Page 21 of 44
EN2.7 | ENT Surgical Instruments — SDL Guide (Part 2)
Throat and Airway Surgical Instruments
Throat and airway surgery covers a diverse set of procedures from the elective (adenotonsillectomy) to the emergency (tracheostomy, foreign body removal). Each has a characteristic instrument set, and the ability to identify these instruments from their physical appearance is a core OSCE skill.
Adenotonsillectomy instruments:
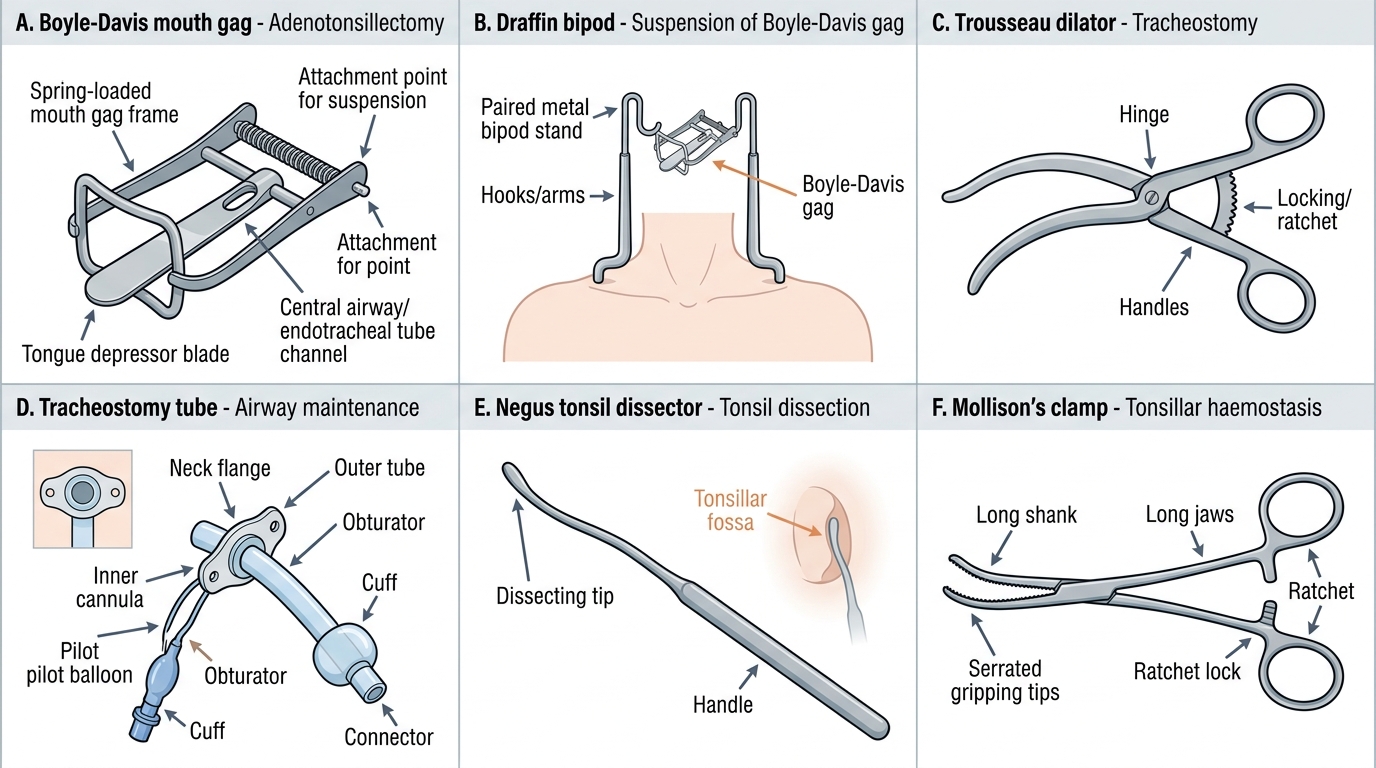
Boyle-Davis mouth gag: The signature instrument of adenotonsillectomy. It is a spring-loaded mouth gag with a tongue depressor blade that keeps the mouth wide open and the tongue depressed, providing access to the oropharynx. The tongue blade has a central channel that accommodates the endotracheal tube during general anaesthesia. The gag is attached to a supporting stand (Draffin bipod or a Mayo stand) to maintain its position without the surgeon having to hold it.
Draffin bipod (bipod stand): A metal bipod stand that attaches to the Boyle-Davis gag and rests on the patient's chest, holding the gag in position during adenotonsillectomy.
Negus tonsil dissector: A curved instrument used for blunt dissection of the tonsil from its peritonsillar space capsule during tonsillectomy.
Mollison's haemostatic tonsil clamp: A curved artery clamp used to secure bleeding points in the tonsillar fossa after tonsil removal.
Adenoid curette (Beckmann curette): A ring-shaped curette with a sharp edge on one side, used to scrape the adenoid tissue from the posterior nasopharyngeal wall.
Foreign body removal instruments:
Chevalier Jackson laryngoscope: A rigid direct-vision laryngoscope used for direct laryngoscopy and the removal of foreign bodies from the larynx and proximal trachea.
Hopkins rod telescope: Used in conjunction with the rigid laryngoscope to provide endoscopic visualisation of the larynx and trachea.
Rigid oesophagoscope: A long metal tube used for visualising and removing foreign bodies from the oesophagus (foreign body in the food passage) under general anaesthesia. Distinct from the flexible oesophagoscope.
