Page 1 of 44
EN2.1 | ENT History Taking and Case Presentation — SDL Guide
Learning Objectives
- Elicit a complete, structured ENT history using a systematic five-domain framework
- Characterise each major ENT symptom (hearing loss, otalgia, otorrhoea, tinnitus, vertigo, nasal obstruction, rhinorrhoea, epistaxis, hoarseness, dysphagia, neck swelling) with appropriate clarifying questions
- Identify red-flag symptoms in ENT history that require urgent investigation or referral
- Present an ENT case clearly and logically in a clinical or examination setting
INSTRUCTIONS
ENT complaints account for a significant proportion of primary-care and outpatient consultations in India. A poorly taken history leads to missed diagnoses — a patient with unilateral hearing loss and otalgia may have CSOM with cholesteatoma; a patient with hoarseness for six weeks may have laryngeal carcinoma. This module builds the disciplined, systematic approach to ENT history-taking and case presentation that underpins every subsequent clinical skill in this subject.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Ch 1, 2 (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Ch 3 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Vol 1, Ch 4 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the casualty medical officer at a district hospital. A 45-year-old male farmer is brought in by his wife. She says he has been 'losing his hearing' in the right ear for the past two years and lately has started getting severe headaches and has been 'confused' at times. The patient himself appears drowsy. You take a quick history — the ear has been discharging thick, foul-smelling pus intermittently for over a decade. Last week the discharge suddenly stopped, the ear 'dried up,' and the headaches began. What questions do you need to ask right now? And why does 'discharge that stopped' make things worse, not better?
WHY THIS MATTERS
The NMC 2024 competency EN2.1 is designated at the Skills/Habit (SH) level — meaning you are expected not merely to know what questions to ask, but to demonstrate, repeatedly and fluently, a complete, structured ENT history in clinical and examination settings. ENT is a specialty where the history alone can be diagnostic: the combination of unilateral conductive hearing loss + foul-smelling purulent otorrhoea + vertigo virtually clinches CSOM atticoantral (cholesteatoma) disease. In the scenario above, the cessation of discharge and new-onset headache suggests intracranial extension — a complication that is lethal if not recognised within hours. Conversely, ENT symptoms are frequently underreported because patients normalise them: many patients with significant hearing loss have never been asked about it directly. A systematic, unhurried, domain-by-domain history is the skill that separates the clinician who catches things from the one who misses them.
RECALL
Before working through the technique, briefly recall the anatomical and physiological foundations that make ENT symptoms interpretable. The ear consists of the outer ear (pinna and external auditory canal), middle ear (tympanic membrane, ossicular chain — malleus, incus, stapes — and Eustachian tube), and inner ear (cochlea for hearing, vestibular labyrinth for balance). Damage at different levels produces different symptom patterns: conductive hearing loss arises from problems in the external or middle ear (wax, TM perforation, ossicular disease, otitis media), while sensorineural hearing loss arises from cochlear or eighth nerve pathology. The nose serves olfaction, air conditioning, and resonance; the nasal mucosa is continuous with the paranasal sinuses via the ostiomeatal complex. The larynx is innervated by the recurrent laryngeal nerves (branches of the vagus); left-side RLN has a longer intrathoracic loop around the aortic arch. Cranial nerves VII (facial), VIII (vestibulocochlear), IX (glossopharyngeal), X (vagus), and XII (hypoglossal) are all relevant to ENT symptom localisation.
Why Systematic ENT History Taking Matters
ENT history taking is a procedural skill, not merely an act of remembering a list of questions. The discipline matters because ENT symptoms are remarkably non-specific in isolation: hearing loss, for example, can result from wax impaction (trivial), otitis media (common), CSOM (potentially dangerous), acoustic neuroma (rare but serious), or aminoglycoside toxicity (preventable if identified early). Similarly, hoarseness is caused by laryngitis, vocal cord nodules, recurrent laryngeal nerve palsy, and carcinoma of the larynx — conditions with vastly different urgency and management. Without a structured approach, crucial contextual information is gathered inconsistently, and patterns that would be diagnostic are missed.
The clinical indication for this skill is every patient who presents with an ENT complaint. There is no ENT subspecialty or general practice setting in which this skill is irrelevant — from a toddler with recurrent otitis media to a retired smoker with a neck mass, the history is the first and most powerful diagnostic tool available.
The three specific abilities that EN2.1 demands are: (1) eliciting — asking the right questions in a systematic, patient-centred manner; (2) documenting — recording the history in a structured format that communicates findings clearly; and (3) presenting — summarising the case orally or in writing to a senior clinician or an examiner. All three are assessed in the OSCE and in clinical postings, and all three are exercised in this SDL.
