Page 7 of 18
OR3.2 | Joint Aspiration Practice — SDL Guide (Part 2)
Synovial Fluid Analysis: Interpretation of Findings
Synovial fluid analysis is the cornerstone of septic arthritis diagnosis and the primary output of joint aspiration. A systematic approach to interpretation — beginning with gross appearance and progressing to cell count, biochemistry, and microbiology — allows the clinician to reach a diagnosis rapidly and confidently. Every parameter of the analysis contributes a different dimension of information: gross appearance gives an instant qualitative signal, cell count provides the critical diagnostic threshold, biochemistry contextualises the cellular findings, and microbiology identifies the causative organism to guide targeted therapy.
Gross appearance: Normal fluid is clear and straw-coloured with high viscosity (the 'string test': it forms a long string when pulled from the syringe). Infected fluid is turbid, cloudy or frankly purulent (pus-like), with reduced viscosity because bacterial enzymes and leucocytes break down hyaluronan. A haemarthrosis is uniformly bloody or xanthochromic (yellow-tinged if old blood). Crystal arthropathies may produce turbid fluid (heavy crystal load).
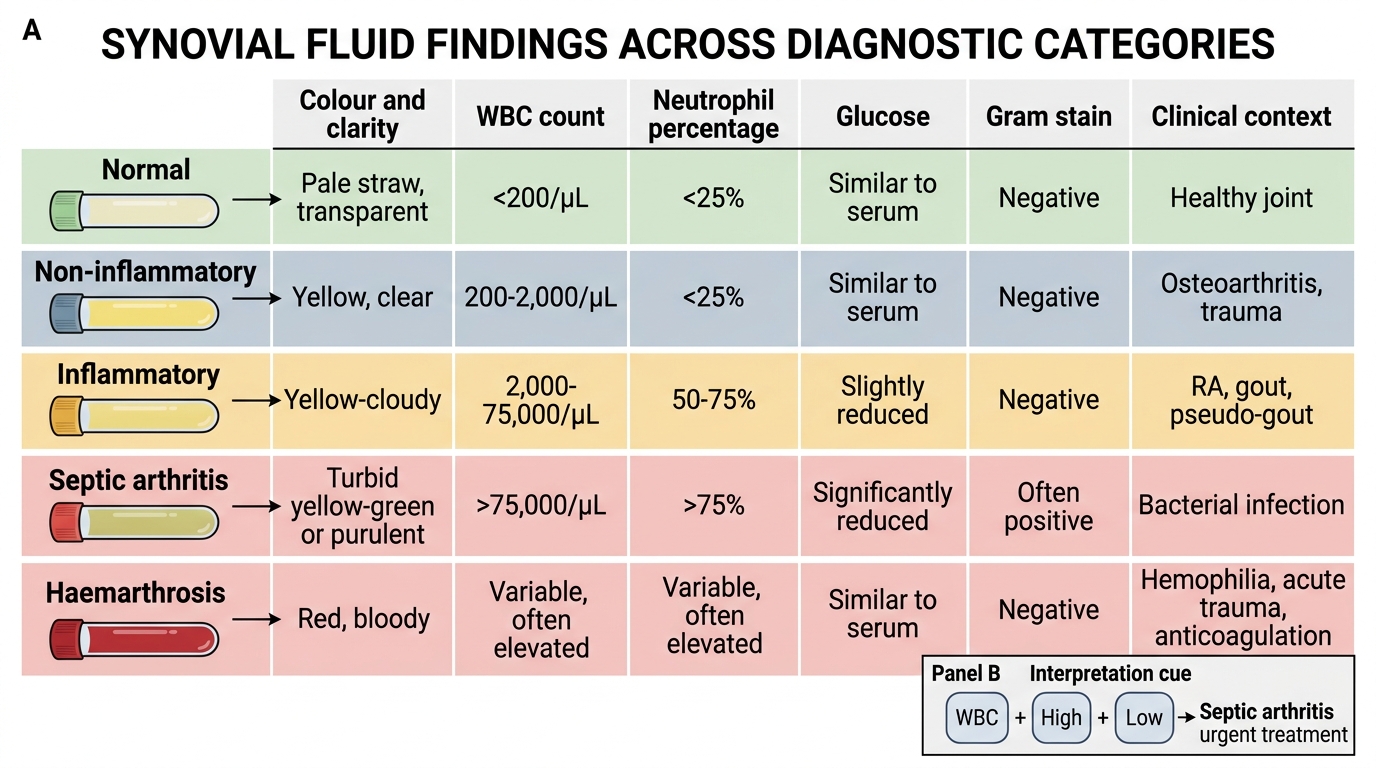
Cell count and differential — the most critical parameter:
| Diagnosis | WBC (cells/μL) | Neutrophil % | Appearance |
|---|---|---|---|
| Normal | <200 | <25% | Clear, straw |
| Non-inflammatory (OA, trauma) | 200-2,000 | <25% | Clear-yellow |
| Inflammatory (RA, crystal, reactive) | 2,000-50,000 | 50-75% | Turbid |
| Septic arthritis | >50,000 (often >100,000) | >90% | Turbid/purulent |
| Haemarthrosis | RBC-dominant | Variable | Bloody |
A WBC cut-off of >50,000 cells/μL with >90% neutrophils is the standard threshold for presumptive septic arthritis, though values between 25,000-50,000 in a febrile patient should also be treated as septic until proven otherwise.
