Page 5 of 17
EN4.2 | External Ear Diseases — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis of External Ear Diseases
External ear diseases form a diagnostically rich group precisely because the external ear is so accessible to direct examination. A systematic approach separating pinna from EAC conditions, combined with the otoscopic findings and key clinical features, usually allows a confident diagnosis. The conditions below are grouped by anatomical location and arranged in order of clinical importance.
Provided image
Pinna conditions:
Haematoma auris: A subperichondrial collection of blood following blunt pinna trauma. On examination, a smooth, fluctuant, non-tender swelling overlying the helix or antihelix appears within hours of trauma. The lobule is spared. The skin over the haematoma is normal coloured or mildly erythematous. If untreated, the haematoma organises into fibrocartilaginous tissue over days to weeks, producing the permanent cauliflower ear deformity — a cosmetic and reconstructive problem. Treatment must be undertaken within 48–72 hours of injury (aspiration or incision and drainage) before organisation occurs.
Perichondritis: Bacterial infection of the perichondrium and subperichondrial space of the pinna, most commonly caused by Pseudomonas aeruginosa (especially after cartilage piercings, burns, or trauma). Presents as diffuse, hot, red, very tender pinna swelling that conspicuously spares the lobule — this lobule-sparing pattern is the single most useful clinical distinguishing feature from cellulitis. A fluctuant area suggests subperichondrial abscess formation. If untreated, the infection destroys the cartilage (pus between perichondrium and cartilage cuts off blood supply) → cartilage necrosis → permanent deformity.
Keloid of pinna: Keloid is a benign but disfiguring overgrowth of fibrous tissue beyond the original wound margin. In the pinna, it most commonly follows ear piercing through the lobule (less often through cartilage). It presents as a firm, rubbery, non-tender nodule or mass. Indian patients are at higher risk for keloid formation due to genetic predisposition. Recurrence after excision is common and high (>50%); post-excision pressure therapy, intralesional steroid injection, or silicone sheeting reduces recurrence.
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) of pinna: The helix is a sun-exposed surface and a common site for skin malignancy in elderly patients. BCC presents as a pearly, nodular or ulcerated lesion with a rolled edge. SCC presents as an indurated, ulcerated lesion that may be faster-growing. Any ulcerated pinna lesion in an older patient should be biopsied.
EAC conditions:
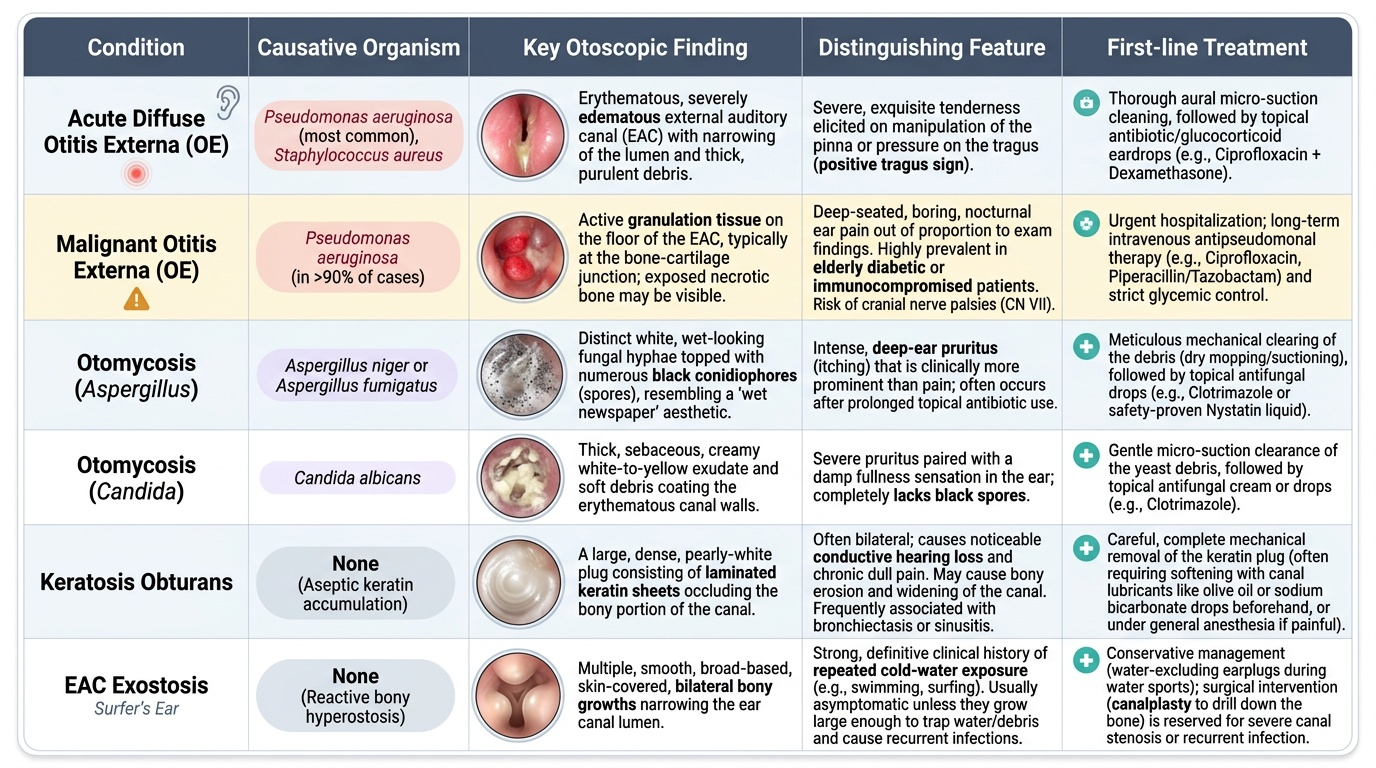
Acute diffuse otitis externa (swimmer's ear): The most common EAC disease. Risk factors include water exposure (disrupts cerumen; raises canal pH), cotton bud use (trauma + removal of protective cerumen), hearing aids, and humid climates. Caused predominantly by Pseudomonas aeruginosa and Staphylococcus aureus. Symptoms: severe otalgia, positive tragal sign, thin watery discharge progressing to purulent, EAC skin erythema and oedema. The TM may be visible and is normal (distinguishing from AOM). Conductive hearing loss if canal is occluded by oedema or debris.
