Page 13 of 44
EN2.4 | Audiogram and Impedance Interpretation — SDL Guide
Learning Objectives
- Describe the correct technique for performing a pure tone audiogram (PTA) and explain the symbol conventions (O, X, ], [)
- Read and interpret a PTA to identify conductive, sensorineural, and mixed hearing loss patterns
- Calculate the pure tone average and classify hearing loss severity
- Interpret a tympanogram by identifying the Jerger type (A, B, C, Ad, As) and its clinical significance
- Integrate audiogram and tympanogram findings to reach a clinical diagnosis
INSTRUCTIONS
Pure tone audiometry and tympanometry are the two most important formal investigations in ENT hearing assessment. Together they quantify the degree of hearing loss, define its type (conductive, sensorineural, or mixed), and assess middle ear function. This module teaches you to read and interpret these investigations — skills tested in OSCEs, clinical postings, and the final MBBS examination.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Ch 3 (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Ch 6 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Vol 1, Ch 11 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are reviewing the investigation results for a 58-year-old retired factory worker referred for hearing loss. His audiogram shows: right ear AC thresholds of 55 dB at 4000 Hz and 65 dB at 8000 Hz, with progressively worse loss at higher frequencies; BC thresholds parallel the AC curve closely, with no gap between them. Left ear shows a similar pattern. His tympanograms are Type A bilaterally. Your attendant asks: 'So is this wear-and-tear deafness from the factory noise, or is it something else? And is there anything wrong with his middle ear?' How do you answer — and what do these numbers and curve shapes actually tell you?
WHY THIS MATTERS
EN2.4 requires you to both perform and interpret the PTA and impedance audiogram. In clinical practice, the audiologist usually performs the test, but the clinician must be able to interpret the result without relying on a report — because the report may be absent, delayed, or incorrect. More importantly, in underserved settings across India, you may be the only person available to perform a basic assessment and decide whether a patient needs amplification, medical treatment, or surgical intervention. The audiogram is also the primary medicolegal document in noise-induced hearing loss cases — occupational health assessments, compensation claims, and disability certification all depend on correctly interpreted PTA results. Understanding how to read an audiogram is therefore not an academic exercise but a professional obligation.
RECALL
Recall from physiology that the cochlea is tonotopically organised: high-frequency sounds (4000–8000 Hz) are processed at the base of the cochlea, while low-frequency sounds (250–500 Hz) are processed at the apex. The basal hair cells are the most metabolically active and the first to be damaged by noise, ototoxicity, and ageing — which is why noise-induced hearing loss and presbycusis preferentially affect high frequencies (especially 4000 Hz, the classic 'notch'). Recall also that sound is measured in decibels (dB) on a logarithmic scale — 0 dB HL (hearing level) represents the threshold of normal young adult hearing at each frequency, calibrated to statistical norms. A threshold of 40 dB HL means the patient needs a 40 dB increase in sound intensity (above the reference) to detect that frequency. Higher dB threshold = worse hearing. On the audiogram, the y-axis runs from –10 dB (better than average) at the top to 110–120 dB (profound loss) at the bottom — note that better hearing is at the TOP of the y-axis, which is counter-intuitive and a common reading error.
Clinical Indication: When and Why Pure Tone Audiometry Is Requested
Tuning fork tests provide a qualitative bedside classification of hearing loss — they tell you whether the loss is conductive or sensorineural, and which ear is affected. What they cannot provide is a quantitative measurement: they do not measure hearing thresholds in decibels, they cannot identify a 4 kHz notch characteristic of noise-induced hearing loss, they cannot distinguish mild from moderate from profound hearing impairment, and they cannot assess individual frequencies across the speech range to determine the impact on communication. Pure tone audiometry (PTA) addresses all of these limitations and is the gold standard for audiological assessment in ENT.
The clinical indication for PTA is any patient with a complaint of hearing loss or any finding on clinical examination that suggests hearing impairment. Specific situations requiring formal PTA include: (1) pre-operative assessment before tympanoplasty, mastoidectomy, or stapedectomy — the surgeon needs to know baseline thresholds to plan the procedure and counsel the patient about expected outcomes; (2) assessment of hearing aid candidacy — the type, severity, and configuration of hearing loss determines amplification requirements; (3) medicolegal assessment in occupational or noise-induced hearing loss; (4) monitoring of ototoxic drug effects (aminoglycosides, cisplatin, loop diuretics) — serial PTA tracks any progression; (5) differentiation of cochlear from retrocochlear pathology — a steeply sloping unilateral SNHL on PTA may indicate an acoustic neuroma (vestibular schwannoma), and the audiological pattern triggers MRI referral.
Impedance audiometry (tympanometry) complements PTA by assessing middle ear function directly. It is particularly valuable in children (in whom PTA is unreliable), in confirming or refuting a middle ear effusion (otitis media with effusion — 'glue ear'), and in evaluating Eustachian tube dysfunction. The acoustic reflex, tested as part of impedance audiometry, assesses the stapedius muscle reflex arc (CN VIII afferent, CN VII efferent) and can help localise the site of a lesion in SNHL.
