Page 1 of 17
EN4.1 | Otalgia — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with otalgia, distinguishing primary from referred pain
- Describe the clinical features and sensory nerve pathways that explain referred otalgia
- Choose appropriate investigations for a patient with otalgia, including those to exclude occult malignancy
- Describe the principles of management of the common causes of otalgia
INSTRUCTIONS
Otalgia — pain in the ear — is one of the most common ENT complaints and is frequently mismanaged because clinicians examine only the ear and miss the true source of pain. In adults, referred otalgia from the throat, teeth, jaw, or larynx is at least as common as primary ear disease, and unexplained otalgia in a middle-aged or elderly adult must raise the alarm for occult head-and-neck malignancy. This module builds the diagnostic framework you need to work through any otalgia case systematically from history to management.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat, 8th ed., Ch. 5: Symptoms of Ear Disease (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat and Head-Neck Surgery, 3rd ed., Ch. 4: Clinical Evaluation of Ear Diseases (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 3, Ch. 236: Otalgia (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male farmer presents to your outpatient clinic with a four-week history of pain in the left ear. He has no hearing loss, no discharge, no dizziness. He drinks alcohol daily and smokes bidis. On otoscopy, both ear canals are clear, both tympanic membranes are intact and normal in appearance. You reassure him it is 'nothing serious' and prescribe analgesics. He returns three months later with the same pain, now worsening, and has noticed a lump in his left neck. A biopsy of the neck node confirms squamous cell carcinoma. The primary turns out to be a hypopharyngeal carcinoma. Could this outcome have been prevented?
WHY THIS MATTERS
Otalgia is among the top five presenting complaints in ENT outpatient clinics and a frequent reason for primary care visits across all age groups. In children, acute otitis media is the overwhelmingly common cause and is easily diagnosed. In adults, however, the picture is strikingly different: up to 50% of adults presenting with ear pain have no primary ear pathology on careful examination (Dhingra). The pain arises in a distant site — the throat, jaw, teeth, larynx, or cervical spine — and is referred to the ear via shared nerve pathways. This distinction has profound management implications. Missing referred otalgia means missing its cause, which in an adult smoker or drinker must include head-and-neck malignancy until proven otherwise. The NMC EN4.1 competency expects you to elicit, document, and present a structured otalgia history, demonstrate clinical examination findings, choose investigations, and describe management principles — all of which depend on a clear understanding of the primary-versus-referred framework.
RECALL
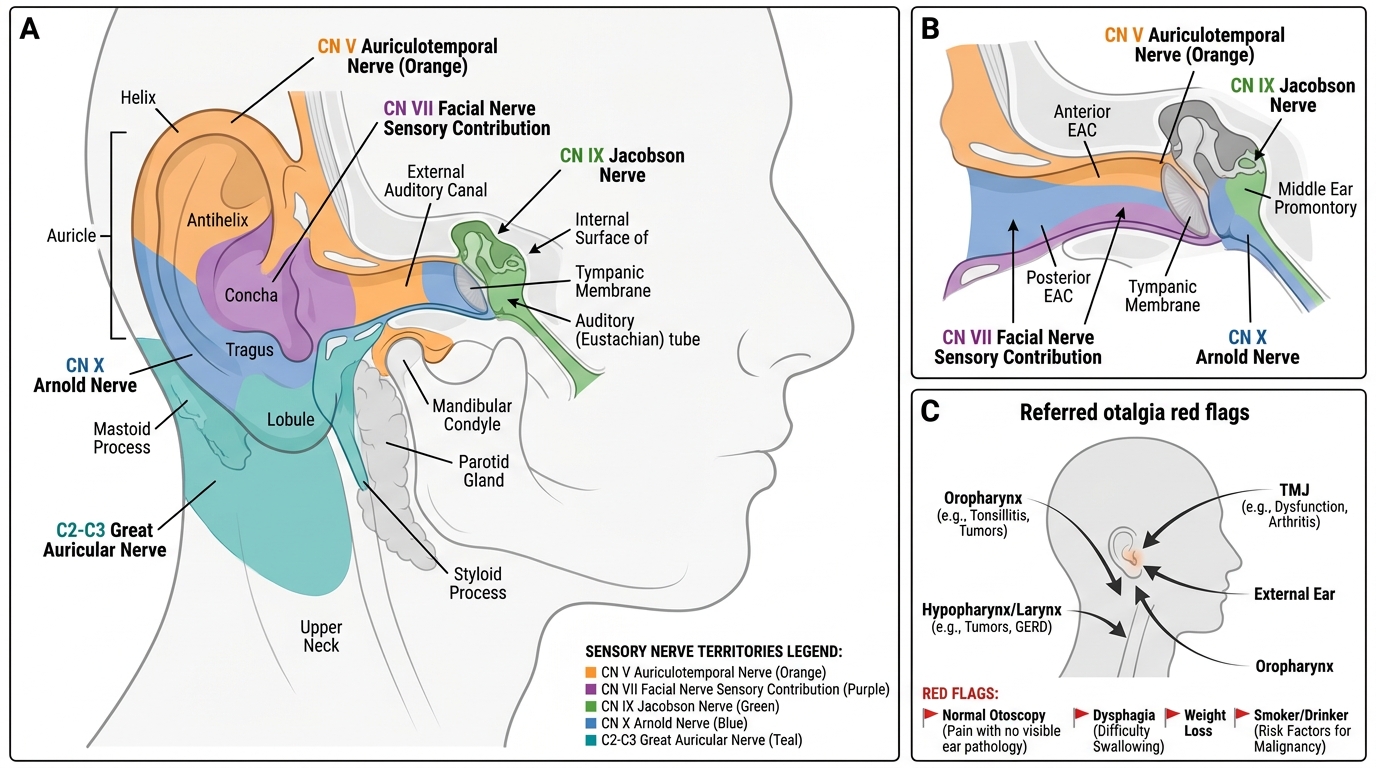
