Page 12 of 18
OR3.3 | Operative Source Control Assistance — SDL Guide (Part 3)
Team-Assist Role: Theatre Participation and Responsibilities
As a final-year student scrubbing in for operative source control procedures, your role is defined within the surgical team hierarchy and the DOPS (Direct Observation of Procedural Skills) framework. You are a team-assist member — not the primary operator — but your participation is active, not passive. Understanding your responsibilities before you enter theatre ensures that you contribute positively to patient safety and procedural efficiency. The surgical team in orthopaedics typically comprises the primary surgeon, a registrar or senior resident, the scrub nurse, the anaesthetist, and the circulating nurse; your position as a student team-assist member is between the registrar and scrub nurse in terms of responsibility. Effective participation requires preparation: you should know the procedure, the anatomical approach, the structures at risk, and the expected sequence of steps before the incision is made.
Pre-operative responsibilities:
- Review the patient's imaging (X-ray, CT, MRI) and understand the planned procedure, the anatomical approach, and the structures at risk
- Confirm the consent form is signed and the correct limb/site is marked (WHO surgical safety checklist)
- Assist with positioning and padding of the patient (pressure point protection is a nurse and student responsibility in many theatres)
- Participate in the WHO time-out briefing — confirm patient name, procedure, site, allergies, and antibiotic prophylaxis administered
Intra-operative responsibilities:
- Retract tissues as instructed — use only the force indicated; excessive retraction injures nerves and vessels
- Pass instruments correctly — handle-first to the surgeon, named clearly (e.g., 'McIndoe scissors', 'Langenbeck retractor')
- Aspirate pus into the sterile pot for culture before any irrigation begins — if irrigation runs before sampling, the specimen is diluted and culture yield drops
- Monitor the instrument and swab count when called upon — this is a patient safety duty
- Irrigate the wound with saline when instructed — use a bulb syringe or pressurised system as directed, aiming the jet at the cavity wall, not at the surgeon
Post-operative responsibilities:
- Apply a sterile dressing to the wound under instruction
- Label and transport the operative specimen (bone biopsy, sequestrum, pus) to the laboratory immediately with the completed request form
- Complete the operative note under supervision (if asked) — this is a core clinical competency
- Monitor the patient in recovery for haemodynamic stability, limb perfusion, and drain output
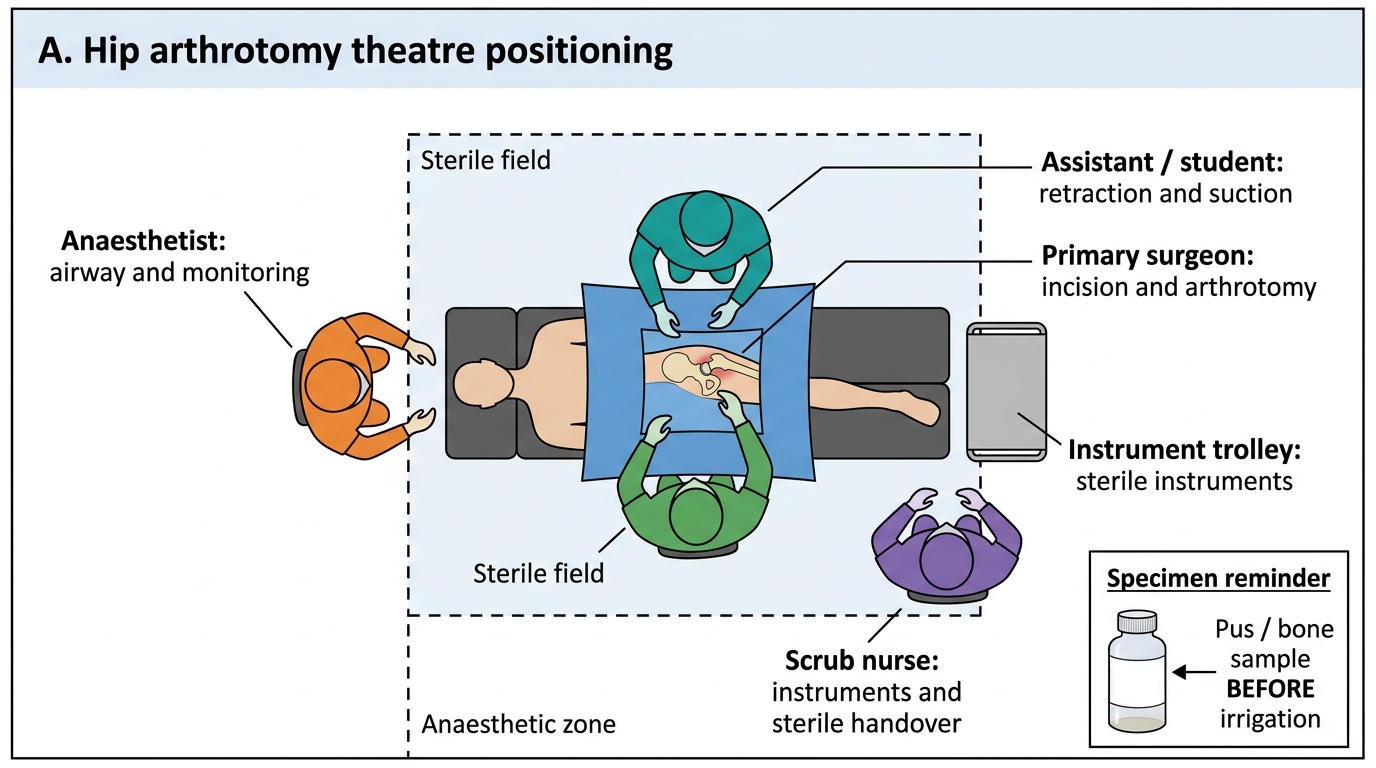
Hip Arthrotomy Theatre Positioning
SELF-CHECK
