Page 17 of 44
EN2.6 | ENT Investigation Selection — SDL Guide
Learning Objectives
- Choose the correct investigation modality (radiological, microbiological, histological, or functional) for common ENT presentations
- Identify the appropriate radiological investigation for ear, nose/sinus, and throat/neck disorders
- Describe the correct technique for ENT microbiological specimens (ear swab, throat swab, FNAC)
- Interpret basic ENT investigation results: PNS X-ray, CT temporal bone report, FNAC cytology report
- Justify investigation selection using cost-effectiveness and clinical yield principles
INSTRUCTIONS
Choosing the right investigation for an ENT patient is a clinical skill that separates efficient, safe practice from expensive, potentially harmful over-investigation. This module covers the indications, limitations, and interpretation of the key radiological, microbiological, histological, and functional investigations used in ENT — with emphasis on selecting the minimum appropriate test and avoiding classic errors such as biopsying a vascular tumour.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Ch 2, 23, 36 (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Ch 4 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Vol 1, Ch 12 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the ENT outpatient clinic. Three patients are waiting. Patient 1: a 55-year-old male with a painless right neck mass for 8 weeks; he is a smoker. Patient 2: a 30-year-old female with chronic right ear discharge and hearing loss for 10 years; she had a normal X-ray mastoid done at a peripheral centre last year that was 'reported as normal.' Patient 3: a 14-year-old male with recurrent severe right-sided epistaxis and right nasal obstruction. For each patient, a junior colleague asks: 'What investigation shall we order?' What do you tell them — and what investigation would be dangerous to order for Patient 3?
WHY THIS MATTERS
EN2.6 sits at the intersection of clinical reasoning and investigative medicine: you must be able not merely to name investigations but to choose correctly between competing options and interpret the results. In real practice, investigation selection errors are among the most costly in ENT: ordering a plain X-ray instead of a CT for a patient with CSOM delays the diagnosis of cholesteatoma and intracranial extension; performing an open biopsy of a suspected parotid pleomorphic adenoma seeds tumour cells along the biopsy tract and complicates subsequent surgery; and biopsying a JNA in the clinic can cause fatal haemorrhage. These errors are entirely preventable by applying a simple investigation selection framework — which is what this SDL teaches. The competency EN2.6 is SH level: you must be able to describe and choose correctly, and to begin interpreting results under supervision.
RECALL
Recall the basic imaging principles from your radiology orientations. Plain X-rays are produced by differential attenuation of X-rays by tissues: bone (white/opaque), air (black), soft tissue (grey). They are cheap, fast, and use low radiation but have limited soft tissue resolution. CT (computed tomography) uses X-rays at multiple angles to reconstruct cross-sectional slices; bone windows optimally show bony structures (temporal bone erosion, sinus walls); soft tissue windows show masses and lymph nodes. MRI uses magnetic fields and radiofrequency pulses — no ionising radiation; superior soft tissue contrast; the investigation of choice for nerve lesions, soft tissue tumours, and intracranial extension. Ultrasound uses high-frequency sound waves — no radiation; real-time guidance for FNAC; preferred for superficial neck masses. FNAC (fine needle aspiration cytology) uses a 23–25 gauge needle to sample cells from a mass without excision — the least invasive tissue diagnosis method. Understanding these principles allows you to predict which modality will answer the clinical question most efficiently.
Clinical Indication: Choosing Investigations for ENT Disorders
The guiding principle of investigation selection in ENT — as in all of medicine — is: choose the investigation that will most efficiently and safely answer the clinical question, with the minimum harm to the patient. This principle has three practical corollaries that are specific to ENT practice and prevent the most consequential errors.
The first corollary is that clinical examination precedes investigation. An investigation ordered without a preceding clinical examination is often the wrong investigation — it answers a question the clinician has not yet asked. In ENT, the history and examination (otoscopy, anterior rhinoscopy, tongue depressor, headlamp) frequently provide enough information to make the diagnosis without any investigation, or to select the one specific investigation needed. A patient with a central TM perforation and mucopurulent otorrhoea does not need imaging — they need a microbiological swab and audiometry. A patient with a palpable neck node requires FNAC, not imaging as the first step.
The second corollary is the do-not-biopsy rule for vascular lesions. Any presentation that could represent a juvenile nasopharyngeal angiofibroma (adolescent male + unilateral nasal obstruction + recurrent epistaxis) or a glomus tumour must NEVER be biopsied in the clinic. The diagnosis of both conditions is made radiologically — contrast CT and/or MRI and angiography — not by tissue sampling. Biopsy in these settings causes catastrophic, potentially fatal haemorrhage. This rule must be applied before ordering any investigation in these presentations.
The third corollary is that FNAC is the first-line tissue investigation for neck masses, not open biopsy. Open biopsy of a lymph node or parotid mass causes tumour seeding, disrupts tissue planes, complicates subsequent surgery, and may be the first step in converting a curable malignancy into one that is not. FNAC with or without ultrasound guidance provides cytological diagnosis, identifies the need for further staging, and guides management without these harms. Open biopsy is reserved for cases where FNAC is inconclusive and a tissue diagnosis is urgently required.