Barron's (Magill) forceps: Angled forceps used to retrieve foreign bodies from the oesophagus or the larynx/trachea under direct vision.
Tracheostomy instruments:
Tracheostomy hook: A sharp single hook used to retract the tracheal wall upward (toward the surgeon) during the procedure to facilitate incision and tube insertion.
Trousseau dilator: A hinged instrument with two blunt ends that, when inserted closed into the tracheal incision and opened, dilates the incision to allow the tracheostomy tube to be inserted. The key design feature is that it dilates by spreading — not by cutting — so it is safer around the posterior tracheal wall.
Tracheostomy tube: A curved flanged tube with an inner cannula (for cleaning without tube removal) and usually a cuff (inflatable balloon to seal the airway and prevent aspiration). Available in various sizes; made of PVC, silicone, or metal (silver).
Throat and Airway Surgical Instruments
Interpreting the Clinical Context: Matching Instruments to Procedures
In the OSCE instrument identification station, the instrument is shown without context. The examination technique is to identify the instrument by its physical features and then connect it to its surgical procedure through knowledge of function. This section provides the framework for that interpretive mapping.
The key identifying features of ENT instruments that allow identification even when the name is forgotten are: (a) size — ear instruments are miniature (Rosen needle, Plester knife) while throat instruments are large (Boyle-Davis gag); (b) shape — the curve of a Trousseau dilator is distinctive (hinged, expanding); the cup shape of Blakesley forceps is specific to FESS; the ring shape of an adenoid curette is unique; (c) function mechanism — a spreading/dilating instrument (Trousseau) vs a cutting instrument (myringotomy knife) vs a holding/retracting instrument (Mollison's retractor, Boyle-Davis gag).
The procedure-to-instrument mapping is as follows:
- Tympanoplasty: operating microscope, Hartmann aural speculum, Rosen needle, Plester sickle knife, tympanoplasty microsurgical instruments
- Mastoidectomy: Mollison's self-retaining retractor, Lempert elevator, mastoid drill and burrs, mastoid chisels and curettes
- Myringotomy: Hartmann speculum, myringotomy knife (Beaver blade), grommet inserter, operating microscope or otoscope
- Septoplasty: Killian speculum, Cottle's elevator, Freer's elevator, osteotome, mallet
- FESS: Hopkins rod endoscope (0°, 30°), Blakesley forceps, Stammberger punch, microdebrider
- Nasal bone reduction: Walsham forceps, Ash forceps
- Adenotonsillectomy: Boyle-Davis gag, Draffin bipod, Negus dissector, Mollison's clamp, Beckmann adenoid curette
- Foreign body removal (airway): Chevalier Jackson laryngoscope, Hopkins rod, Magill/Barron forceps
- Foreign body removal (oesophagus): Rigid oesophagoscope, Barron forceps
- Tracheostomy: tracheostomy hook, Trousseau dilator, tracheostomy tube (cuffed, with inner cannula)
CLINICAL PEARL
The tracheostomy tube has three essential components that are tested in OSCEs: (1) the outer cannula — the main tube that sits in the trachea; (2) the inner cannula — a removable inner tube that can be cleaned and replaced without removing the outer tube (critical for maintaining airway patency in the early post-operative period when secretions are heavy); (3) the cuff — an inflatable balloon that seals the airway below the larynx, preventing aspiration and allowing positive-pressure ventilation. A decannulation (removal) cap is used during the weaning process to progressively reduce the tube size before final removal. Knowing these components allows you to assist with tracheostomy care confidently and to counsel patients and families.
Applied Practice: Instrument Identification Scenarios
The OSCE instrument identification station tests whether you can identify, name, and contextualise ENT surgical instruments in the structured format expected by examiners. The following scenarios mirror the way these questions are posed in clinical examinations and allow you to practise the correct response structure: name, describe, surgical use, anatomical site or important detail.
Scenario 1 — The expanding hinged instrument:
You are shown a metal instrument with two blunt, slightly curved arms joined at a pivot. When the handle is squeezed, the arms splay open. Name: Trousseau tracheal dilator. Description: hinged, expanding instrument with two blunt arms. Surgical use: used during tracheostomy to dilate the tracheal incision after the trachea has been incised between the 2nd and 3rd tracheal rings. Allows insertion of the tracheostomy tube without the risk of posterior tracheal wall perforation. The blunt expansion mechanism (not a cutting mechanism) makes it safer around the posterior wall.
Scenario 2 — The large mouth gag with a tongue blade and central channel:
You are shown a large spring-loaded instrument with a central depression in the tongue blade and a ratchet mechanism. Name: Boyle-Davis mouth gag. Description: spring-loaded mouth gag with a tongue depressor blade containing a central ET tube channel. Surgical use: adenotonsillectomy — maintains the mouth open, depresses the tongue, and accommodates the ET tube during GA. Suspended from a Draffin bipod stand. The instrument is not a direct manipulation tool — it creates and maintains the operative field.
Scenario 3 — The curved ring-shaped curette:
You are shown a long-handled instrument with a ring-shaped end, one side of which has a sharp cutting edge. Name: Beckmann adenoid curette. Surgical use: adenoidectomy — the ring is placed at the junction of the posterior nasopharynx and the skull base; a sweeping movement scrapes the adenoid tissue from the posterior nasopharyngeal wall. The sharp edge is directed toward the adenoid tissue, not toward the Eustachian tube orifices (which are lateral) — careless technique causes Eustachian tube injury.