Page 4 of 10
OR5.1 | Inflammatory Polyarthritis Clinical Approach — SDL Guide (Part 4)
Non-Pharmacological Management, Monitoring, and Specialist Referral
Inflammatory arthritis management extends beyond pharmacology. Immediate initial management at the district hospital level includes: confirming the clinical diagnosis, starting an NSAID for symptom relief while the workup is completed, referring promptly to a rheumatologist, and counselling the patient that this is a chronic but treatable condition requiring long-term monitoring. A delay in DMARD initiation beyond three months from diagnosis worsens the radiographic outcome in RA.
For acute flares of established RA, intra-articular corticosteroid injection (methylprednisolone acetate or triamcinolone acetonide) into an acutely inflamed joint provides rapid, localised relief. Short courses of oral prednisolone (0.5 mg/kg/day for 1–2 weeks, rapidly tapered) are used as 'bridge therapy' while waiting for DMARDs to take effect. Corticosteroids are NOT long-term management for RA — prolonged use causes osteoporosis, diabetes, hypertension, and adrenal suppression.
Physiotherapy is particularly critical in AS: the spine tends to fuse, and fusion in a flexed 'question mark' posture is permanently disabling, whereas fusion in near-neutral extension (achieved by daily prone-lying, spinal extension exercises, and swimming) preserves function. Chest expansion exercises maintain respiratory