During a sequestrectomy, the scrub nurse asks you to prepare the pus sample for culture. The wound has just been irrigated. What should you have done, and what do you do now?
A. The irrigation does not matter — place the irrigated fluid into the culture bottle
B. The pus should have been aspirated into a sterile plain bottle BEFORE irrigation began; now collect a bone biopsy swab from the cavity wall as the best available alternative
C. Irrigation is always performed before sampling — this is correct theatre protocol
D. Culture is not required intraoperatively because blood cultures were already sent in the ward
Reveal Answer
Answer: B. The pus should have been aspirated into a sterile plain bottle BEFORE irrigation began; now collect a bone biopsy swab from the cavity wall as the best available alternative
The operative specimen (pus, bone biopsy) must be collected BEFORE irrigation because saline dilutes the bacterial load and dramatically reduces culture yield. If pus was not collected first, a bone biopsy from the cavity wall is the next best alternative — bone biopsy culture has higher yield than pus culture in chronic osteomyelitis because organisms are embedded in the bone matrix. This is a common team-assist error that the student must pre-empt by reminding the surgeon to sample before irrigation.
Post-operative Complications and Recognition
Operative source control procedures carry specific post-operative complications that the team-assist member must be able to recognise. Early identification and escalation of complications prevents permanent harm. The post-operative period is a critical window during which the benefits of surgery can be consolidated or lost: a haematoma that goes unrecognised for 12 hours may become secondarily infected; a neurovascular deficit not detected on the first post-operative check may progress to irreversible ischaemia; a drain occluded by fibrin in the first 24 hours may convert a draining wound into a re-accumulating pus collection. Your responsibility as a team-assist member extends into the post-operative ward — visiting the patient, examining the limb, reviewing the drain output, and escalating concerns promptly to the registrar or consultant.
The most important complications to recognise are grouped below by procedure and timing.
All procedures — early (24-72 hours):
- Wound haematoma: expanding swelling, firmness, and pain at the wound site; may compress a drain and occlude drainage. Requires return to theatre for evacuation if large.
- Neurovascular compromise: weakness, paraesthesia, pallor, or pulselessness in the distal limb. For hip procedures, assess hip flexion (femoral nerve) and foot dorsiflexion/eversion (sciatic/peroneal nerve). For tibial procedures, assess ankle dorsiflexion (anterior tibial nerve).
