Page 1 of 10
OR5.1 | Inflammatory Polyarthritis Clinical Approach — SDL Guide
Learning Objectives
- Distinguish inflammatory from degenerative arthritis using clinical and laboratory criteria
- Outline the pathogenesis of rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis
- Describe the characteristic clinical features and radiological signs of each inflammatory arthropathy
- Explain the principle and rational selection of disease-modifying antirheumatic drugs (DMARDs)
- Construct a systematic approach to a patient presenting with polyarthritis
INSTRUCTIONS
Inflammatory polyarthritis accounts for a significant proportion of orthopaedic and general medicine consultations in India. Misclassifying an inflammatory arthropathy as osteoarthritis delays disease-modifying treatment and leads to irreversible joint destruction. This module equips you with a structured clinical framework to differentiate the major inflammatory joint diseases — rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis — and to initiate appropriate investigation and management at the district hospital level.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch 25 (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch 4 (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed., Ch 31–33 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 34-year-old female teacher presents with a 6-month history of bilateral hand stiffness that is worst in the morning and eases after about an hour of activity. She has noticed progressive swelling of the proximal interphalangeal (PIP) and metacarpophalangeal (MCP) joints of both hands and is no longer able to make a full fist. She is increasingly fatigued, has lost 3 kg, and her ESR is 68 mm/h. Her 65-year-old neighbour has a similar complaint and was told it is 'joint wear and tear.' Are these the same condition? How you answer this question will determine whether this woman's joints are saved or destroyed.
WHY THIS MATTERS
Inflammatory arthritides — particularly rheumatoid arthritis (RA), ankylosing spondylitis (AS), and psoriatic arthritis (PsA) — are collectively the leading cause of preventable musculoskeletal disability in working-age adults. Unlike osteoarthritis, where cartilage wears mechanically, inflammatory arthritis is driven by an immune-mediated process that can be arrested with disease-modifying drugs if diagnosed early. A delay of even six months from symptom onset to DMARD initiation significantly worsens the radiographic outcome. As an MBBS graduate you must be able to recognise these conditions, order the right investigations, and initiate or expedite specialist referral. In resource-limited settings, accurate clinical diagnosis — without waiting for expensive serology — saves joints and livelihoods.
RECALL
Before you proceed, recall these foundations: (1) Joints have three main tissues targeted in arthritis — synovium (lines joints), articular cartilage, and subchondral bone. (2) The cytokines TNF-α, IL-1, and IL-6 drive synovial inflammation. (3) HLA (Human Leukocyte Antigen) alleles encode immune recognition proteins on chromosome 6 — HLA-DR4 and HLA-DR1 are linked to RA risk; HLA-B27 to seronegative spondyloarthropathies. (4) The ESR and CRP are acute-phase reactants that rise with active inflammation. (5) Recall the basic anatomy: the spine has facet joints (zygapophyseal), costovertebral joints, and the sacroiliac joint — all are synovial and can be inflamed in spondyloarthropathies.