Radiological Investigation Principles and Modality Selection
Radiological investigation in ENT is stratified by region and clinical question. The choice between plain X-ray, CT, and MRI is determined by what tissue type needs to be visualised, how precisely, and what degree of radiation exposure is acceptable.
Provided image
Plain X-rays in ENT:
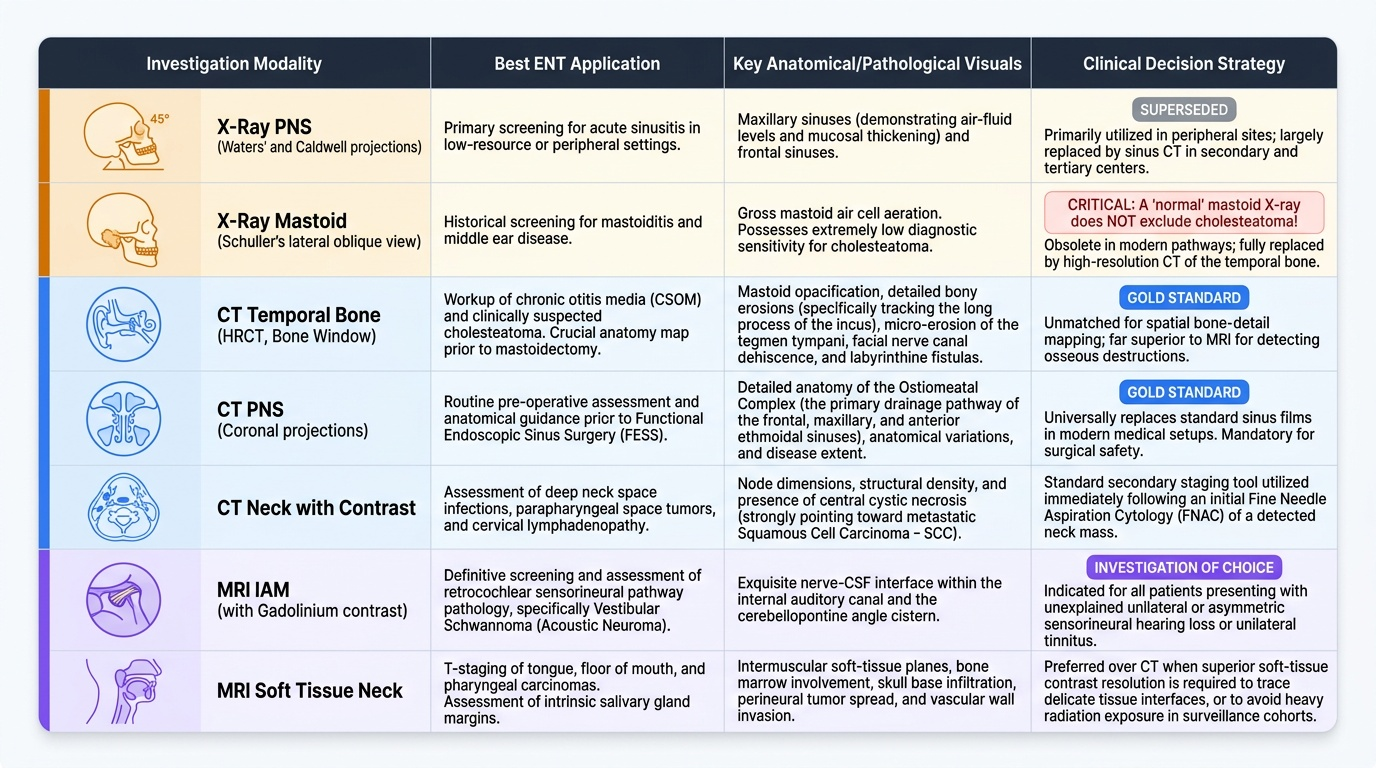
Paranasal sinuses: The Waters' view (occipito-mental projection) is the standard X-ray view for the paranasal sinuses; it shows the maxillary sinuses (air fluid levels or mucosal thickening) and the frontal sinuses well. It is used for screening in acute sinusitis where imaging is indicated. The Caldwell view (postero-anterior) is better for the ethmoidal and frontal sinuses. Plain X-rays of the sinuses have largely been superseded by CT in secondary care, but remain in use at peripheral settings.
Mastoid/temporal bone: Schuller's view (lateral oblique projection of the mastoid) was historically used for mastoid disease but has very limited diagnostic accuracy for cholesteatoma. It has been almost entirely superseded by CT temporal bone in secondary and tertiary ENT care. A 'normal' mastoid X-ray does NOT exclude cholesteatoma — this is a critical point when receiving investigation reports from peripheral centres.
