Page 7 of 13
OR9.1 | Cerebral Palsy Orthopaedic Assessment — SDL Guide (Part 3)
Self-Assessment: Key Principles in Cerebral Palsy
Consolidating your understanding of CP requires active retrieval, not passive review. Research in cognitive science consistently demonstrates that attempting to recall information — even imperfectly — produces more durable, transferable learning than re-reading the same material. Use this section as a deliberate closed-book exercise: cover the preceding content, formulate a complete answer from memory, and then return to the relevant section to verify and fill gaps. CP is a condition where examiners routinely test three themes simultaneously — classification, systematic assessment, and the intervention hierarchy — because these three dimensions are inseparable in clinical practice. A student who can classify CP but cannot map classification to management, or who knows botulinum toxin exists but cannot state its prerequisites and limitations, will underperform in viva and clinical examinations. Practise weaving all three themes into every answer.
The following questions are arranged from foundational classification through to applied surgical decision-making:
- Classification vignette: A premature infant (28 weeks) develops bilateral lower-limb spasticity with minimal arm involvement, GMFCS level II at age 4. What type and distribution of CP is this? What is the underlying brain pathology and why does it preferentially affect the legs?
- UMN vs LMN distinction: A 6-year-old has equinus foot, brisk knee jerks, and an upgoing plantar response. A second child has equinus foot, absent knee jerks, and a flexor plantar response. Identify the diagnosis in each, explain the mechanism of equinus in each, and state how management differs.
- Spasticity management: A 5-year-old diplegic child has dynamic equinus (gastrocnemius spasticity MAS 2, full passive dorsiflexion at rest, positive Silfverskiöld test). What is the first-line spasticity intervention, and what combined treatment maximises its effect? When would you escalate to surgery?
- Hip surveillance: At what migration percentage (Reimers index) does a CP hip require surgical intervention? A non-ambulatory 10-year-old with quadriplegic CP has a migration percentage of 70% — what are the surgical options?
- SEMLS rationale: Why is single-event multilevel surgery preferred over sequential staged operations in an ambulatory diplegic child requiring femoral derotation, hamstring lengthening, and Achilles lengthening?
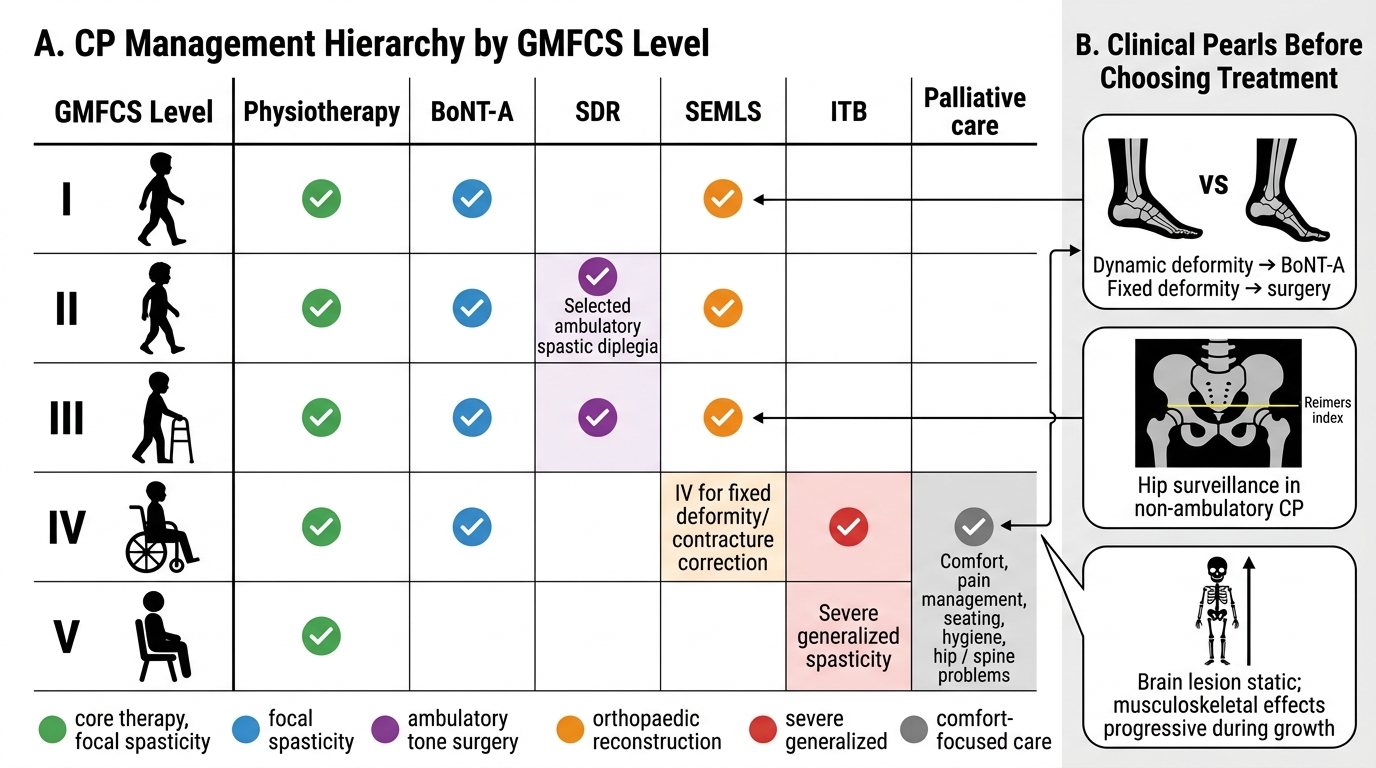
Cerebral Palsy Management Hierarchy by GMFCS Level
CLINICAL PEARL
Three rules for CP assessment: (1) Always distinguish DYNAMIC from FIXED deformity before planning treatment — botulinum toxin works for dynamic, surgery is needed for fixed. (2) Perform hip surveillance X-rays (AP pelvis, Reimers index) at every clinic visit for non-ambulatory CP — hip dislocation is silent until it causes pain, and correction becomes much harder after complete dislocation. (3) Never describe CP as 'static' to families without qualification — the brain lesion is static, but the musculoskeletal consequences are progressive throughout growth. Families and students who hear 'static' often misunderstand this to mean 'nothing will change or worsen' — which is clinically dangerous and leads to missed intervention windows.