Inflammatory versus Degenerative Arthritis: The Diagnostic Pivot
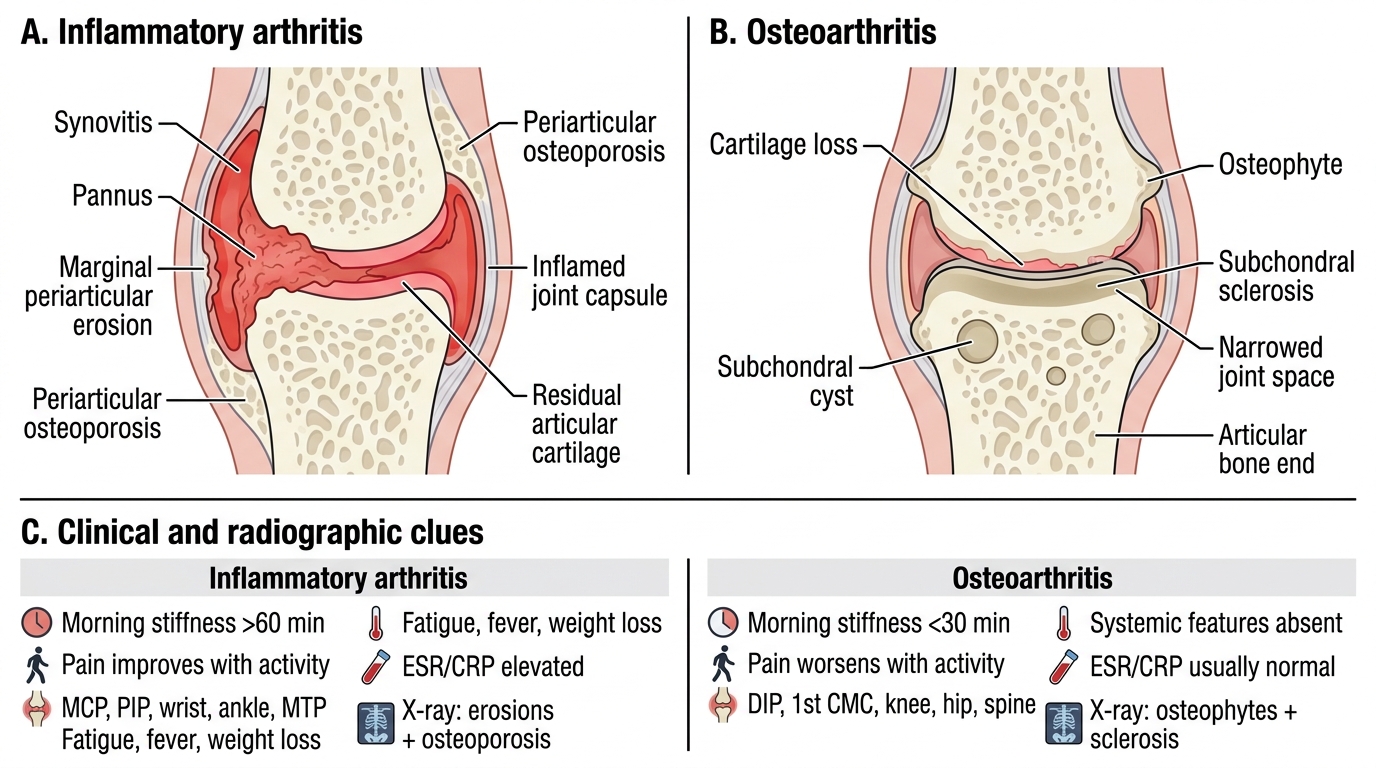
The first and most important clinical step in any patient presenting with joint pain is to determine whether the process is inflammatory or degenerative (mechanical). This single determination routes the entire subsequent workup and treatment strategy, and failure to make it is the most common diagnostic error in arthritis care. Inflammatory arthritis is characterised by synovitis — the synovial lining becomes hyperaemic, hypertrophied, and infiltrated with immune cells, producing excess synovial fluid that is rich in cytokines. Degenerative arthritis (osteoarthritis) is characterised by cartilage loss, subchondral bone sclerosis, and osteophyte formation with relatively little synovial reaction.
The key discriminating features are systematically captured in the table below, but the two most important at the bedside are morning stiffness duration and the pattern of joint involvement. Inflammatory morning stiffness lasts longer than 60 minutes (often 1–3 hours) because the synovial fluid 'gels' overnight in the inflamed joint and requires active movement to loosen; degenerative morning stiffness typically clears in under 30 minutes ('gelling' or 'start-up pain'). Pain that improves with activity strongly favours inflammation, whereas pain that worsens with sustained activity favours degeneration.
Pattern of joint involvement provides a parallel diagnostic signal. Inflammatory polyarthritis classically affects the small joints of the hands (MCPs, PIPs) and feet symmetrically, often sparing the distal interphalangeal (DIP) joints in RA. Osteoarthritis preferentially affects the DIP joints (Heberden's nodes), the carpometacarpal joint of the thumb, weight-bearing joints (knee, hip), and the spine — largely sparing the MCPs. The wrist, elbow, shoulder, and ankle are rarely affected in primary OA but are often involved in RA.