Otomycosis (fungal OE): Fungal infection of the EAC, most commonly caused by Aspergillus niger (produces characteristic black spore heads on white hyphae, resembling the inside of a 'pepper pot') and Candida albicans (white curd-like deposits). Pruritus (itching) is the predominant symptom, more than pain — this itching-predominance distinguishes otomycosis from bacterial OE. Predisposing factors: prolonged topical antibiotic use, humid climates, immunosuppression, diabetes. Diagnosed by microscopy (KOH mount) showing hyphae and conidia.
Malignant (necrotising) otitis externa: A misnomer — not truly malignant, but named for its potentially fatal behaviour. Pseudomonas aeruginosa infection in the EAC of an elderly diabetic or immunocompromised patient (HIV, haematological malignancy) that spreads beyond the EAC skin into the skull base via Santorini's fissures. The pathognomonic otoscopic finding is granulation tissue at the floor of the EAC at the bony-cartilaginous junction. Clinically: severe unremitting otalgia out of proportion to apparent local disease, profound tenderness, systemic features. As it tracks along the skull base, it damages cranial nerves in sequence — CN VII (facial palsy) first, then CN IX–XII (as the jugular foramen is involved). Mortality without treatment was historically >50%; with prolonged IV anti-pseudomonal antibiotics, mortality is significantly reduced.
Wax impaction (cerumen impaction): Accumulation of cerumen in the EAC causing conductive hearing loss ± otalgia ± tinnitus. Most common cause of adult-onset conductive hearing loss. Predisposing factors: cotton bud use (pushes wax deeper), narrow or tortuous canals, hearing aid use, use of ear drops that dry cerumen. Diagnosed by otoscopy (brown or black plug obscuring the TM). Treatment: softening with olive oil or sodium bicarbonate drops for several days followed by syringing (if no TM perforation) or microsuction.
Keratosis obturans: An uncommon condition in which abnormal accumulation of desquamated keratin fills and expands the bony EAC, causing bony erosion and a widened canal. Distinct from EAC cholesteatoma (which causes localised bony erosion at one site, not diffuse canal widening). Presents with conductive hearing loss and occasional pain. Treatment: regular microsuction under otomicroscopy.
EAC exostoses and osteomata: Exostoses are bilateral, multiple, smooth, broad-based bony projections from the anterior and posterior walls of the bony EAC, caused by repeated cold-water exposure (common in swimmers and surfers — 'surfer's ear'). They narrow the canal progressively, predisposing to wax impaction and OE. An osteoma is a solitary, pedunculated, unilateral bony projection — less directly related to cold water. Symptomatic exostoses or osteomata are treated surgically (canalplasty).