Recall from your first-year anatomy sessions the cranial nerves that supply sensory fibres to the ear and its surrounding structures. The ear has an unusually rich and overlapping sensory supply because several different cranial and cervical nerves converge on it. The auricular branch of the trigeminal nerve (CN V₃), specifically the auriculotemporal nerve, supplies the anterior and superior external auditory canal (EAC) and the anterior auricle. The facial nerve (CN VII) carries sensory fibres to the posterior EAC via its auricular branch. The glossopharyngeal nerve (CN IX) supplies the middle ear promontory and tympanic cavity via Jacobson's nerve (the tympanic branch), and contributes to the concha and lower auricle. The vagus nerve (CN X) supplies the posterior EAC and posterior auricle via Arnold's nerve (the auricular branch of CN X). Finally, the great auricular nerve — a branch of the cervical plexus arising from spinal roots C2–C3 — supplies the lower half of the auricle and the skin over the mastoid region. This multi-nerve supply means that any pathology along these nerves, anywhere from the brainstem to the peripheral target organ, can be perceived as ear pain.
Clinical Presentation of Otalgia
A well-structured history is the most important single step in evaluating otalgia. The history must determine whether the pain arises from the ear itself (primary/otogenic otalgia) or is transmitted from a distant site (referred/non-otogenic otalgia). This distinction guides every subsequent examination and investigation step.
In taking the history, the clinician should characterise the pain using standard parameters — onset, duration, character (dull, sharp, throbbing, burning), severity, radiation, aggravating and relieving factors, and associated symptoms. The associated symptoms listed below are especially revealing because each one tends to localise the source of pain to a specific anatomical region. When you see discharge, you think external or middle ear; when you see dysphagia in an adult smoker, you think pharynx or larynx; when you see jaw clicking, you think temporomandibular joint. Reading the associated symptoms through this anatomical lens at the bedside is the clinical skill that separates a thorough ENT history from a generic "where does it hurt" consultation.
- Discharge (otorrhoea): presence of discharge strongly suggests a primary ear cause (otitis externa, acute or chronic otitis media, cholesteatoma). The character of discharge is itself diagnostic — watery discharge in malignant otitis externa or CSF otorrhoea; purulent discharge in AOM or CSOM; foul-smelling discharge with bone erosion points to cholesteatoma.
- Hearing loss: primary ear pathology (middle or inner ear disease) frequently coexists with pain; referred otalgia does NOT produce hearing loss.
- Tinnitus and vertigo: inner ear involvement. Tinnitus and low-frequency fluctuating hearing loss with vertigo suggest Meniere's disease; acute vertigo after ear pain suggests labyrinthitis secondary to otitis media.
- Trismus, dysphagia, odynophagia, dysphonia: these symptoms point away from the ear toward the oral cavity, pharynx, or larynx — strongly suggesting referred otalgia. Trismus suggests a temporomandibular joint (TMJ) or peritonsillar/pterygomandibular pathology. Dysphagia + otalgia in an older adult with smoking/alcohol history must be treated as oropharyngeal or hypopharyngeal malignancy until proven otherwise.