Glucose: Normally, synovial fluid glucose is approximately equal to (or slightly less than) serum glucose. In septic arthritis, bacteria and leucocytes consume glucose — synovial glucose falls to less than 50% of the simultaneous blood glucose. This is a supporting finding rather than a standalone diagnostic criterion.
Gram stain: The Gram stain identifies the causative organism immediately, allowing targeted antibiotic therapy. However, sensitivity is only 50-70% — a negative Gram stain does NOT exclude bacterial infection. Gram-positive cocci in clusters suggest S. aureus; Gram-positive cocci in chains suggest Streptococcus; Gram-negative diplococci suggest N. gonorrhoeae.
Culture and sensitivity: The gold standard for identifying the organism and guiding antibiotic therapy. Sensitivity is 70-85% in untreated cases. Blood cultures should be sent simultaneously (positive in ~50-60% of cases). Culture MUST be set up before antibiotics are started.
Crystal analysis (under polarised light microscopy): monosodium urate (gout) — needle-shaped, negatively birefringent; calcium pyrophosphate (pseudogout) — rhomboid, weakly positively birefringent. Crystal arthropathy can coexist with septic arthritis ('pseudoseptic' presentation).
Synovial Fluid Analysis: Diagnostic Comparison
Applying Kocher Criteria and Risk Stratification
In children presenting with acute hip pain, the most critical clinical decision is distinguishing septic arthritis of the hip from transient synovitis (also called toxic synovitis) — the commonest cause of acute hip pain in children aged 3-10 years. Transient synovitis is a self-limiting inflammatory condition (likely post-viral) that mimics septic arthritis but does not require surgery. Correctly identifying which children need urgent surgical washout versus observation is a high-stakes diagnostic task.
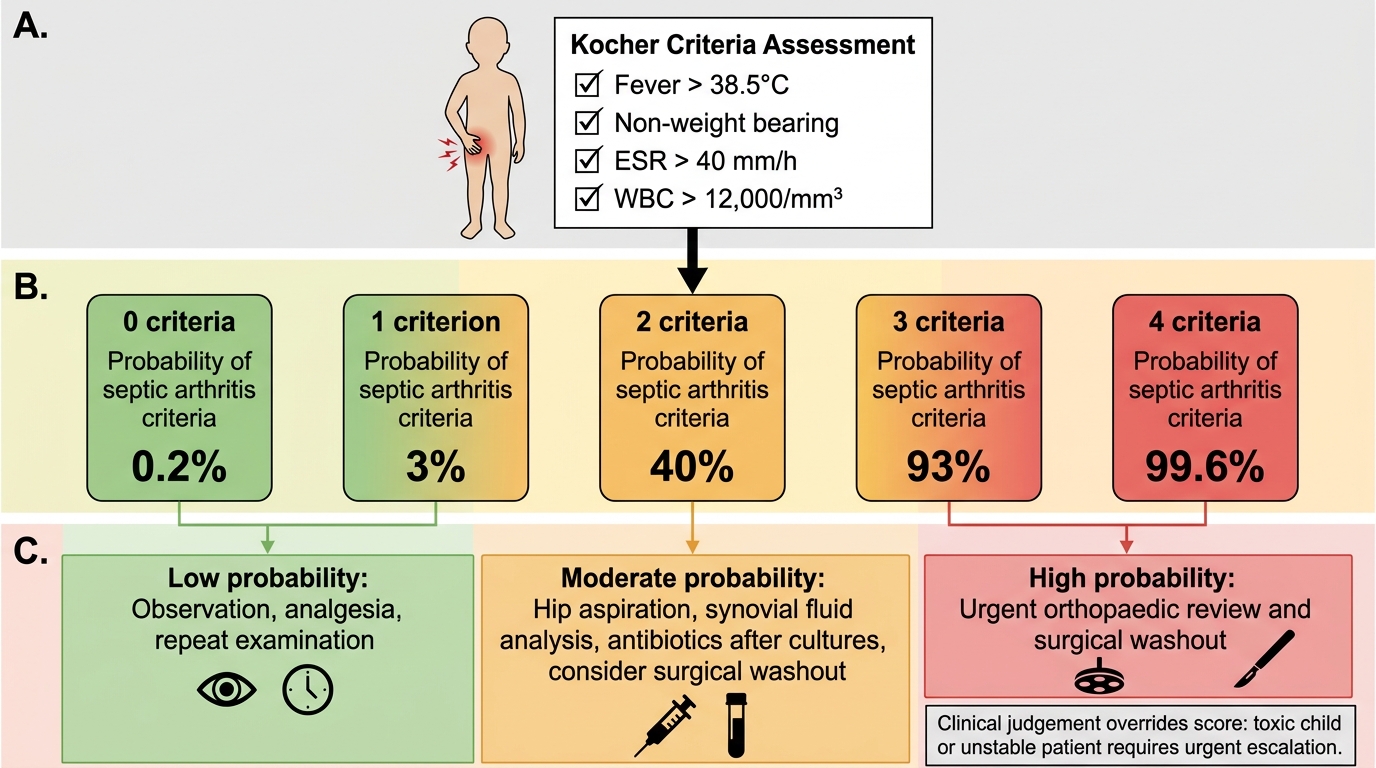
The Kocher criteria provide a validated, evidence-based risk stratification tool for this exact scenario. Originally derived by Kocher et al. (2004) from a large paediatric cohort and subsequently validated in multiple centres including Indian hospitals, these four clinical and laboratory parameters combine to generate a probability estimate that is both simple to calculate at the bedside and sufficiently accurate to inform high-stakes surgical decisions. Each criterion is binary — either present or absent — making the score immediately applicable without specialist equipment. The four predictors are:
1. Non-weight-bearing on the affected side
2. ESR >40 mm/h
3. Temperature >38.5°C
4. WBC >12,000/μL
The predicted probability of septic arthritis based on number of criteria present:
- 0 criteria: <0.2% probability
- 1 criterion: ~3%
- 2 criteria: ~40%
- 3 criteria: ~93%
- 4 criteria: >99%
The addition of a raised CRP (>20 mg/L) as a fifth predictor (Caird et al. modification) further improves specificity: 5 criteria = ~98% probability.
A probability >40% (≥2 Kocher criteria) is generally considered the threshold for proceeding to hip joint aspiration under ultrasound guidance and probable surgical washout. Children with 0-1 criteria and no fever may be observed with repeat examination at 24-48 hours.
Important caveat: the Kocher criteria were derived and validated in a specific population; clinical judgement must always be applied. A child who appears toxic and ill with all four criteria should go directly to surgical washout after aspiration confirms purulent fluid, without waiting for culture results.
Kocher Criteria Flowchart for Acute Pediatric Hip Pain
Supervised Practice: Team Role in Joint Aspiration
As a final-year student participating in joint aspiration under supervision, your role within the team is structured and graduated. You will rarely perform the aspiration independently at this stage, but you are expected to contribute meaningfully to every step of the procedure and to demonstrate competence in the preparatory and interpretive components.
Your supervised practice tasks are graded to match your level of training: observation and understanding come first, then assisted preparation, and finally active participation under direct supervision. Each task listed below represents a measurable competency that your supervising clinician can observe and sign off on a logbook or DOPS (Direct Observation of Procedural Skills) assessment card. The goal is not perfection on first attempt but systematic, safe progress — demonstrating that you know what you are doing, why each step matters, and what to do if something does not go as expected. Document each supervised opportunity in your logbook, noting the joint aspirated, your specific contribution, and any feedback received.