Anatomy of a Good ENT History: The Five Domains
A complete ENT history is organised into five mutually-reinforcing domains. This is not an arbitrary checklist — each domain maps onto a specific anatomical region and a specific set of pathologies, ensuring that no major symptom complex is omitted.
Provided image
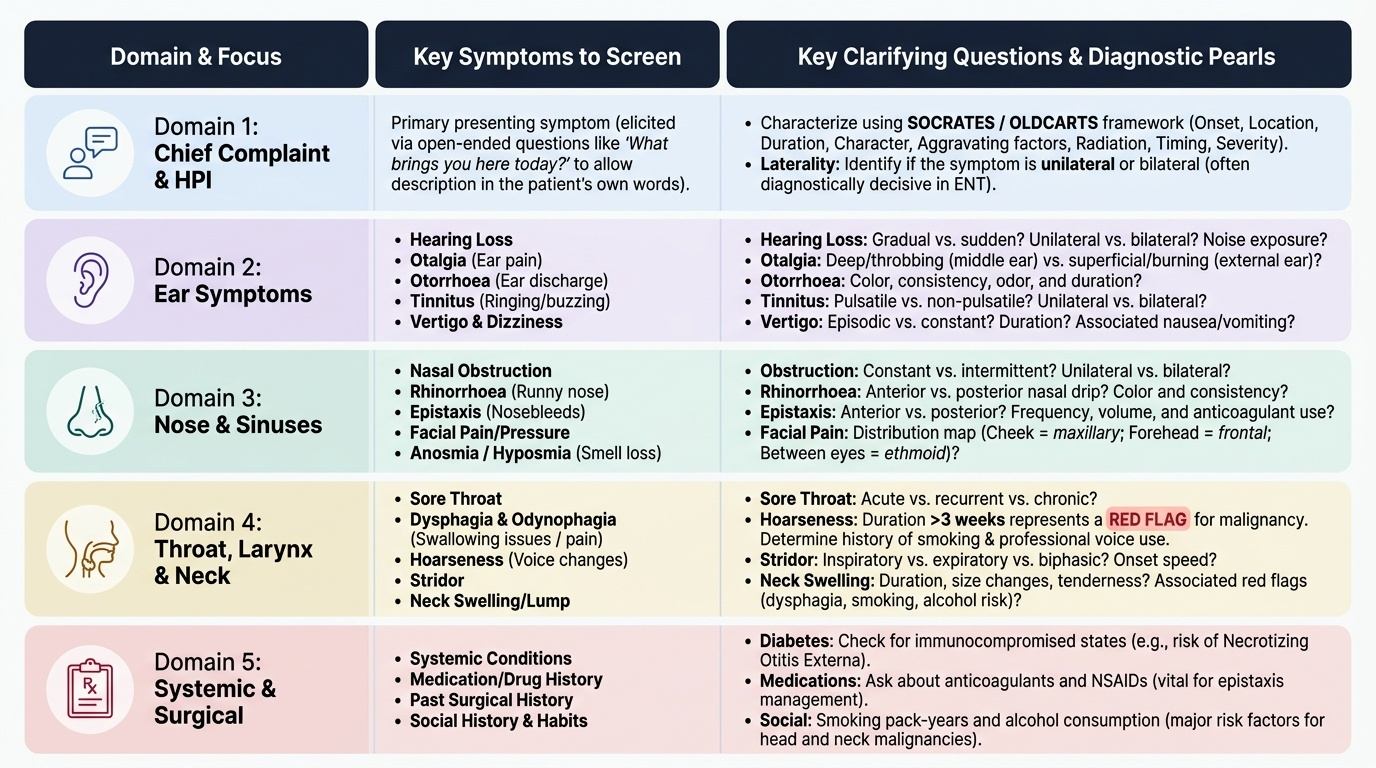
The framework proceeds as follows:
Domain 1 — Chief Complaint and History of Present Illness (HPI): Begin with an open question: 'What brings you here today?' Allow the patient to describe their primary symptom in their own words. Then characterise it using the SOCRATES / OLDCARTS framework: Onset, Location, Duration, Character, Alleviating/Aggravating factors, Radiation (for pain), Timing, and Severity. For ENT, the 'location' includes laterality (unilateral vs bilateral) — which is often diagnostically decisive.
Domain 2 — Ear Symptoms: Systematically screen for hearing loss (gradual vs sudden, unilateral vs bilateral, associated noise or infection), otalgia (pain — deep, throbbing vs superficial/burning), otorrhoea (discharge — colour, consistency, smell, duration), tinnitus (ringing/buzzing, unilateral vs bilateral, pulsatile vs non-pulsatile), and vertigo/dizziness (episodic vs constant, duration of episodes, associated nausea/vomiting, hearing change during attacks).
