Page 3 of 13
OR8.1 | Post-polio Residual Paralysis — SDL Guide (Part 3)
Self-Assessment: Key Principles in PPRP
Self-assessment is the mechanism by which you confirm that passive reading has been converted into active, retrievable knowledge. Research in cognitive science consistently shows that the act of attempting to retrieve an answer — even imperfectly — produces more durable learning than re-reading the same material. Use this section as a closed-book exercise: cover the preceding content, attempt each question from memory, then return to the relevant section to verify and consolidate your answer. The five questions below are deliberately representative of the highest-yield examination domains for PPRP, covering neurological classification, surgical principles, deformity mapping, operative sequencing, and late complications. Final-year students are expected to apply these principles to clinical vignettes, not merely recall definitions.
The following structured questions cover the key testable domains of PPRP at a final-year MBBS and postgraduate entrance level:
- LMN vs UMN distinction: A patient presents with a childhood history of febrile paralytic illness. On examination: flaccid tone, absent knee and ankle jerks, wasting, normal sensation, no Babinski sign. A second patient presents with a similar history but shows spastic tone, brisk reflexes, and an upgoing plantar response. What is the diagnosis in each, and how do the deformity patterns and management strategies differ?
- Tendon transfer prerequisites: Name the four prerequisites for tendon transfer and explain why each is non-negotiable. What happens if you transfer a grade 3 muscle? What must be done if a fixed contracture exists before planning a functional procedure?
- Deformity-to-muscle-imbalance mapping: Which specific muscle group, when paralysed, produces (a) equinus foot, (b) calcaneal deformity, (c) genu recurvatum, (d) Trendelenburg gait? For each, name a tendon transfer that can restore balance.
- Staged surgical planning: A 10-year-old girl has a fixed equinovarus deformity (20° equinus, 15° varus) with tibialis posterior grade 4, peronei grade 2, tibialis anterior grade 1. Outline the operative sequence (step 1 → step 2), explaining why the order matters.
- Post-polio syndrome: At what interval after acute polio does PPS typically occur? What is its pathophysiology? Why is aggressive physiotherapy contraindicated?
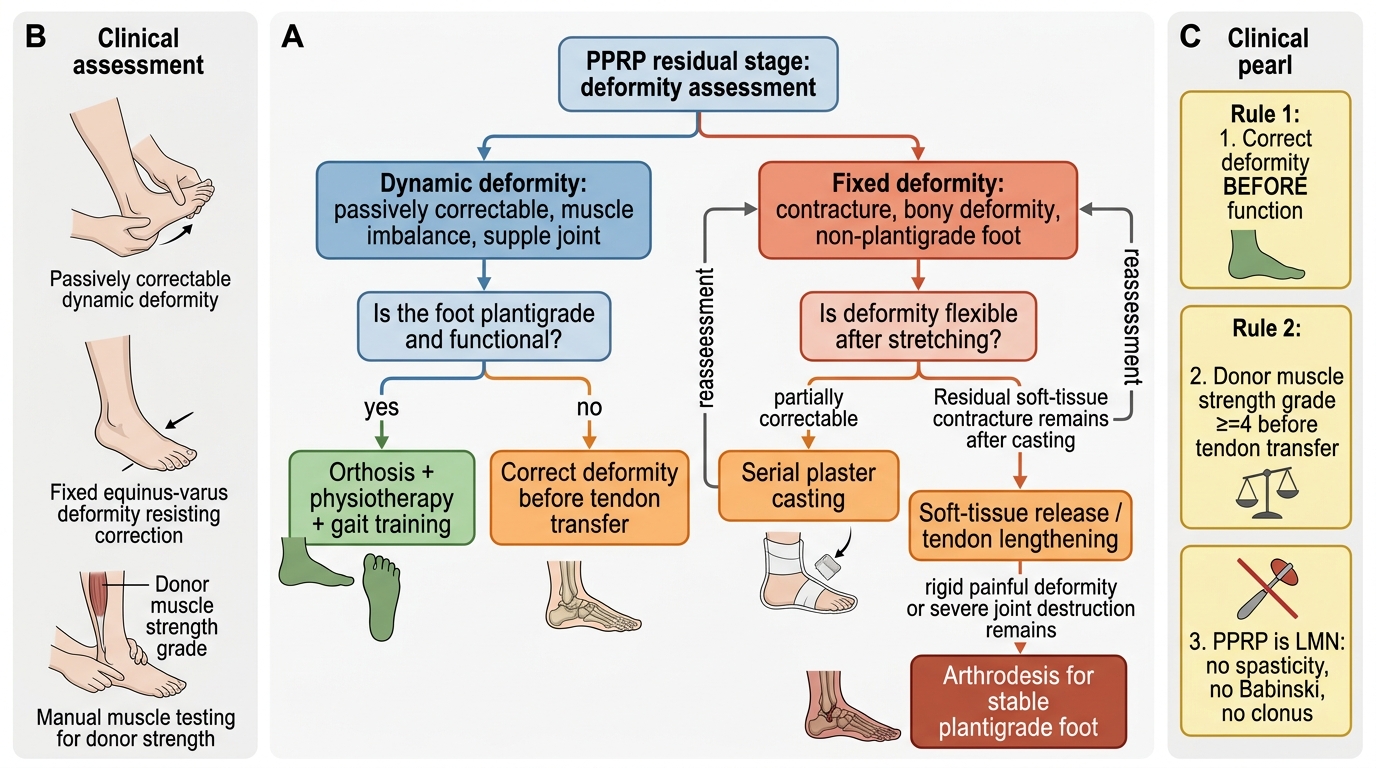
PPRP Residual Stage Management Algorithm
CLINICAL PEARL
The three most important clinical rules in PPRP: (1) Correct deformity BEFORE function — a tendon transfer onto a non-plantigrade foot or a contracted joint will fail. Achieve a supple, plantigrade foot first. (2) Grade ≥4 for the donor — resist the temptation to transfer a grade-3 muscle; the patient ends up worse than before surgery. (3) PPRP is a pure LMN disease — there is NO spasticity, NO Babinski, NO clonus. If any UMN sign is found in a supposed 'polio' patient, reconsider the diagnosis (cerebral palsy or combined pathology). This distinction changes every aspect of management.