Page 1 of 13
OR8.1 | Post-polio Residual Paralysis — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis and natural history of poliomyelitis leading to post-polio residual paralysis (PPRP)
- Identify the clinical stages of polio (acute, convalescent, residual) and enumerate the characteristic LMN findings in PPRP
- Assess deformities arising from muscle imbalance in PPRP using appropriate clinical and functional evaluation tools
- Explain the principles of management of PPRP including orthotic devices, physiotherapy, tendon transfers, and arthrodesis
- Distinguish post-polio residual paralysis (LMN flaccid pattern) from upper motor neurone conditions such as cerebral palsy
INSTRUCTIONS
Despite near-elimination through immunisation, post-polio residual paralysis (PPRP) remains a significant cause of preventable disability in India. Thousands of children and adults live with limb deformities resulting from asymmetric muscle paralysis. As a final-year student you will encounter patients with old polio in outpatient clinics, disability assessment centres, and surgical wards. Understanding the LMN pathophysiology, recognising the deformity patterns, and knowing the hierarchy of interventions — from orthoses to tendon transfers to arthrodesis — is essential for planning rehabilitation and surgery in resource-limited settings.
References
- Maheshwari's Essential Orthopaedics, Ch on Neuromuscular Disorders (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Ch on Paralytic Disorders (textbook)
- Ebnezar's Textbook of Orthopaedics, Ch on Poliomyelitis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 14-year-old boy from rural Maharashtra is brought to your outpatient clinic by his parents. He contracted a febrile illness at age 2 and was left with a limp. On examination, his left lower limb is thinner than the right; he walks with an equinovarus deformity and uses a stick. He cannot stand on his left heel. His knee jerks are absent on the left side. His parents ask if he can have surgery to walk better before he starts secondary school. How do you assess the deformity systematically, and what sequence of interventions will you offer?
WHY THIS MATTERS
India carries one of the world's largest burdens of post-polio disability despite the Pulse Polio Programme. Millions of Indians live with PPRP-related deformities — equinus, equinovalgus, genu recurvatum, flail hip, paralytic scoliosis — most of which are correctable or compensatable if managed in a structured, stepwise manner. At district and taluk hospitals, the orthopaedic surgeon is often the first and only specialist these patients ever see. Knowing the surgical hierarchy (orthoses first, soft-tissue procedures next, bony stabilisation last), the prerequisites for tendon transfer (donor grade ≥4, supple joint, neurological stability), and when to refer to a higher centre directly determines patient outcomes. This SDL also reinforces the fundamental distinction between LMN flaccid paralysis (polio) and UMN spastic paralysis (cerebral palsy) — a distinction that changes every aspect of management.
RECALL
Before proceeding, recall the following from your basic sciences: (1) The anatomy of the anterior horn cell (lower motor neurone) and the clinical difference between LMN and UMN lesions — LMN damage causes flaccid paralysis with wasting and absent reflexes, while UMN damage causes spastic paralysis with exaggerated reflexes. (2) The Medical Research Council (MRC) grading of muscle power (0–5). (3) The concept of agonist–antagonist balance across a joint and how selective paralysis of one group causes progressive deformity. (4) Basic gait phases (stance: heel strike → foot flat → mid-stance → heel rise → toe-off; swing: acceleration → mid-swing → deceleration) and how weakness at specific phases produces characteristic gait deviations.