- Clicking or pre-auricular pain on jaw movement: TMJ dysfunction (Costen's syndrome) — pain reproduced by jaw movement or on palpating the TMJ is diagnostic.
- Dental pain, recent dental work: referred otalgia via the auriculotemporal branch of CN V.
- Neck pain or stiffness: cervical spine pathology referred via the great auricular nerve (C2–C3).
Key red flags in the history that must never be missed:
1. Otalgia in a middle-aged or older adult with no primary ear pathology on otoscopy — this is referred otalgia until proven otherwise.
2. Otalgia + weight loss + dysphagia/dysphonia in a smoker/drinker — must exclude head-and-neck malignancy.
3. Otalgia in a child with persistent fever, severe illness, or high-grade hearing loss — consider complications of AOM (mastoiditis, intracranial extension).
4. Unilateral pulsatile tinnitus + otalgia — consider glomus tumour or vascular anomaly.
The social history should always include tobacco use (smoking, chewing), alcohol consumption, and occupational exposures. Both tobacco and alcohol are major risk factors for squamous cell carcinoma of the upper aerodigestive tract — the most important referred otalgia cause to exclude in adults.
Anatomy and Neuroanatomy Relevant to Otalgia
The rich and overlapping sensory nerve supply of the ear is the anatomical basis for referred otalgia. When a structure remote from the ear is diseased, pain impulses travel centripetally along the nerve that supplies both the diseased structure and the ear — and the brain, which has learned to attribute pain in that nerve's territory to the ear, perceives the sensation as otalgia.
Five nerve pathways are clinically important:
1. Auriculotemporal branch of the trigeminal nerve (CN V₃):
This branch of the mandibular division of CN V supplies the anterior wall of the EAC, the tragus, and the anterior auricle. It also carries sensory fibres from the TMJ, the lower molars, the parotid gland, and the temporal scalp. Dental caries or abscess (especially lower molars), TMJ dysfunction (Costen's syndrome — articular disk displacement or osteoarthritis of the TMJ), and parotid gland pathology all refer pain to the ear via this pathway. TMJ otalgia is classically reproduced or worsened by jaw movement — chewing, opening wide, clenching — and is associated with pre-auricular tenderness.
2. Facial nerve (CN VII) — auricular branch (Ramsay Hunt syndrome pathway):
The auricular branch of the facial nerve supplies the posterior EAC skin and the conchal bowl of the auricle. In herpes zoster oticus (Ramsay Hunt syndrome), the varicella-zoster virus reactivates in the geniculate ganglion of CN VII, causing severe otalgia, vesicular eruption in the EAC and concha, peripheral facial palsy, and sometimes sensorineural hearing loss. This is one of the most painful ear conditions encountered in clinical practice.
3. Jacobson's nerve — tympanic branch of CN IX:
Jacobson's nerve is the tympanic branch of the glossopharyngeal nerve (CN IX). It forms the tympanic plexus on the promontory of the middle ear, supplying the middle ear mucosa. CN IX also supplies the tonsillar fossa, the posterior one-third of the tongue, the oropharyngeal mucosa, and part of the soft palate. Consequently, tonsillitis, peritonsillar abscess, oropharyngeal carcinoma, and lingual tonsil pathology all refer pain to the ear via CN IX. Otalgia after tonsillectomy — a common complaint in the first post-operative week — is referred via this pathway.
4. Arnold's nerve — auricular branch of CN X (vagus):
Arnold's nerve is the auricular branch of the vagus (CN X). It supplies the posterior wall and floor of the EAC and the adjacent posterior auricle. CN X also supplies the laryngopharynx, the hypopharynx, the cervical oesophagus, and the infrahyoid larynx. This is the critical pathway for referred otalgia from laryngeal carcinoma and hypopharyngeal carcinoma — malignancies of the lower pharynx and larynx refer pain to the ear via Arnold's nerve. This nerve also mediates the Arnold's nerve reflex (ear-cough reflex) — stimulation of the posterior EAC (e.g., during syringing or insertion of an earbud) can provoke a cough or even syncope.
5. Great auricular nerve (C2–C3, cervical plexus):
The great auricular nerve, arising from spinal roots C2–C3, supplies the lower auricle, the skin over the mastoid, and the adjacent parotid region. Cervical spondylosis, cervical disc prolapse (especially at C2–3 or C3–4 levels), and posterior triangle lymphadenopathy refer otalgia via this pathway. The pain is typically described as dull and aching, associated with neck pain or stiffness, and worsened by neck movement.