The Audiometer and Impedance Bridge: Instrument Principles
Understanding what these instruments measure — and how measurement error occurs — makes the technique steps self-explanatory rather than a rote procedure.
The audiometer is an electronic instrument that generates pure tones (single-frequency sinusoidal signals) at precisely controlled frequencies (250–8000 Hz) and intensity levels (from –10 dB to 110 dB HL, in 5 dB steps). The patient signals each time they detect a tone (usually by pressing a button), and the examiner presents tones at decreasing intensity until the threshold is found. AC is tested through headphones (supra-aural or insert earphones); BC is tested through a bone vibrator placed on the mastoid process of the ear being tested. The standard testing protocol is the modified Hughson-Westlake ascending method: descend in 10 dB steps to a point where the patient cannot hear, then ascend in 5 dB steps until the patient responds — the threshold is the lowest level at which the patient responds in ≥50% of presentations at a given frequency.
For valid results: the patient must be positioned with their back to the audiometer (to prevent visual cueing); the room must be a sound-treated booth or a quiet room with ambient noise below 35 dB; insert earphones are preferred over supra-aural headphones because they provide better sound attenuation and eliminate the occlusion effect. Masking is required whenever testing the worse ear — the better ear receives a noise signal to prevent it from detecting the tones presented to the worse ear (contralateral crossover). Failure to mask when required produces spuriously good thresholds for the worse ear (the better ear responds instead), leading to an underestimation of the air-bone gap.
The impedance bridge (tympanometer) measures the compliance (mobility) of the tympanic membrane and middle ear system by delivering a probe tone (220 Hz or 226 Hz) into a hermetically sealed ear canal and varying the air pressure from +200 to –400 daPa. At the peak compliance point, the middle ear pressure equals the probe pressure, and the TM vibrates most freely. The output is plotted as a tympanogram — a graph of compliance (y-axis, in mL or mmho) against pressure (x-axis, in daPa). The acoustic reflex is tested by delivering a loud tone to the ear and recording the resulting compliance change due to stapedius muscle contraction — tested ipsilaterally and contralaterally.
SELF-CHECK
On a pure tone audiogram, the y-axis represents hearing level in dB. Better hearing (lower threshold) is plotted at the:
A. Bottom of the y-axis (higher dB values)
B. Top of the y-axis (lower dB values, near 0 dB)
C. Middle of the y-axis
D. It varies by laboratory
Reveal Answer
Answer: B. Top of the y-axis (lower dB values, near 0 dB)
On the audiogram, 0 dB HL (normal hearing threshold) is plotted at the TOP of the y-axis. The axis increases downward — a threshold of 50 dB HL is plotted lower than a threshold of 20 dB HL. This counter-intuitive layout means that 'worse hearing = lower on the audiogram.' A common reading error is to think that higher thresholds (plotted lower) mean better hearing — they mean worse hearing.
Reading the Pure Tone Audiogram
Reading an audiogram correctly requires mastering the symbol conventions and the axes before attempting interpretation. The conventions are standardised internationally and used uniformly across all audiological reports — which means that once you have learnt them, you can read any audiogram from any audiology laboratory in the world without needing a legend. This standardisation is a deliberate design choice: the audiogram is a medicolegal document, and its interpretation must be unambiguous regardless of where it was produced. The two axes encode the two fundamental dimensions of hearing measurement: what frequency is being tested (x-axis) and how loud the stimulus must be before the patient detects it (y-axis). Every clinical decision that follows from the audiogram — whether to recommend a hearing aid, to perform surgery, to diagnose noise-induced hearing loss, or to request an MRI for a suspected acoustic neuroma — flows from correctly reading these two axes and the symbols plotted on them. The symbol conventions distinguish right from left, and air conduction from bone conduction, using shape and colour; mastering these prevents the commonest audiogram misreading error, which is to confuse the AC and BC curves.
Axes:
- X-axis (horizontal): Frequency in Hz, plotted logarithmically from 250 Hz (left) to 8000 Hz (right). Standard test frequencies: 250, 500, 1000, 2000, 4000, 8000 Hz. Speech frequencies are primarily 500–4000 Hz.
- Y-axis (vertical): Hearing level in dB HL, from –10 dB (top, better than average) to 110 dB (bottom, profound loss). REMEMBER: better hearing = closer to the top.