Clinical Presentation and Stages of Poliomyelitis
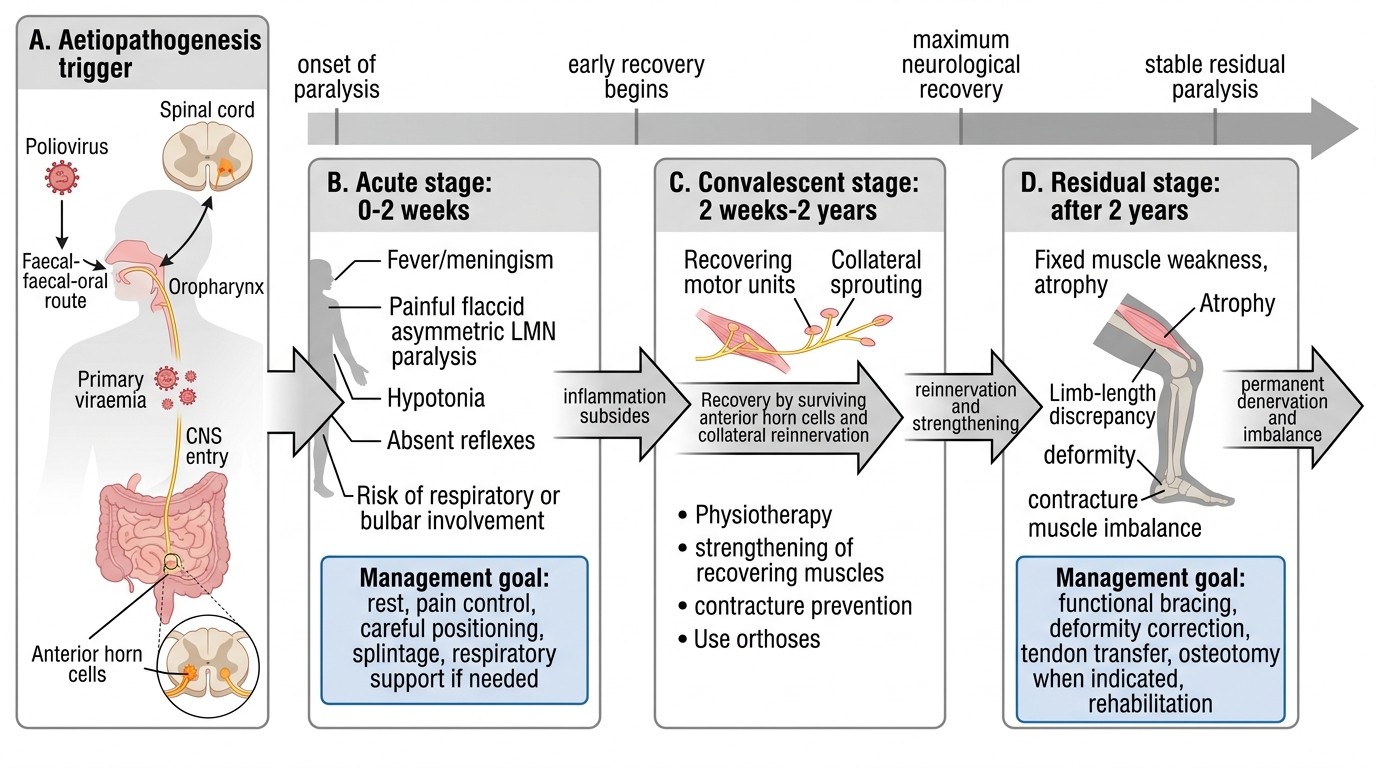
The clinical course of poliomyelitis passes through three well-defined stages, each with distinct orthopaedic implications. Understanding these stages is essential for setting the appropriate management goal at each phase and for communicating accurately with patients and families about what to expect.
Stage 1 — Acute Paralytic Stage (0 to 2 months): The child typically presents with a biphasic fever ('dromedary curve'), headache, meningism, and then the abrupt onset of asymmetric flaccid paralysis, usually maximal within 48–72 hours. The affected muscles are painful and tender (due to reactive inflammation around the dying anterior horn cells). Respiratory involvement (bulbospinal or bulbar polio) may threaten life and demands intensive-care monitoring. From an orthopaedic standpoint, management in this stage is entirely supportive: bed rest, analgesics, positioning of limbs in neutral or corrected position to prevent contracture, and splinting in the position of function. Active stretching or strengthening exercises are absolutely contraindicated while muscles are inflamed and painful.
Stage 2 — Convalescent Stage (2 months to 2 years): Once fever resolves, neurological function in surviving motor units begins to recover through two mechanisms: (a) recovery of reversibly damaged anterior horn cells that were stunned but not permanently destroyed, and (b) collateral re-innervation — axonal sprouting from surviving intact motor neurones that adopt denervated muscle fibres into enlarged motor units. Most recovery occurs in the first 6 months and is substantially complete by 2 years. Physiotherapy, active and passive exercises, and hydrotherapy are the mainstay of management to maximise recovery and prevent contracture formation. Lightweight callipers and ankle-foot orthoses are prescribed to maintain joint position and allow functional ambulation. Serial plaster splinting can correct dynamic deformities during this phase.
Stage 3 — Residual (Chronic) Stage (beyond 2 years): No further neurological recovery occurs. What remains is the permanent pattern of paralysis with secondary structural deformities. This is the stage at which the vast majority of patients present to the orthopaedic surgeon. The goals shift from recovery to function optimisation: correct established deformities, restore muscle power balance, achieve plantigrade weight-bearing, and restore independent ambulation where possible.
