure. Every suspected septic joint must be aspirated without delay. Synovial fluid analysis is the cornerstone of diagnosis:
The Kocher criteria (for the hip in children) combine four clinical and laboratory parameters to distinguish septic arthritis from transient synovitis: (1) non-weight-bearing, (2) ESR >40 mm/h, (3) fever >38.5°C, and (4) WBC >12,000/μL. Four criteria predict a 99.6% probability of septic arthritis; zero criteria essentially exclude it. A predicted probability >40% indicates the need for urgent joint aspiration and probable surgical drainage.
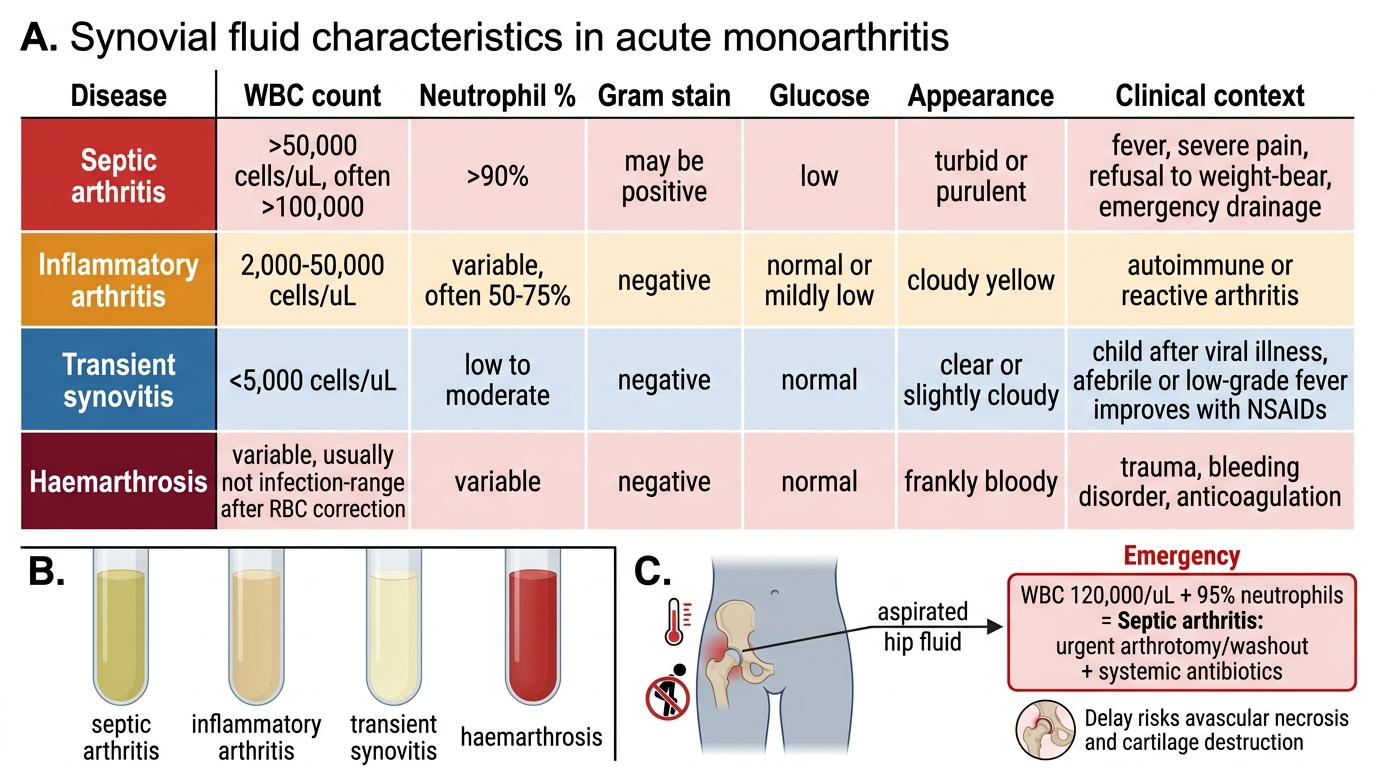
The synovial fluid analysis should include cell count, Gram stain, culture and sensitivity, glucose, and protein. Septic arthritis typically shows:
- WBC >50,000 cells/μL (often >100,000) with >90% neutrophils
- Low glucose (<50% of simultaneous blood glucose)
- Positive Gram stain in ~50-70% of cases
- Culture positive in ~70-85% of cases
Comparison with other joint effusions: inflammatory arthritis (RA, crystal) = 10,000-50,000 WBC; transient synovitis = <5,000 WBC predominantly mononuclear; haemarthrosis = predominantly red cells.
Radiologically, plain X-rays may show joint space widening (from effusion) and soft-tissue swelling. Ultrasound is the most rapid method to detect a joint effusion (particularly in the hip) and to guide aspiration. MRI shows synovial enhancement, effusion, and adjacent bone oedema.
Management requires urgent surgical drainage (arthrotomy or arthroscopic washout), combined with systemic antibiotics. Septic arthritis of the hip is a surgical emergency — the hip must be opened and drained within hours to prevent avascular necrosis. Post-drainage, antibiotics are continued intravenously until clinical and laboratory improvement, then completed orally for a total of 3-6 weeks. Joint splintage in a position of comfort reduces pain; physiotherapy and early mobilisation are begun once infection is controlled to prevent stiffness.
Synovial Fluid Patterns in Acute Monoarthritis
SELF-CHECK
A 4-year-old boy with fever and refusal to weight-bear has synovial fluid aspirated from his left hip showing WBC 120,000 cells/μL with 95% neutrophils. Which diagnosis is most likely and what is the immediate next step?
A. Transient synovitis — reassure parents and prescribe NSAIDs
B. Reactive arthritis — arrange outpatient blood tests
C. Septic arthritis — urgent surgical arthrotomy and washout with systemic antibiotics
D. Rheumatoid arthritis — refer to paediatric rheumatology
Reveal Answer
Answer: C. Septic arthritis — urgent surgical arthrotomy and washout with systemic antibiotics
A WBC >50,000 with >90% neutrophils in joint fluid is diagnostic of septic arthritis. Transient synovitis shows <5,000 WBC. The hip must be surgically drained urgently — delay risks avascular necrosis from pressure on the lateral epiphyseal arteries and from direct enzymatic cartilage destruction.