Domain 3 — Nose and Sinus Symptoms: Screen for nasal obstruction (unilateral vs bilateral, intermittent vs constant), rhinorrhoea (anterior vs posterior nasal drip, colour and consistency of discharge), epistaxis (anterior vs posterior, frequency, volume, precipitants, current medications especially anticoagulants/NSAIDs), facial pain or pressure (distribution: cheek for maxillary sinus, forehead for frontal sinus, between eyes for ethmoidal), and anosmia or hyposmia (loss/reduced sense of smell).
Domain 4 — Throat, Larynx, and Neck Symptoms: Screen for sore throat (acute vs recurrent vs chronic, dysphagia — difficulty swallowing, odynophagia — painful swallowing), hoarseness (duration: >3 weeks = red flag for malignancy, occupation as voice user, smoking history), stridor (inspiratory vs expiratory vs biphasic, onset — acute vs gradual), and neck swelling (duration, change in size, tenderness, associated hoarseness or dysphagia, smoking and alcohol history for malignancy risk).
Domain 5 — Systemic, Drug, and Surgical History: Relevant systemic conditions include diabetes (risk of malignant otitis externa), hypertension (epistaxis risk, cardiovascular cause of tinnitus), tuberculosis (cervical lymphadenopathy, nasopharyngeal involvement), HIV/immunosuppression (unusual opportunistic infections). Drug history must capture: aminoglycosides (ototoxicity), loop diuretics (ototoxicity), NSAIDs/anticoagulants (epistaxis risk), antihistamines/decongestants (relief of nasal symptoms). Past surgical history: any previous ear, nose, or throat surgeries; any tracheostomy; any neck dissection. Family history: hereditary hearing loss (Connexin 26 mutations), allergic rhinitis. Social history: occupation (noise exposure → noise-induced hearing loss), smoking (laryngeal, oral, and nasopharyngeal cancer risk), alcohol (pharyngeal and laryngeal cancer risk), living conditions.
SELF-CHECK
A 60-year-old male smoker presents with hoarseness for 8 weeks. The most important next step is:
A. Prescribe a proton pump inhibitor for presumed laryngopharyngeal reflux
B. Refer for laryngoscopy to exclude laryngeal malignancy
C. Prescribe voice rest and reassure
D. Request a thyroid ultrasound
Reveal Answer
Answer: B. Refer for laryngoscopy to exclude laryngeal malignancy
Hoarseness persisting for more than 3 weeks in a patient with smoking history is a red-flag symptom for laryngeal carcinoma and mandates laryngoscopy as the next investigation (per Dhingra and Scott-Brown's). Laryngeal carcinoma — particularly glottic carcinoma — presents early with hoarseness because of its location on the vocal cord. Empirical PPI therapy, voice rest, or thyroid imaging without laryngoscopy risks delayed diagnosis of a potentially curable malignancy.
Ear Symptoms in Depth