Systemic features — fatigue, weight loss, low-grade fever, anaemia of chronic disease — occur in inflammatory arthritis and are absent in uncomplicated OA. Laboratory findings in inflammatory arthritis include elevated ESR (>20 mm/h women, >15 mm/h men), elevated CRP, normocytic normochromic anaemia, and thrombocytosis. Radiological features of inflammation (periarticular osteoporosis, soft-tissue swelling, erosions) are quite different from OA changes (joint space narrowing, osteophytes, sclerosis, subchondral cysts).
Inflammatory Arthritis vs Osteoarthritis
| Feature | Inflammatory Arthritis | Osteoarthritis |
|---|---|---|
| Morning stiffness | >60 min | <30 min |
| Pain with activity | Improves | Worsens |
| Joints involved | MCP, PIP, wrist, ankle, MTP | DIP, CMC thumb, knee, hip, spine |
| Systemic features | Fatigue, fever, weight loss | Absent |
| ESR/CRP | Elevated | Usually normal |
| X-ray pattern | Erosions, osteoporosis | Osteophytes, sclerosis |
Approach to a Patient with Polyarthritis: Systematic Framework
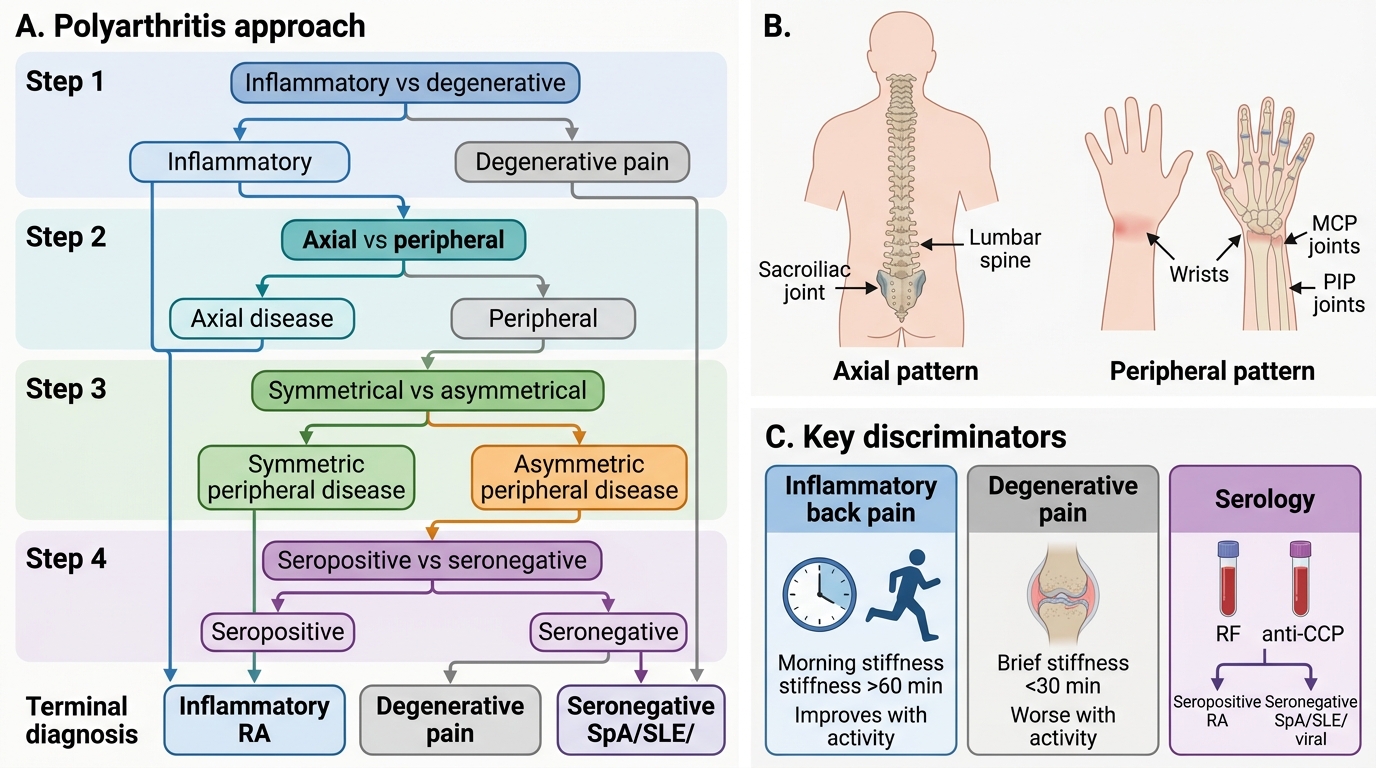
A structured approach converts a complex presentation into a manageable differential. Polyarthritis is defined as simultaneous involvement of five or more joints (oligoarthritis = 2–4 joints; monoarthritis = 1 joint). The history and examination systematically narrow the differential along several axes that together point strongly toward a diagnosis even before serology returns.