reserve. Joint protection and occupational therapy preserve hand function in RA. Surgical management is reserved for structural failure: synovectomy (rarely used now with biologics), total joint replacement arthroplasty (end-stage RA hip or knee destruction), arthrodesis (wrist or ankle fusion for painful destroyed joints), and cervical spine fusion for atlantoaxial subluxation threatening the spinal cord.
Monitoring for methotrexate: monthly FBC + LFTs for the first 3–6 months, then 3-monthly. Hydroxychloroquine: annual ophthalmological review for macular toxicity. Biologic DMARDs: pre-treatment TB screening + 3-monthly clinical review.
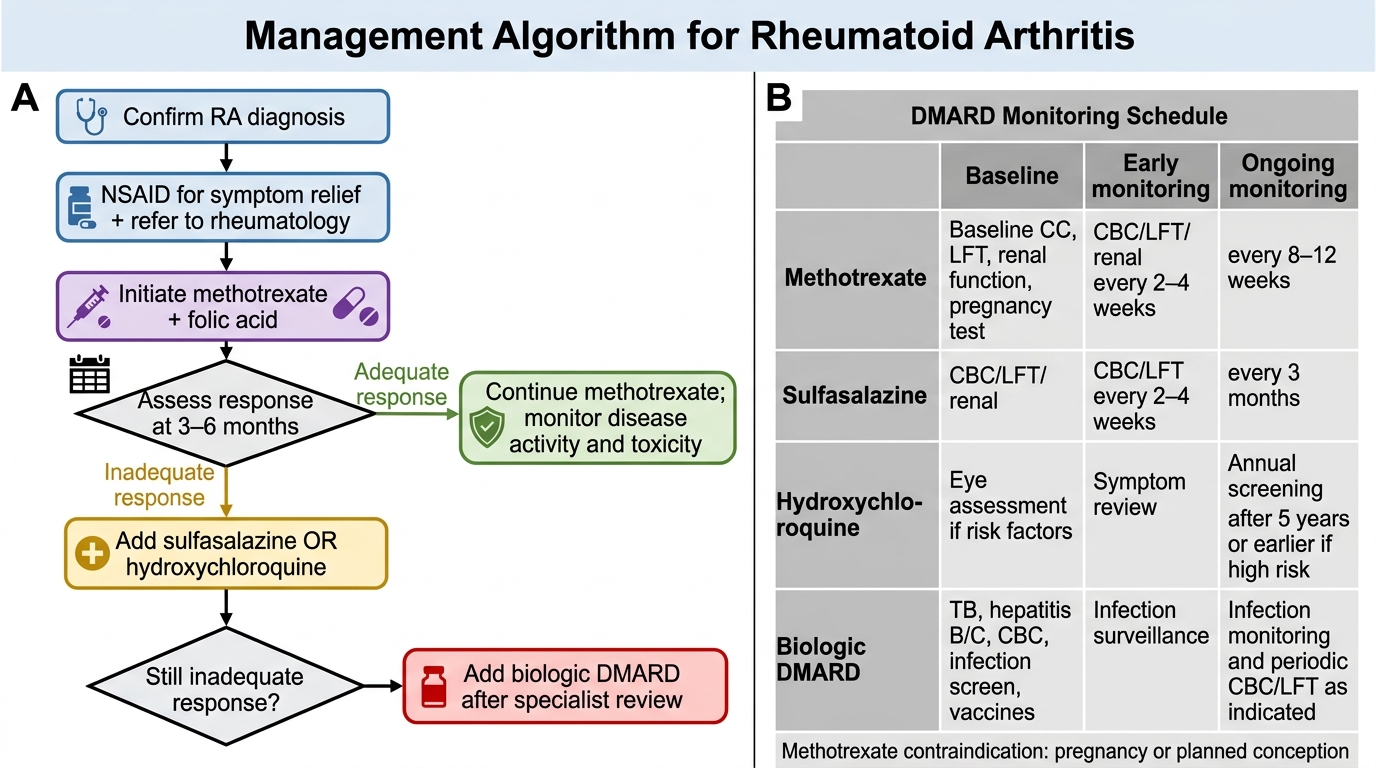
Rheumatoid Arthritis Management Algorithm and DMARD Monitoring
SELF-CHECK
A 30-year-old woman with rheumatoid arthritis is about to start methotrexate therapy. Which is an absolute contraindication to its use?
A. Mild elevation of serum creatinine (1.2 mg/dL)
B. Known pregnancy or planned conception within 3 months
C. Anaemia of chronic disease with haemoglobin 10.5 g/dL
D. HLA-DR4 positive serology
Reveal Answer
Answer: B. Known pregnancy or planned conception within 3 months
Methotrexate is absolutely contraindicated in pregnancy — it is a potent folate antagonist that causes neural tube defects, fetal death, and teratogenicity. Women of childbearing age must use effective contraception during therapy and for at least 3 months after stopping. Mild renal impairment requires dose reduction rather than absolute contraindication. Anaemia of chronic disease and HLA-DR4 status are not contraindications.