- Drain occlusion: drains become blocked with fibrin plugs within 24-48 hours. If drain output suddenly drops but the wound is swollen, suspect occlusion. Gentle milking of the drain may restore flow.
Sequestrectomy — late complications:
- Recurrence of infection: the most common late complication, usually due to incomplete sequestrum removal or inadequate dead-space management. Presents as recurrence of sinus tract discharge, pain, and rising inflammatory markers 4-12 weeks post-operatively.
- Fracture through the saucerised cavity: especially in the tibia, where a large cortical window weakens the bone structurally. Protective weight-bearing restrictions and sometimes external fixation are needed for 6-12 weeks.
- Wound non-healing: particularly in Type B (compromised) hosts — diabetics, immunosuppressed patients, elderly. Requires optimisation of the underlying comorbidity and sometimes a muscle flap or skin graft.
Arthrotomy — late complications:
- Joint stiffness (arthrofibrosis): adhesions forming if physiotherapy is delayed. Early passive movement is essential.
- Avascular necrosis of the femoral head (hip arthrotomy): the most feared complication, occurring if pressure on the lateral epiphyseal vessels is not relieved sufficiently early. Presents as hip pain, stiffness, and femoral head collapse on X-ray weeks to months later.
- Secondary osteoarthritis: cartilage damage from the initial infection and surgical trauma leads to progressive joint degeneration.
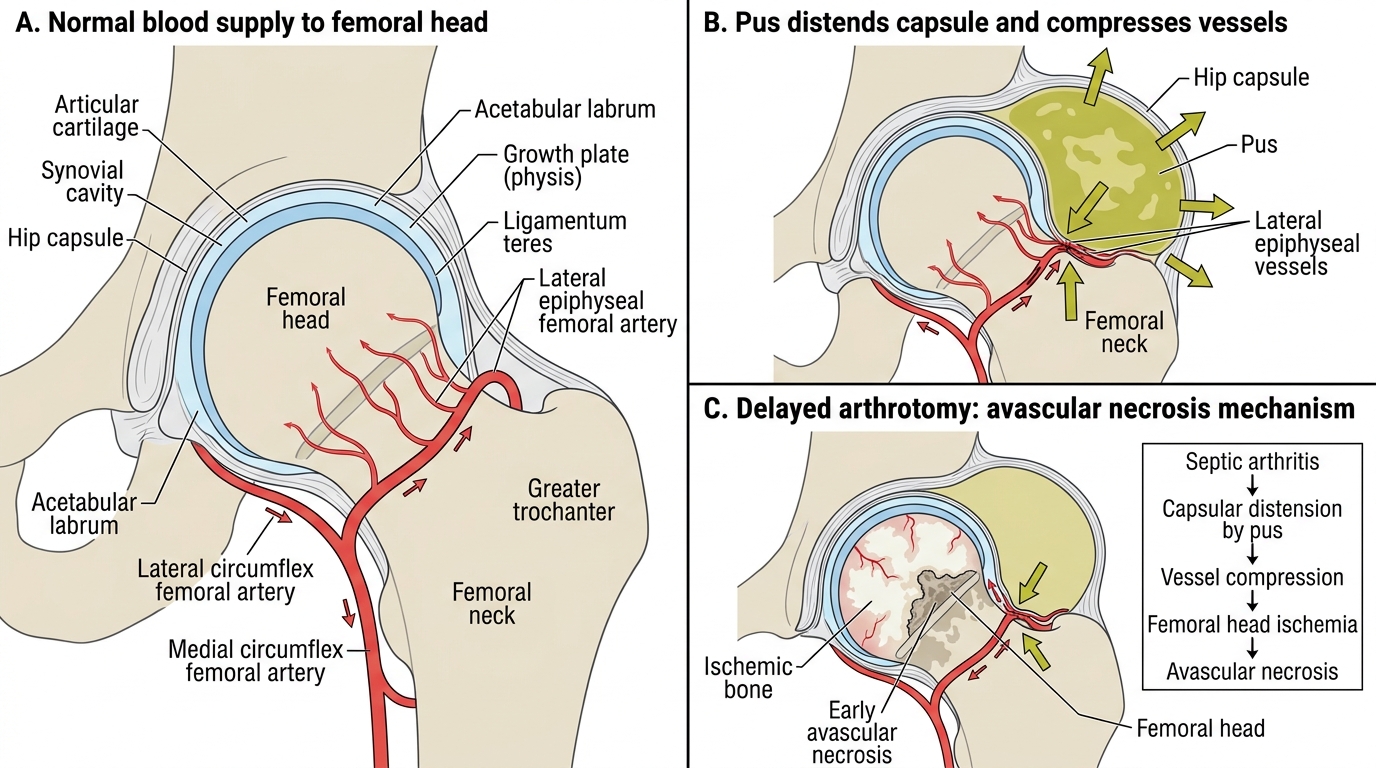
Hip Sepsis and Avascular Necrosis Mechanism
Self-Assessment: Theatre Readiness and Procedural Knowledge
Before your first supervised operative session, you should be able to answer every question below without reference to your notes. This self-assessment mirrors the standard questions a consultant or registrar will ask you at the scrub sink before allowing you to participate in the procedure. Working through these questions is also good preparation for OSCE and clinical examination stations on operative orthopaedics. Where you find a gap, re-read the relevant section of this module and the pre-operative briefing notes from your clinical placement. Aim to be able to explain the rationale for each step, not just recall the step itself — 'what' without 'why' is not clinical knowledge. A consultant watching you scrub in will test your understanding, not your memory alone.
Indications:
- Name three indications for arthrotomy in septic arthritis that cannot be managed by aspiration alone.
- What is the single most critical radiological finding that mandates sequestrectomy?
- Why is the hip the most urgent joint to drain in a child with septic arthritis?
Anatomy:
- What nerve is at risk during a proximal tibial approach for abscess drainage, and where does it lie?
- Describe the surgical interval for an anterior Smith-Petersen approach to the hip.
- What is the saucerisation — and why must the cavity walls be made of bleeding, vascular bone?
Procedure:
- Why must the operative specimen be collected BEFORE irrigation?
- What is dead-space management, and why does it matter after sequestrectomy?
- What does the team-assist member do during copious joint irrigation?
Complications:
- A patient 6 weeks after sequestrectomy develops a new discharging sinus. What is the most likely cause?
- A child develops inability to flex the hip and paraesthesia in the thigh on post-operative day 1 after hip arthrotomy. Which nerve is likely affected, and what is the immediate action?
Answer key: Three arthrotomy indications: hip septic arthritis, failure of aspiration within 24-36 h, loculated infection. Radiological finding for sequestrectomy: visible sequestrum on CT (dense avascular fragment). Most urgent hip drainage: avascular necrosis risk from raised intra-articular pressure on lateral epiphyseal vessels. Proximal tibial nerve at risk: common peroneal nerve wrapping around the fibular neck, lies at the posterolateral aspect. Smith-Petersen interval: between sartorius/rectus femoris (femoral nerve) and tensor fasciae latae (superior gluteal nerve). Saucerised cavity walls of vascular bone: support granulation tissue ingrowth — avascular sclerotic walls prevent healing. Specimen before irrigation: dilution reduces bacterial count and culture yield. Dead-space: cavity left by removed sequestrum, managed with bone graft or antibiotic beads to prevent haematoma and reinfection. Team assist during irrigation: aims saline jet at wound walls, avoids surgeon's field, adjusts suction. New sinus at 6 weeks: incomplete sequestrum removal (residual avascular bone). Hip flexion + thigh paraesthesia post-op: femoral nerve injury — call senior immediately, assess distal neurology, check retractor position on review.
CLINICAL PEARL
Sample before you irrigate — this is the single most important operative habit to internalise. The intraoperative culture of pus or bone biopsy is the most reliable specimen for identifying the causative organism in chronic osteomyelitis, far superior to sinus-tract swabs (which grow colonising organisms rather than the true pathogen in >50% of cases). The moment the cavity is opened, the first action is to aspirate or swab a sample and hand it to the scrub nurse for immediate placement in a sterile plain pot. If you irrigate first, you dilute the bacterial count and may convert a culture-positive specimen to a false-negative, leaving the patient on empirical antibiotics for weeks without a targeted regimen.