Begin with the temporal pattern: acute (<6 weeks) polyarthritis raises the differential of reactive arthritis, viral arthritis (parvovirus B19, hepatitis B, rubella), acute rheumatic fever, and gout flares. Chronic (>6 weeks) polyarthritis narrows to RA, seronegative spondyloarthropathies, psoriatic arthritis, and connective tissue diseases. A migratory pattern (one joint becomes inflamed then settles before the next flares) is typical of acute rheumatic fever and gonococcal arthritis. An additive pattern (each new joint remains inflamed as more are added) is typical of RA.
Next, determine axial versus peripheral predominance. If the spine (especially the lower back and sacroiliac region), hips, and shoulders are the primary sites with peripheral joints involved secondarily, a spondyloarthropathy is likely — this group includes AS, PsA (axial type), reactive arthritis, and enteropathic arthritis. Predominantly peripheral small-joint disease, particularly in a symmetrical MCP/PIP distribution, points toward RA.
Then assess extra-articular features: skin (psoriasis plaques for PsA; malar rash for SLE), eyes (uveitis/iritis in AS and PsA; conjunctivitis in reactive arthritis), genitourinary history (urethritis in reactive arthritis), nail changes (pitting, onycholysis in PsA), and nodules (rheumatoid nodules over the olecranon in seropositive RA). Classifying the arthritis as symmetrical versus asymmetrical, and as seropositive versus seronegative, then points firmly at a diagnosis.
Clinical Approach to Polyarthritis
SELF-CHECK
A 28-year-old man presents with 4 months of lower back pain and stiffness that is worst on waking and improves with exercise. He has no history of trauma. Which feature most strongly differentiates this from mechanical low back pain?
A. Pain radiating to the leg
B. Improvement of stiffness with activity and duration greater than 60 minutes
C. Night pain that awakens the patient
D. Paravertebral muscle spasm
Reveal Answer
Answer: B. Improvement of stiffness with activity and duration greater than 60 minutes
Inflammatory back pain — the hallmark of spondyloarthropathies including ankylosing spondylitis — characteristically improves with activity and causes prolonged morning stiffness exceeding 60 minutes. This is the opposite of mechanical back pain, which worsens with activity and eases with rest. Radiation to the leg, night pain, and paraspinal spasm can occur in either mechanical or inflammatory disease.
Rheumatoid Arthritis: Pathogenesis and Tissue Lesions
Rheumatoid arthritis (RA) is a systemic, chronic, autoimmune inflammatory disease whose primary target is the synovial joint. It affects approximately 0.5–1% of adults worldwide, with a female-to-male ratio of 3:1 and peak onset in the fourth and fifth decades. Understanding the pathogenesis clarifies why DMARDs — which target immune mediators — are effective, whereas analgesics and NSAIDs are not disease-modifying.
The central lesion of RA is synovitis progressing to pannus formation. The process begins when CD4+ T-helper cells are activated against self-antigens — principally citrullinated peptides — in genetically susceptible individuals carrying HLA-DR4 or HLA-DR1. Cigarette smoking, which generates citrullinated proteins in lung tissue, is the dominant environmental trigger. Activated T cells recruit macrophages and B cells; macrophages release TNF-α, IL-1, and IL-6, which drive a sustained inflammatory cascade. B cells produce the characteristic autoantibodies — rheumatoid factor (RF), an IgM anti-IgG antibody, and anti-cyclic citrullinated peptide antibody (anti-CCP) — which form immune complexes that perpetuate synovial inflammation.