Stages of Poliomyelitis: Timeline, Features, and Management
Aetiopathogenesis: Poliovirus, Anterior Horn Cell Destruction, and Muscle Imbalance
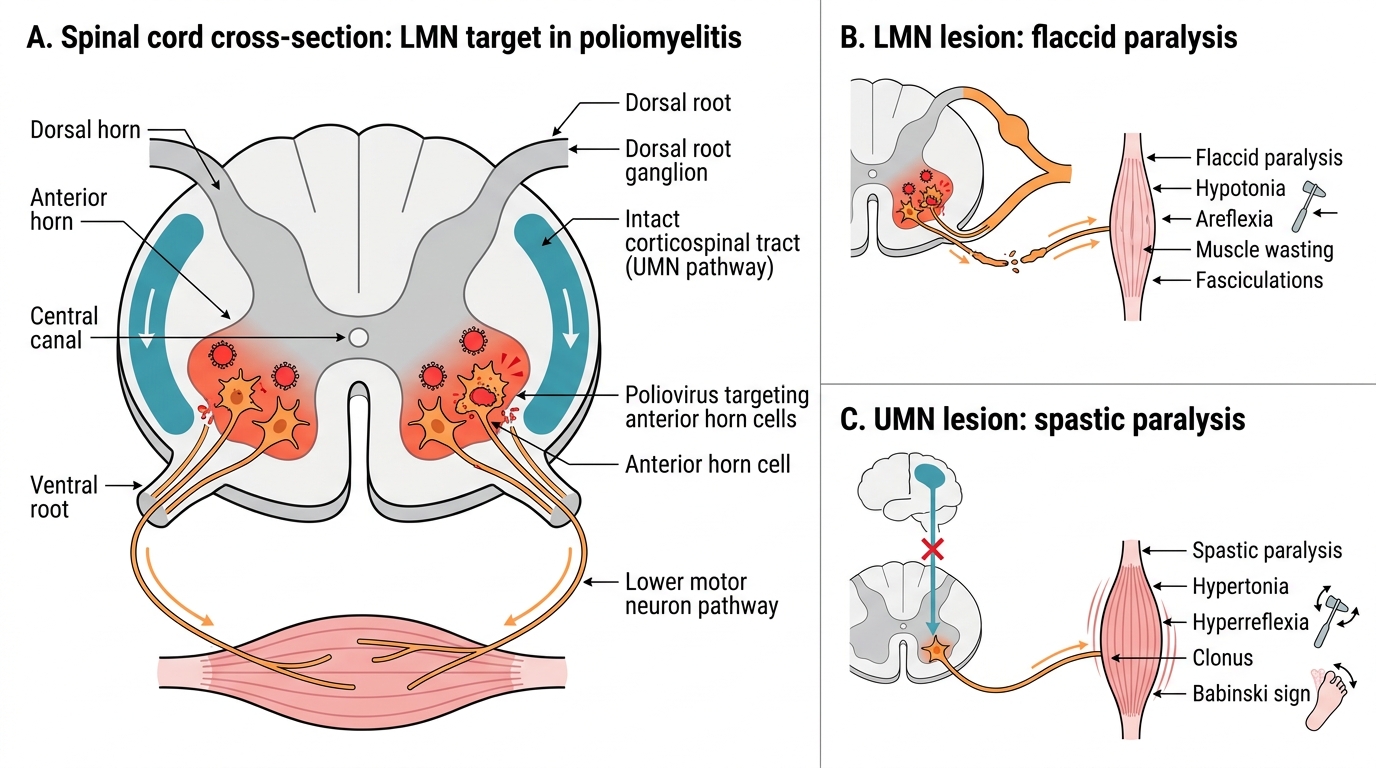
Poliomyelitis is caused by the poliovirus (an enterovirus, genus Enterovirus, three serotypes — type 1 is the most paralytogenic and responsible for the majority of epidemic outbreaks), which is transmitted via the faecal-oral route. After ingestion, the virus replicates in the oropharyngeal and intestinal epithelium, enters the bloodstream (primary viraemia), and in a minority of infected individuals — fewer than 1% of all those exposed — crosses the blood-brain barrier and enters the central nervous system. The critical and irreversible pathological event is selective destruction of anterior horn cells (AHCs) in the grey matter of the spinal cord, and the motor nuclei of cranial nerves in bulbar polio. The AHC is the final common pathway for all voluntary muscle contraction; its destruction produces a pure lower motor neurone (LMN) lesion with complete, irreversible muscle denervation.