CT in ENT:
CT temporal bone (HRCT — high resolution CT): The investigation of choice for chronic ear disease, including CSOM and cholesteatoma. CT temporal bone in bone window settings shows: mastoid air cell opacification, ossicular chain erosion (particularly the long process of incus — the most commonly eroded ossicle in cholesteatoma), tegmen erosion (intracranial extension), labyrinthine fistula, and facial nerve canal erosion. It is mandatory before mastoidectomy surgery.
CT paranasal sinuses: The gold standard investigation before functional endoscopic sinus surgery (FESS). Shows the ostiomeatal complex (the common drainage pathway for frontal, maxillary, and anterior ethmoid sinuses), extent of disease, and any anatomical variants. Coronal cuts are most informative.
CT neck with contrast: For neck masses, lymphadenopathy, parapharyngeal masses, and assessment of lymph node characteristics (size, density, central necrosis — suggesting metastatic SCC). Used after FNAC for staging.
MRI in ENT:
MRI internal auditory meati (IAM) with gadolinium: The investigation of choice for suspected acoustic neuroma (vestibular schwannoma) — the nerve is soft tissue, invisible on CT. Gadolinium-enhanced MRI shows the tumour within the IAM and any extension into the cerebellopontine angle. MRI IAM is indicated whenever a patient has unilateral SNHL, unilateral tinnitus, or asymmetric audiogram without an obvious cause.
MRI soft tissue neck/nasopharynx: Superior soft tissue contrast makes MRI preferred for nasopharyngeal carcinoma (NPC — particularly intracranial extension through the skull base), parapharyngeal tumours, and retropharyngeal masses.
SELF-CHECK
A 45-year-old male with long-standing right ear discharge and right-sided hearing loss is being evaluated before possible mastoidectomy surgery. The most appropriate pre-operative radiological investigation is:
A. X-ray mastoid (Schuller's view)
B. High-resolution CT of the temporal bone
C. MRI of the internal auditory meatus
D. X-ray skull (lateral view)
Reveal Answer
Answer: B. High-resolution CT of the temporal bone
High-resolution CT of the temporal bone (HRCT temporal bone) is mandatory before mastoidectomy surgery. It shows the extent of mastoid disease, ossicular chain erosion (especially the long process of incus), tegmen integrity (risk of intracranial extension), labyrinthine fistula, and facial nerve canal erosion — all of which directly influence the surgical approach. A Schuller's X-ray has very limited diagnostic accuracy for cholesteatoma and is no longer the standard of care. MRI IAM is used for acoustic neuroma/nerve lesions, not chronic ear disease. A normal plain X-ray does NOT exclude cholesteatoma.
Microbiological and Histological Investigation Technique
Microbiological and histological investigations in ENT serve different clinical goals and require different techniques. Using the wrong sampling method — for example, a superficial swab from a discharging ear that only picks up colonising organisms rather than the true pathogen — gives a misleading result and leads to inappropriate antibiotic prescribing.
Ear swab for microbiological culture:
An ear swab is indicated in CSOM with active otorrhoea, otitis externa not responding to empirical treatment, and post-operative ear infections. Technique: clean the external canal gently to remove superficial debris; take a swab deep in the canal from the freshest discharge emerging from the middle ear (not the canal skin flora). Request aerobic and anaerobic bacterial culture plus fungal culture (otomycosis is common in tropical climates — Aspergillus, Candida). Common organisms in CSOM: Pseudomonas aeruginosa, Staphylococcus aureus, Bacteroides (anaerobic). Common organisms in otomycosis: Aspergillus niger (black spores), Aspergillus flavus (yellow-green), Candida.
Throat swab:
Indicated in acute exudative tonsillitis, peritonsillar abscess (pus from incision), recurrent tonsillitis, and suspected diphtheria. Technique: ask the patient to open wide and say 'Ah'; swab the tonsillar surface and posterior pharyngeal wall directly (not the tongue). Label for culture and sensitivity; for suspected diphtheria, send for Löffler's medium and toxigenicity testing.
FNAC (Fine needle aspiration cytology) of neck masses:
FNAC is the first-line tissue diagnosis investigation for any neck mass. It is performed with a 23–25 gauge needle, with or without ultrasound guidance. Pass the needle into the mass with a slight suction on the syringe, make 3–4 passes in different directions, release suction before withdrawing, and smear the aspirate on glass slides (half fixed, half air-dried). The cytopathologist reports: cellular adequacy, cytological features (reactive vs malignant), and if malignant, the cell type (squamous cell carcinoma, adenocarcinoma, lymphoma, etc.). Ultrasound-guided FNAC is preferred for impalpable, deep, or cystic masses.
Open biopsy of laryngeal/oropharyngeal lesions:
For suspicious mucosal lesions in the larynx or oropharynx, biopsy is performed under general anaesthesia via direct laryngoscopy or microlaryngoscopy (suspension laryngoscopy). Never attempt blind biopsy of a suspected JNA (vascular tumour — fatal haemorrhage risk). For oral cavity and oropharyngeal lesions, punch biopsy under local anaesthesia is standard.