Your supervised practice tasks include:
Before the procedure:
- Take and present the relevant history and examination findings (including the Kocher criteria score for a paediatric hip case)
- Select the correct investigation tubes and label them before the procedure starts
- Describe the anatomical approach to be used and why it is safe
- Prepare the sterile field: open equipment onto the trolley without contaminating the sterile zone
During the procedure:
- Observe the operator's hand positioning, needle angulation, and aspiration technique
- Call out if aseptic technique is broken (e.g., if the operator's glove touches a non-sterile surface)
- Note the colour, turbidity, and volume of aspirated fluid
After the procedure:
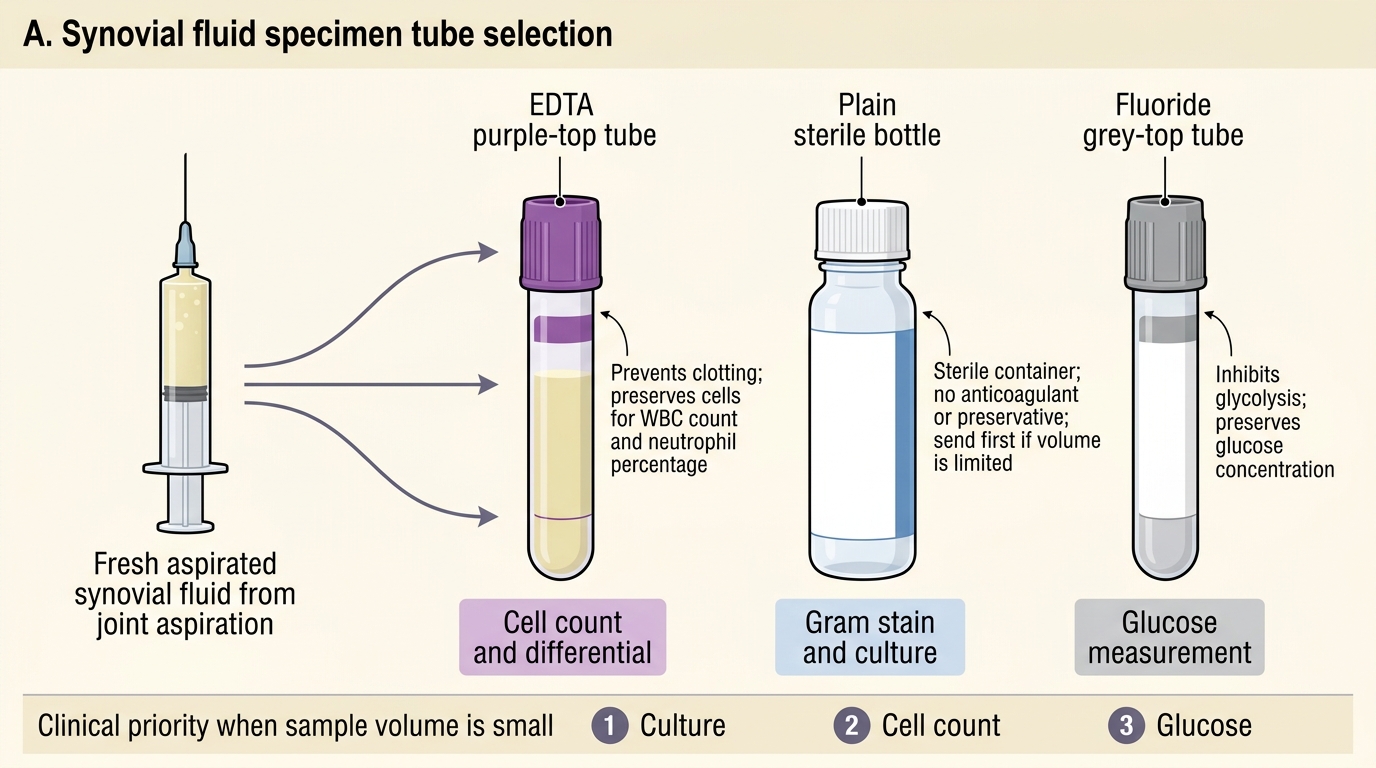
- Transfer fluid into the correct specimen tubes (EDTA for cell count, sterile bottle for culture, fluoride tube for glucose)
- Complete the request form with the clinical diagnosis, organism suspected, and antibiotics already given (the laboratory needs this to prioritise and interpret results)
- Monitor the patient for post-aspiration pain, swelling, or signs of vascular injury (haematoma)
- Interpret the preliminary cell count result and present it to the supervising clinician with a management recommendation
A common error at this stage is transferring the aspirate into the wrong tube: culture requires a plain sterile bottle (EDTA anticoagulant inhibits bacterial growth), and cell count requires EDTA (prevents clotting). Mixing up the tubes compromises both results.
Synovial Fluid Tube Selection
SELF-CHECK
A 5-year-old with acute left hip pain has 2 out of 4 Kocher criteria (fever 38.6°C and non-weight-bearing; ESR 35 mm/h; WBC 10,500). What is the predicted probability of septic arthritis and the recommended next step?
A. 0.2% probability — observe at home and review in one week
B. ~3% probability — discharge with NSAIDs and GP review
C. ~40% probability — arrange ultrasound-guided hip joint aspiration and admit for observation
D. ~93% probability — proceed immediately to emergency surgical washout without aspiration
Reveal Answer
Answer: C. ~40% probability — arrange ultrasound-guided hip joint aspiration and admit for observation
Two Kocher criteria yield approximately 40% predicted probability of septic arthritis — this crosses the threshold for aspiration. Ultrasound-guided aspiration is performed; if the fluid shows >50,000 WBC with neutrophilia, proceed to surgical washout. With 0-1 criteria, observation is appropriate. Four criteria (>99%) would warrant urgent theatre without waiting for aspiration results in most centres.