This sustained synovitis produces pannus — a sheet of proliferating synovial fibroblasts and inflammatory cells that overhangs and erodes the articular cartilage and subchondral bone at the 'bare area' (the uncovered bone at the cartilage–synovium junction). Proteolytic enzymes (matrix metalloproteinases, cathepsins) secreted by pannus cells digest collagen irreversibly. Simultaneously, RANKL expressed by synoviocytes activates osteoclasts, producing juxta-articular erosions and periarticular osteoporosis visible on plain X-ray. Over years, cartilage destruction, ligament and tendon damage, and capsular fibrosis produce the classic deformities: ulnar deviation at the MCPs, Boutonnière deformity (PIP flexion + DIP hyperextension from central slip rupture), and swan-neck deformity (PIP hyperextension + DIP flexion from volar plate laxity).
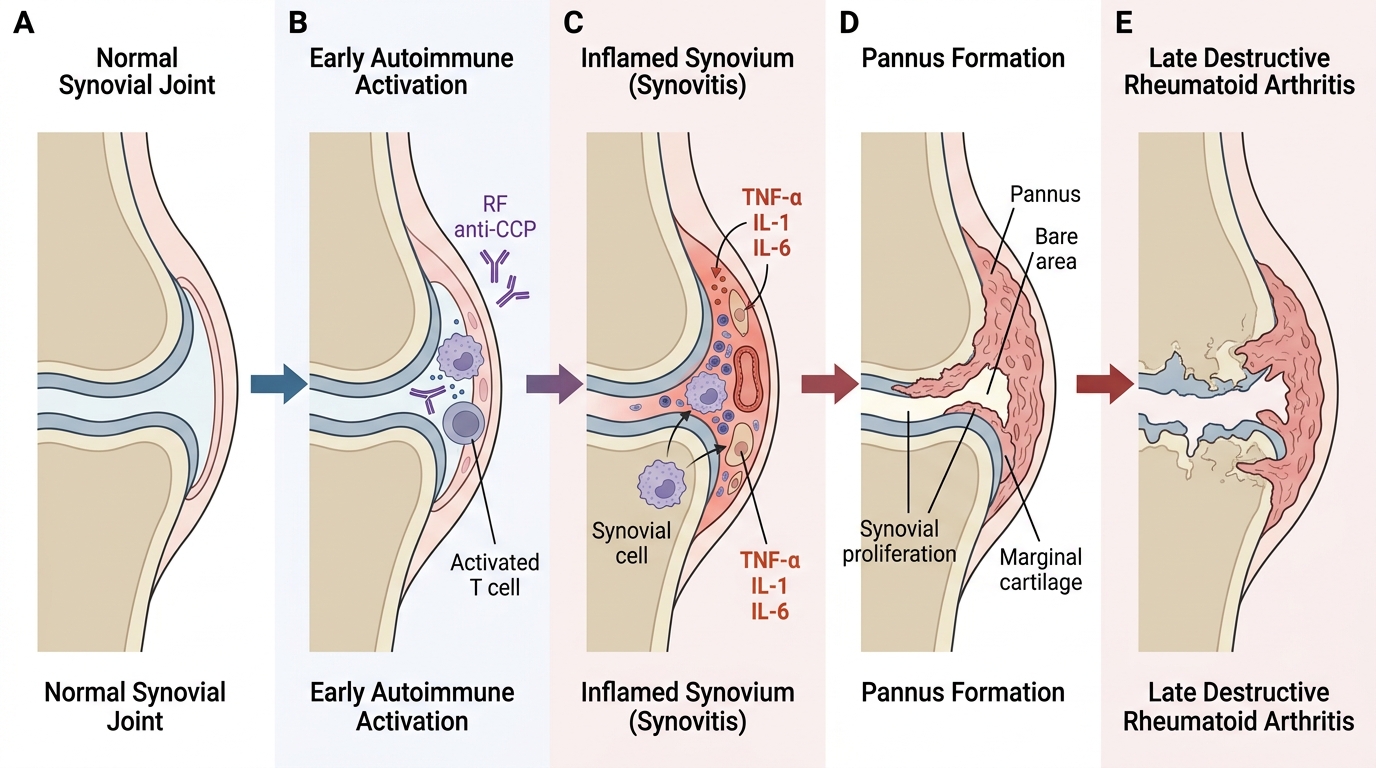
Pathogenesis Sequence of Rheumatoid Arthritis