Comparison and Diagnostic Synthesis of the Three Arthropathies
Provided image
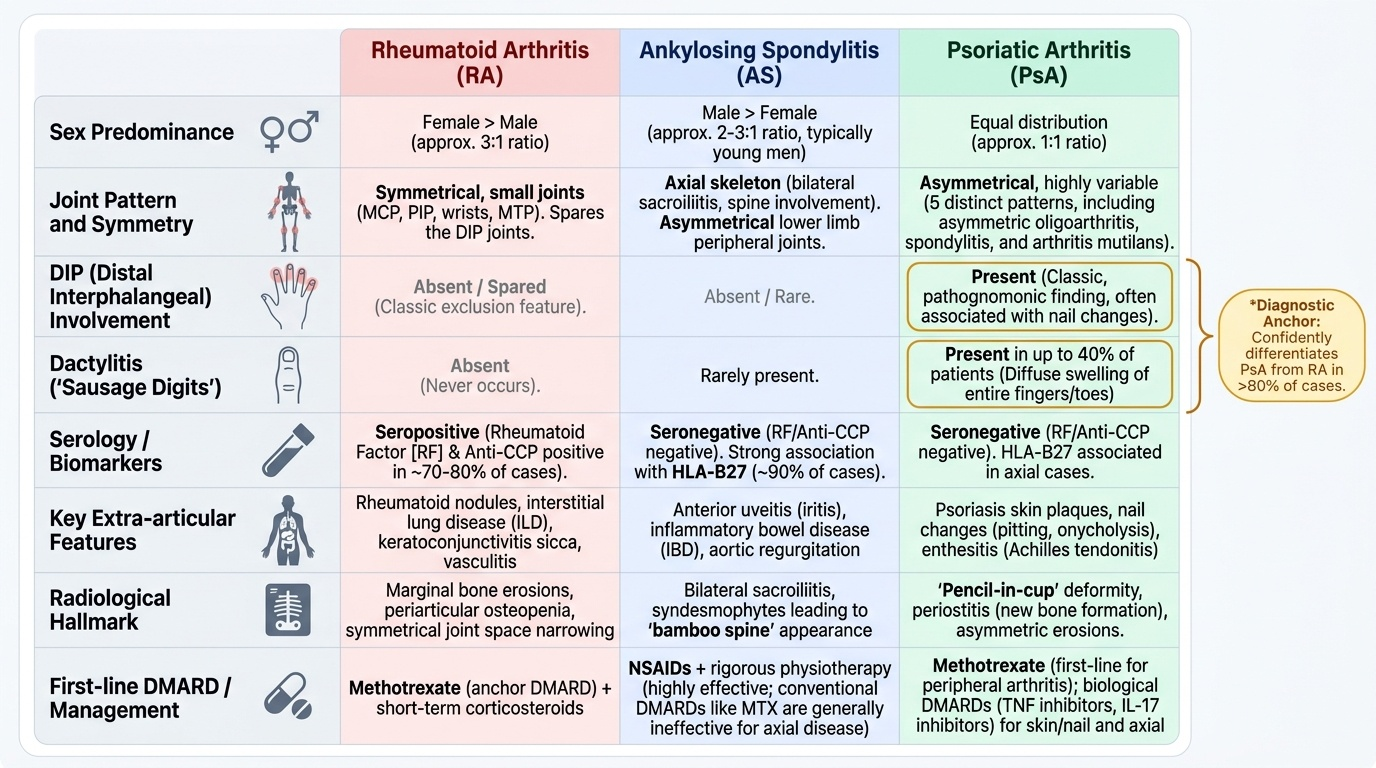
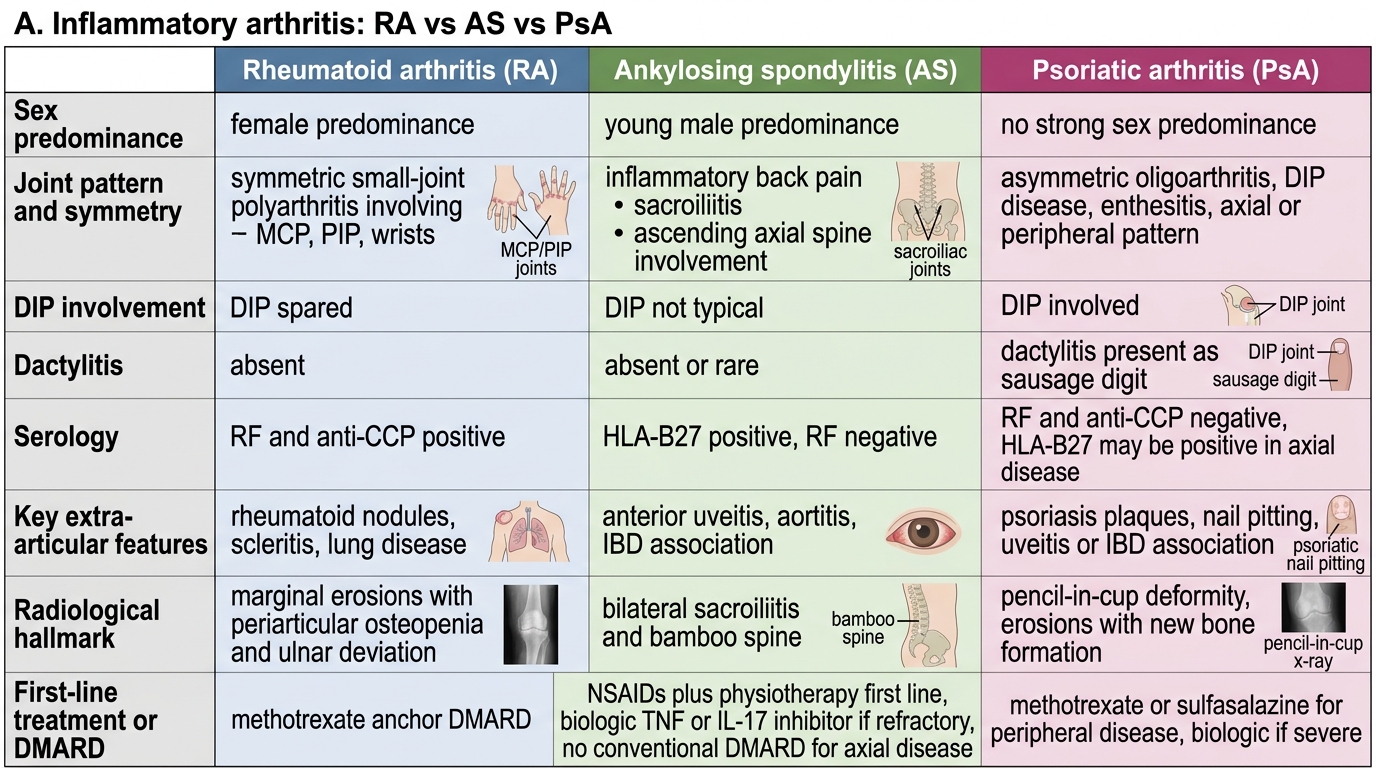
The ability to rapidly differentiate RA, AS, and PsA at the bedside is the practical skill this module builds toward. While each has a distinct pathogenesis and phenotype, differentiation is clinically achievable in most cases from history and examination alone, with serology and imaging confirming the diagnosis.
The comparative framework below integrates the pathogenesis, clinical features, radiological findings, and management into a single diagnostic reference. The three anchor comparisons are: (1) RA affects small joints symmetrically, spares DIPs, is seropositive (RF/anti-CCP), and methotrexate is its anchor DMARD. (2) AS affects the sacroiliac joints and spine in young men, is HLA-B27 positive and RF-negative, produces the bamboo spine, and requires NSAIDs + physiotherapy as the first-line response. (3) PsA is seronegative, associated with psoriasis, has five joint patterns including pathognomonic DIP involvement and dactylitis, and shows the pencil-in-cup X-ray deformity. The two features that are unique to PsA and never occur in RA are DIP arthritis and dactylitis — knowing these two anchors allows confident differentiation in over 80% of cases.