Symbol conventions (international standard):
- Right ear air conduction: O (open circle), red ink
- Left ear air conduction: X (cross), blue ink
- Right ear bone conduction: ] (right-facing bracket, mastoid), red
- Left ear bone conduction: [ (left-facing bracket, mastoid), blue
- Masked symbols: triangle (Δ) for masked AC; square (□) for masked BC
- No response symbols: marked with an arrow downward from the last tested level
Reading the audiogram step by step:
1. Orient yourself: identify right ear (O, red) and left ear (X, blue). Confirm both AC and BC are plotted.
2. Read each threshold: at 1000 Hz right AC, what dB level does the 'O' fall at?
3. Calculate the air-bone gap (ABG) at each frequency: ABG = AC threshold (dB) − BC threshold (dB). A gap of >15 dB at a given frequency indicates a conductive component at that frequency.
4. Identify the audiogram configuration (the shape of the threshold curve):
- Flat configuration: thresholds similar across all frequencies — seen in conductive losses (wax, TM perforation, middle ear effusion)
- High-frequency sloping loss: thresholds worst at 4000–8000 Hz — seen in noise-induced hearing loss (often with a 4 kHz notch), presbycusis, SNHL
- Low-frequency notch/loss: thresholds worst at 250–1000 Hz — characteristic of early Meniere's disease (fluctuating low-frequency SNHL)
- Cookie-bite (mid-frequency notch): thresholds worst at 1000–2000 Hz — hereditary SNHL
5. Calculate the pure tone average (PTA): average of AC thresholds at 500, 1000, and 2000 Hz. This gives the single-number hearing level used for disability assessment and hearing aid fitting.
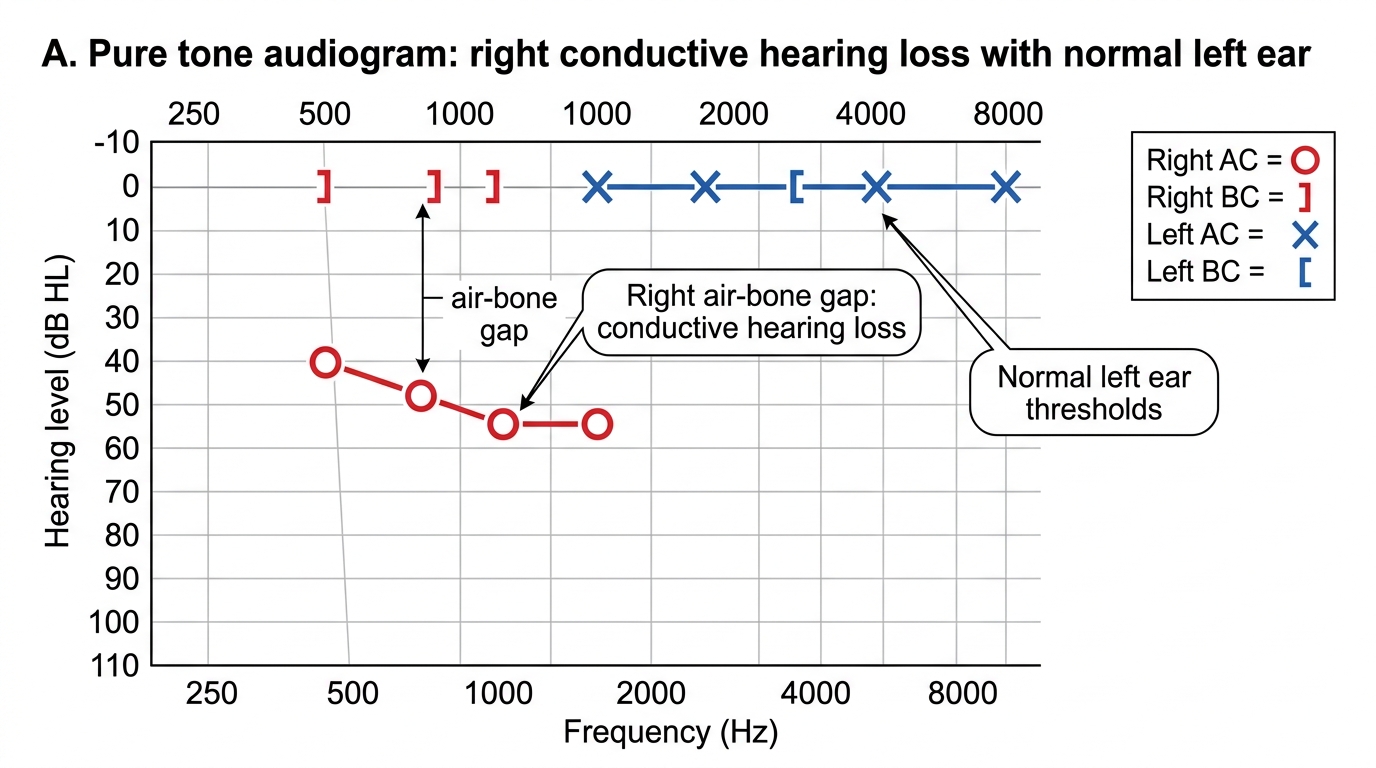
Pure Tone Audiogram: Right Conductive Hearing Loss