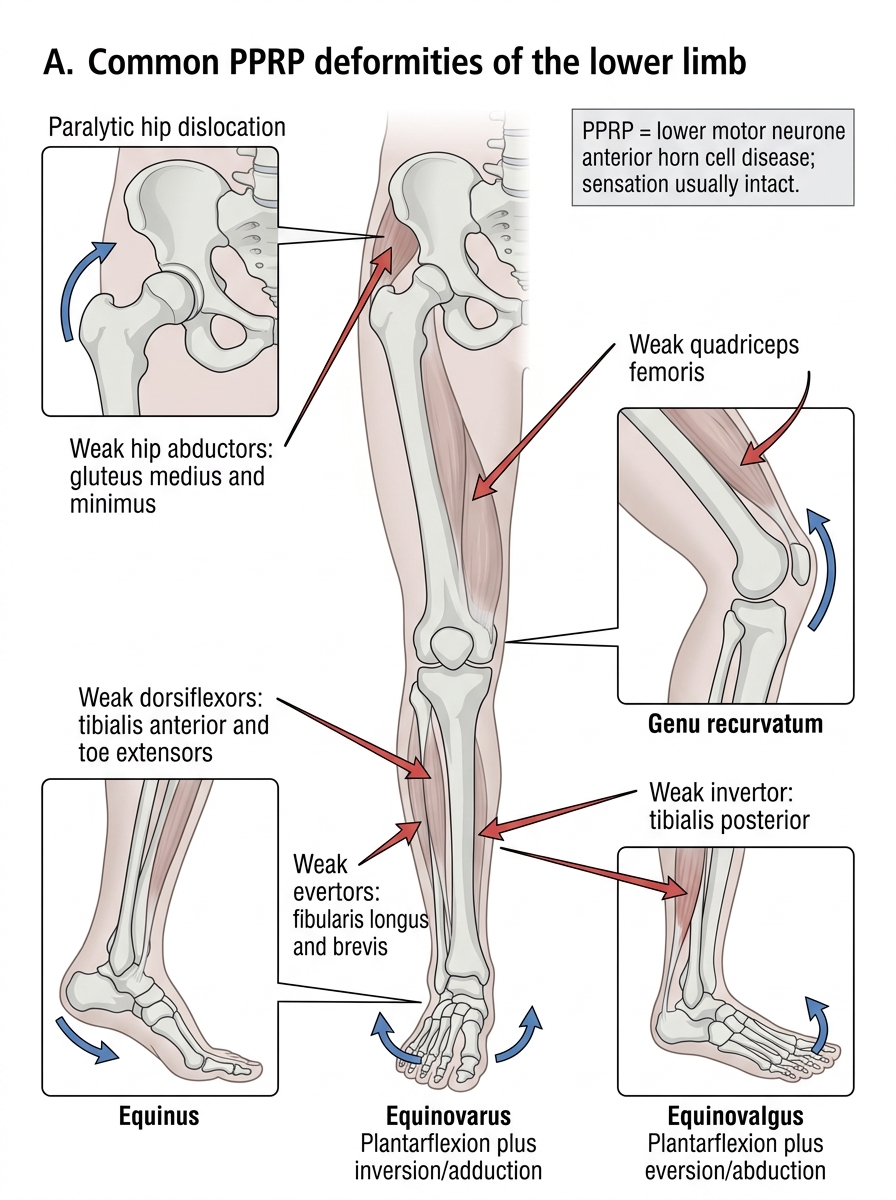
The pathological consequence of AHC destruction is characteristically asymmetric, patchy paralysis — because not every AHC at a given spinal segment is destroyed, and the virus does not respect dermatomal or segmental symmetry. This patchy pattern of denervation is the root cause of the muscle imbalance that drives deformity formation in PPRP. When the agonist of a joint is paralysed but its antagonist retains power, the unopposed stronger muscle continuously pulls the joint into a predictable deformity position. Over months to years, this paralytic position becomes first a dynamic (passively correctable) deformity, then a structural (fixed) deformity due to soft-tissue contracture and secondary bony remodelling.