RA vs AS vs PsA Comparison
| Feature | RA | AS | PsA |
|---|---|---|---|
| Sex ratio | F:M = 3:1 | M:F = 3:1 | Equal |
| Joint pattern | Symmetric MCP/PIP/wrist | Sacroiliac + spine | Asymmetric; 5 patterns |
| DIP involvement | Never | Rare | Yes (pathognomonic) |
| Dactylitis | No | No | Yes |
| Serology | RF+/anti-CCP+ (~70%) | Seroneg; HLA-B27+ (~90%) | Seroneg; HLA-B27+ (axial) |
| Key extra-articular | Nodules, ILD | Uveitis, AR | Psoriasis, nail changes |
| X-ray hallmark | Erosions + periarticular osteoporosis | Bamboo spine + sacroiliitis | Pencil-in-cup + DIP erosions |
| First-line DMARD | Methotrexate | NSAIDs + physiotherapy | Methotrexate / IL-17i |
CLINICAL PEARL
Three pattern rules that save joints: (1) If a young woman's morning stiffness lasts more than one hour and her MCPs are boggy — not bony — think RA and check RF + anti-CCP without delay; anti-CCP positive predicts erosive disease requiring early aggressive DMARD therapy. (2) If a young man's back pain improves with exercise, starts before age 40, lasts more than 3 months, and wakes him at night — think AS and image the sacroiliac joints; do not dismiss it as muscle strain. (3) If a patient with psoriasis develops asymmetric joint pain and a sausage digit — think PsA; nail pitting is a clinical sign, not a cosmetic finding. In all three conditions, the window for effective DMARD treatment is early — the joint is always easier to save than to replace.