SELF-CHECK
A 70-year-old man with type 2 diabetes mellitus presents with four weeks of severe right ear pain unresponsive to topical ear drops. On otoscopy, granulation tissue is visible at the floor of the right EAC at the bony-cartilaginous junction. The most likely diagnosis and the organism responsible is:
A. Chronic otitis externa caused by Staphylococcus aureus
B. Malignant otitis externa caused by Pseudomonas aeruginosa
C. Otomycosis caused by Aspergillus niger
D. Keratosis obturans with secondary infection
Reveal Answer
Answer: B. Malignant otitis externa caused by Pseudomonas aeruginosa
This is malignant (necrotising) otitis externa: the triad of elderly diabetic + severe otalgia unresponsive to topical treatment + granulation tissue at the EAC floor at the bony-cartilaginous junction is pathognomonic. The causative organism is Pseudomonas aeruginosa, which tracks along Santorini's fissures into the skull base. Chronic OE would show diffuse EAC skin thickening without the granulation tissue at this specific anatomical junction. Aspergillus otomycosis produces characteristic black spore heads and itching rather than severe pain. Keratosis obturans causes diffuse bony EAC expansion without granulation tissue.
Principles of Management of External Ear Diseases
Management of external ear diseases follows the general ENT principle: treat the underlying cause, not the symptom. The specific approach varies substantially across conditions, and knowing which conditions require systemic versus topical treatment, and which require urgent referral or hospital admission, is the key clinical competency.
Haematoma auris:
The time-critical intervention is drainage within 48–72 hours of injury, before the haematoma organises into fibrocartilaginous tissue. Technique: aspiration with a wide-bore needle or incision and drainage under local anaesthesia, followed immediately by a pressure bandage or suturing through-and-through to obliterate the potential space and prevent re-accumulation. If re-accumulation occurs despite pressure, a bolster stitch (dental roll or silicone sponge tied across both surfaces of the pinna) maintains compression. Cosmetically disfiguring established cauliflower ears require reconstructive surgery.
Perichondritis:
Early and aggressive systemic antibiotic therapy is essential to prevent cartilage necrosis. Ciprofloxacin (oral or intravenous depending on severity) is the drug of choice because of its reliable anti-Pseudomonal activity and good cartilage penetration. A fluctuant abscess requires drainage. If there is established cartilage necrosis, debridement of necrotic cartilage under general anaesthesia may be required, followed by reconstruction. Prevention: avoid ear piercing through cartilage (pierce through the lobule only); perioperative antibiotics for ear surgery.
Keloid:
Initial treatment: intralesional corticosteroid injections (triamcinolone acetonide) — reduce keloid volume. Surgical excision alone has a very high recurrence rate (>50–80%) and should not be performed without adjuvant treatment. Adjuvant options after excision: repeat intralesional steroids, silicone sheeting, pressure therapy, or low-dose radiotherapy in refractory cases.
Acute diffuse otitis externa:
The treatment sequence is: aural toilet first, then topical drops. Aural toilet — suctioning or dry mopping the canal under otomicroscope or good illumination — removes the debris and discharge that would otherwise prevent drops from penetrating to the affected skin. After aural toilet, topical antibiotic-steroid combination drops are instilled: ciprofloxacin 0.3% + hydrocortisone 1%, or gentamicin + betamethasone drops, for 7–10 days. If the canal is severely oedematous and drops cannot penetrate, an ear wick (Pope wick or glycerine-ichthammol ribbon gauze inserted into the canal) delivers medication via capillary action. The wick is removed after 48–72 hours once oedema subsides. Analgesics (NSAIDs ± paracetamol) for pain. Avoid water entry (ear plug during bathing). Systemic antibiotics are added only if cellulitis extends beyond the EAC or if the patient is diabetic or immunocompromised.
Otomycosis:
Aural toilet to remove all fungal debris is mandatory — topical antifungals cannot penetrate fungal mats. After thorough cleaning under microscopy, topical clotrimazole 1% solution is applied to the EAC for 2–4 weeks; alternatives include nystatin drops (preferred for Candida) or boric acid solution. Systemic antifungals (itraconazole, fluconazole) are reserved for severe cases or immunocompromised patients. Predisposing topical antibiotic use should be stopped if safe to do so.
Malignant (necrotising) otitis externa:
This is a medical emergency requiring hospital admission.
- Intravenous anti-pseudomonal antibiotics for 6–8 weeks: ciprofloxacin (oral bioavailability >80% — can often be used orally) or piperacillin-tazobactam IV ± aminoglycoside for severe cases. Oral ciprofloxacin 750 mg twice daily is an acceptable regimen for less severe cases with good oral tolerance.
- Aggressive glycaemic control in diabetics: a blood glucose >10 mmol/L impairs neutrophil function and antibiotic efficacy.