Key downstream pathological consequences:
- Denervation atrophy — the affected limb is uniformly thinner (circumferential measurements reveal a significant shortfall vs the contralateral side)
- Trophic changes — impaired vasomotor tone and reduced mechanical loading produce osteoporosis, a cold limb, and shortening of the affected limb (limb-length discrepancy)
- Joint laxity — loss of active muscle tone allows progressive ligamentous stretching; flail joints are vulnerable to gravity-driven positional deformity
- Compensatory hypertrophy of innervated muscles in the same limb — these muscles carry excess load for decades and may eventually fail (the basis of post-polio syndrome in adults)
Critical neurological distinction for the OR arc: in PPRP the lesion is confined to the AHC — there is NO upper motor neurone involvement, NO pyramidal tract pathology, and NO basal ganglia involvement. Reflexes are ABSENT (the AHC is the efferent arc of the stretch reflex), tone is reduced or absent, and there is NO clonus, NO extensor plantar response (Babinski sign). This distinguishes PPRP categorically from cerebral palsy, where the primary lesion is in the brain or UMN tracts and spasticity dominates.
Poliomyelitis: LMN Versus UMN Pathways
Clinical Examination: Muscle Charting, Deformity Assessment, and Imaging
Clinical assessment of PPRP demands a systematic and highly detailed approach. The presenting complaint is almost always a deformity or functional disability in a child or young adult who had a febrile paralytic illness in infancy or early childhood. The examiner must document the full pattern of paralysis, characterise each deformity as dynamic or fixed, and assess functional capacity before any management plan is formulated.
History: Age at illness onset; vaccination status (Oral Polio Vaccine / Inactivated Polio Vaccine — 5-dose schedule under India's Universal Immunisation Programme); prior surgical or orthotic interventions; current functional status (ability to stand, walk unaided, distance walked, aids used). A history of new deterioration after years of stability raises the possibility of post-polio syndrome.
Inspection: Wasting (circumference measurements of both thighs and calves at fixed bony landmarks, comparing sides); limb-length discrepancy (real length: ASIS to medial malleolus; apparent length: umbilicus to medial malleolus); skin changes (shiny, cold, dystrophic nails — trophic signs); visible deformities (equinus, varus, valgus, genu recurvatum, paralytic scoliosis, pelvic obliquity).
Neurological examination — the PPRP signature:
- Tone: flaccid (reduced or absent)
- Reflexes: ABSENT (knee jerk absent, ankle jerk absent in lower limb polio)
- Plantar response: flexor or absent — NEVER extensor (Babinski) in pure PPRP
- Sensation: NORMAL throughout — poliovirus spares all sensory neurones; intact sensation distinguishes PPRP from peripheral neuropathies where both motor and sensory fibres are involved
Muscle charting (mandatory before any surgery): Systematic MRC grading (0–5) of every major muscle group: hip abductors (Trendelenburg test), hip extensors (gluteus maximus — prone extension), knee extensors (quadriceps), knee flexors (hamstrings), ankle dorsiflexors (tibialis anterior), ankle plantarflexors (gastrosoleus), invertors (tibialis posterior), evertors (peronei). A muscle must grade ≥4 to qualify as a tendon transfer donor.
Gait analysis: Equinus gait (toe-walk), calcaneal gait (heel-only, absent push-off), Trendelenburg gait (trunk lurch over affected side — weak hip abductors), genu recurvatum gait (compensatory knee hyperextension for quadriceps weakness).
Deformity classification: Dynamic (corrects passively to neutral) vs fixed (rigid, requires surgical correction before functional procedures).
Imaging: Weight-bearing AP and lateral X-rays of the affected limb to document joint alignment and deformity angles. Scanogram or CT scanogram for precise limb-length discrepancy measurement.
Common PPRP Deformities of the Lower Limb
SELF-CHECK
A child with PPRP is being assessed. The examiner finds absent deep tendon reflexes, flaccid tone, and wasting of the right lower limb. Sensation is intact throughout. Which nerve lesion level is responsible for this picture?
A. Upper motor neurone (cortex or descending tracts)
B. Lower motor neurone (anterior horn cell)
C. Peripheral sensorimotor nerve (peripheral neuropathy)
D. Dorsal root ganglion (sensory ganglion)
Reveal Answer
Answer: B. Lower motor neurone (anterior horn cell)
PPRP is an anterior horn cell (lower motor neurone) disease. LMN lesions produce flaccid paralysis, wasting, absent reflexes, and fasciculations. Sensation is intact because poliovirus selectively destroys motor neurones in the anterior horn, sparing sensory neurones in the dorsal horn and dorsal root ganglia. This distinguishes PPRP from peripheral neuropathies (which involve both motor and sensory fibres) and from UMN lesions (which produce spastic paralysis with preserved or exaggerated reflexes).