The ear section of the ENT history is the most complex because the ear's anatomy packs auditory, vestibular, and facial nerve functions into a small volume, and disease at one level typically produces a characteristic combination of symptoms. Mastering the characterisation of each ear symptom is therefore the core procedural skill of ENT history taking.
Provided image
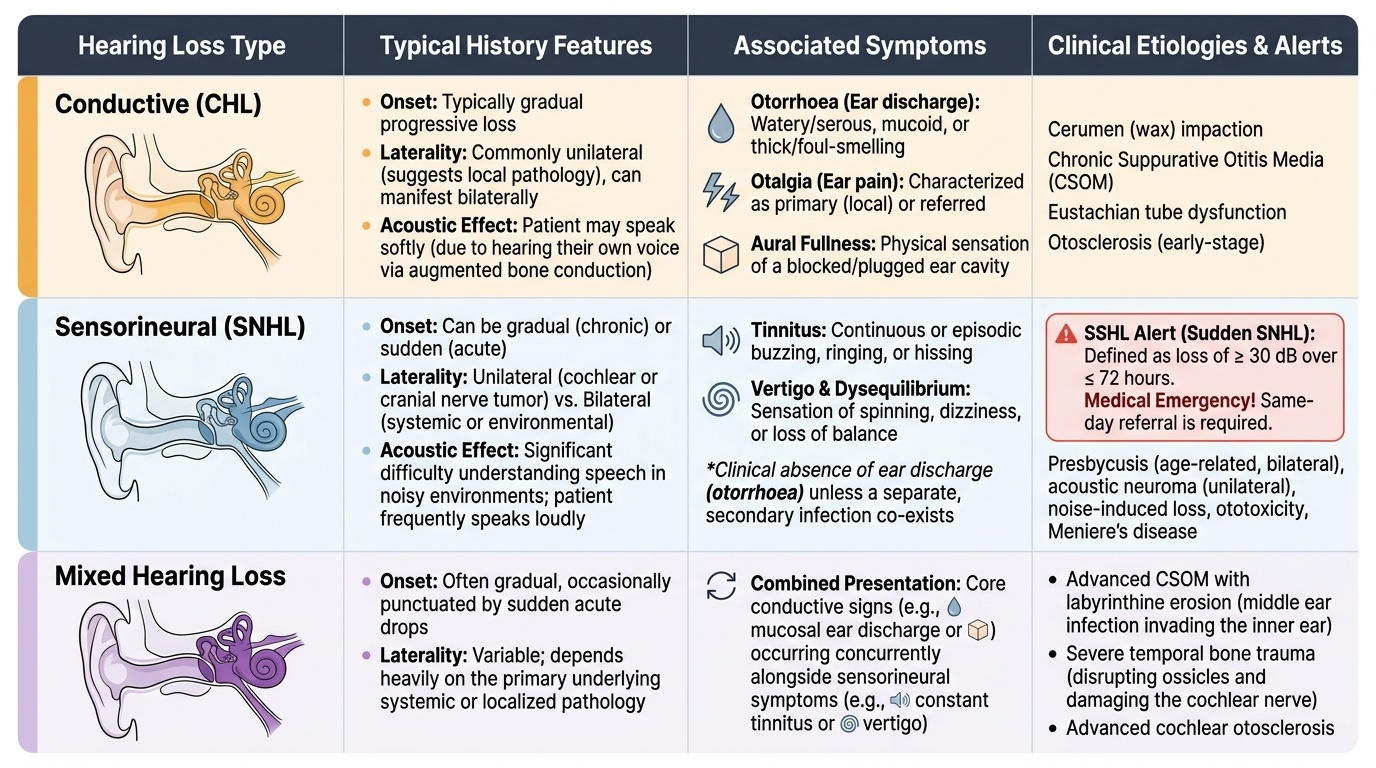
Hearing loss — Begin with onset: sudden hearing loss (defined as ≥30 dB loss over ≤72 hours) is a medical emergency (sudden sensorineural hearing loss, SSHL) requiring same-day referral, while gradual progressive loss suggests chronic middle ear disease or presbycusis. Establish laterality: unilateral loss points to local pathology (wax, CSOM, acoustic neuroma), while bilateral loss suggests a systemic cause (noise, ototoxicity, hereditary). Enquire about associated symptoms: a discharging ear with hearing loss = CSOM; hearing loss with tinnitus and vertigo = Meniere's disease or SSHL.
Otalgia (ear pain) — Characterise as primary (arising from the ear itself) or referred (from other structures sharing sensory innervation). The ear is innervated by branches of cranial nerves V, VII, IX, and X, and the C2/C3 cervical nerves. Referred otalgia is common and originates from dental disease (CN V), temporomandibular joint dysfunction, tonsillitis (CN IX), laryngeal pathology (CN X), or cervical spine disease (C2/C3). A patient with otalgia and a completely normal ear examination must prompt a thorough oral cavity, pharynx, and larynx examination to find the referred source.
Otorrhoea (ear discharge) — Characterise by type: watery/serous (otitis externa, CSF leak if following head injury), mucoid (Eustachian tube dysfunction), mucopurulent (CSOM tubotympanic type), and foul-smelling thick/cheesy (strongly suggests cholesteatoma = CSOM atticoantral type — the most dangerous). Ask about duration and whether the ear ever becomes 'dry' — sudden cessation of discharge in CSOM is an ominous sign suggesting the spread of infection beyond the ear, possibly toward the mastoid or intracranially.
Tinnitus — Ask about character: high-pitched ringing (sensorineural pathology), low-pitched buzzing or roaring (Meniere's — classically the tinnitus fluctuates with episodes), pulsatile tinnitus (synchronous with heartbeat — arteriovenous malformation, glomus tumour, carotid stenosis, benign intracranial hypertension). Pulsatile tinnitus always requires vascular imaging.
Vertigo and dizziness — The history must distinguish true vertigo (an illusion of rotational movement — suggests peripheral labyrinthine or central vestibular pathology) from dizziness/presyncope (light-headedness, near-fainting — cardiovascular). For true vertigo, ask: episodic or constant? Duration of episodes (seconds–minutes = BPPV triggered by position change; minutes–hours = Meniere's disease; days–weeks = vestibular neuritis, labyrinthitis). Associated hearing change during attacks? Dix-Hallpike positive = BPPV.