- Aural toilet to remove granulation tissue and improve drug delivery.
- Surgical debridement is required for devitalised or necrotic bone; however, extensive surgery is avoided in the acute phase — the primary treatment is medical.
- Regular cranial nerve assessment during treatment.
- Response monitoring: gallium-67 scan (correlates with active infection), ESR, CRP, clinical improvement in pain and granulation tissue.
Wax impaction:
Soften with olive oil drops (preferred) or 5% sodium bicarbonate drops nightly for 3–5 days, then irrigation (syringing with warm water at body temperature, directed at the posterosuperior EAC wall). Contraindications to syringing: perforated TM, history of TM surgery, only-hearing ear. In these cases: microsuction (ENT referral). Manual removal with a Jobson Horne probe or wax curette by a trained clinician is an alternative.
EAC exostoses:
Small asymptomatic exostoses: observe. Symptomatic exostoses causing recurrent OE or conductive hearing loss: surgical canalplasty (drill out the bone) — a specialist ENT procedure requiring referral.
SELF-CHECK
After aural toilet in a patient with acute diffuse otitis externa, the canal is found to be very swollen and oedematous, making it impossible to insert drops adequately. The most appropriate next step is:
A. Start oral antibiotics and discontinue topical treatment
B. Insert an ear wick (Pope wick or glycerine-ichthammol ribbon gauze) into the canal
C. Perform myringotomy to relieve pressure
D. Refer immediately to ENT for CT temporal bone
Reveal Answer
Answer: B. Insert an ear wick (Pope wick or glycerine-ichthammol ribbon gauze) into the canal
When the EAC is too oedematous for topical drops to penetrate, an ear wick (Pope wick or glycerine-ichthammol ribbon gauze inserted into the canal) delivers topical antibiotic-steroid medication by capillary action. The wick acts as a vehicle to hold the drops in contact with the swollen canal walls. Oral antibiotics alone are insufficient for OE without aural toilet and topical therapy. Myringotomy is not indicated in OE (which is a disease of the EAC, not the middle ear). CT is not indicated for uncomplicated OE — it is reserved for suspected malignant OE with skull base involvement.
CLINICAL PEARL
In malignant otitis externa, the severity of pain is almost always disproportionate to the initial otoscopic appearance. The diabetic patient who returns repeatedly complaining of ear pain despite topical drops, especially if there is granulation tissue at the bony-cartilaginous junction of the EAC floor, has malignant OE until proven otherwise. The absence of a visible large abscess or gross destruction is not reassuring — the disease is spreading subcutaneously along the skull base. The rule: in any elderly diabetic with unrelenting otalgia not responding to topical treatment, diagnose malignant OE first and exclude it by CT + nuclear imaging, not by continued topical treatment while awaiting a more dramatic presentation.
Self-Assessment
Test your recall across the key clinical and management facts from this module. The ability to apply these facts accurately in a clinical setting — not just recall them in isolation during a quiet study session — is precisely what the NMC competency assessment examines. Research on retrieval practice consistently shows that attempting answers without notes, even when you get them wrong, produces significantly better long-term retention than passive re-reading. The five questions below cover the full range of this SDL, from anatomical reasoning through diagnostic pattern recognition to management decisions and contraindications. For each question, commit to an answer before reading on. If you get it right, note why — identify the clinical feature or anatomical fact that anchored the correct answer. If you get it wrong, return to the specific section that covers that point, read it with the question as your guide, and re-attempt the question without looking at the answer. This active approach, repeated across all your ENT modules, is the most efficient way to build a durable factual foundation for your MBBS examinations and your clinical practice.
- A pinna swelling after trauma spares the lobule. What is the diagnosis, and why does the lobule escape — i.e., what is the anatomical reason?
- Name the organism most commonly responsible for (a) acute diffuse OE, (b) malignant OE, and (c) otomycosis. What microscopy finding confirms fungal OE?
- A patient has had a wax impaction treated by syringing. The patient mentions they had a tympanoplasty two years ago. Was syringing safe in this patient? What should have been done instead?
- Describe the pathognomonic otoscopic finding of malignant OE. What cranial nerve palsy appears first as the disease spreads, and why?
- What is the first step in treating acute diffuse OE — aural toilet or topical drops? Why does the order matter?
If you cannot state the anatomical reason for lobule-sparing in perichondritis (the lobule has no cartilage, therefore no perichondrium, therefore no perichondrial blood supply to infect), return to the anatomy section. If you cannot name the malignant OE organism and its drug of choice (Pseudomonas aeruginosa; ciprofloxacin), re-read the management section before your examination.