Sensory Nerve Supply of the Ear and Referred Otalgia
SELF-CHECK
A 55-year-old man presents with a three-week history of right-sided otalgia. On otoscopy, the ear canal is clear and the tympanic membrane is normal. He has mild dysphagia and has lost 4 kg over two months. He smokes 20 cigarettes per day and drinks alcohol daily. The most appropriate next step is:
A. Prescribe NSAID analgesics and reassure the patient
B. Perform a full oral cavity, oropharyngeal, and laryngopharyngeal examination to exclude malignancy
C. Refer for audiometry to assess middle ear function
D. Treat empirically for otitis externa
Reveal Answer
Answer: B. Perform a full oral cavity, oropharyngeal, and laryngopharyngeal examination to exclude malignancy
This presentation — unexplained unilateral otalgia with normal otoscopy + dysphagia + weight loss in a middle-aged male smoker-drinker — is a classic referred otalgia red flag for hypopharyngeal or oropharyngeal malignancy until proven otherwise. The next step is a full H&N examination including mirror laryngoscopy or fibreoptic nasopharyngolaryngoscopy. Reassurance and symptomatic treatment are dangerous. Audiometry assesses hearing and middle ear function but does not examine the throat or larynx. Empiric treatment for otitis externa is incorrect when the EAC and TM are normal.
ENT Examination and Investigation in Otalgia
The examination protocol for otalgia is broader than for any other ENT complaint precisely because the cause may lie anywhere from the ear to the larynx. A systematic approach in five parts ensures no cause is missed.
Part 1 — Otoscopic examination of both ears:
Begin with a thorough otoscopic examination of both ears. Inspect the auricle, the pre- and post-auricular skin (vesicles in Ramsay Hunt syndrome), the EAC (canal skin — erythema, oedema, discharge, tenderness on tragal pressure in otitis externa), and the tympanic membrane (bulging, opaque, perforated, retracted, cholesteatoma debris in the pars flaccida). A normal otoscopic examination in a patient with significant otalgia immediately shifts suspicion to referred causes.
Part 2 — Oral cavity and oropharynx examination:
With adequate light and a tongue depressor, inspect the oral cavity (teeth, gums, tongue, floor of mouth), the tonsillar fossae (erythema, tonsillar enlargement, peritonsillar bulge, ulceration), the soft palate, the posterior pharyngeal wall, and the base of the tongue. Any ulcer in the oral cavity or oropharynx in an adult with otalgia must be biopsied.
Part 3 — TMJ and parotid gland assessment:
Palpate the TMJ bilaterally while asking the patient to open and close the mouth. Tenderness, clicking, or restricted mouth opening suggests TMJ dysfunction. Palpate the parotid gland for enlargement or tenderness (parotitis, parotid tumour).
Part 4 — Indirect laryngoscopy / fibreoptic nasopharyngolaryngoscopy:
This is the critical step that is most often omitted. Mirror laryngoscopy (or fibreoptic nasopharyngolaryngoscopy) must be performed in every adult with unexplained otalgia to inspect the nasopharynx, hypopharynx, piriform fossae, postcricoid region, and larynx. Hypopharyngeal and laryngeal malignancies characteristically present as painless masses (the malignancy itself is relatively insensate) but refer pain to the ear — the primary lesion can be missed without direct visualisation.
Part 5 — Neck examination:
Palpate the cervical lymph nodes systematically (levels I–VI). A palpable neck node in an adult with otalgia and no primary ear pathology is a malignancy until proven otherwise. Palpate the posterior triangle for tenderness (cervical lymphadenopathy) and assess range of neck movement (cervical spondylosis).
Investigations — guided by examination findings:
- Pure tone audiometry: if hearing loss is present — establishes whether the hearing loss is conductive, mixed, or sensorineural, pointing to middle ear or inner ear pathology.
- Tympanometry: assesses middle ear pressure and tympanic membrane compliance — useful if AOM or middle ear effusion is suspected.
- CT of the temporal bones: if mastoiditis, skull base osteomyelitis, cholesteatoma, or middle ear mass is suspected.
- CT or MRI of the neck and thorax: if referred otalgia from a pharyngeal, laryngeal, or oesophageal lesion is suspected — defines the extent of disease.
- Contrast-enhanced CT neck: for suspected parapharyngeal or parotid pathology, or lymphadenopathy.
- Panoramic dental X-ray (OPG): if dental abscess or lower molar pathology is suspected.
- Fibreoptic nasopharyngolaryngoscopy: for direct visualisation of hypopharynx and larynx in unexplained adult otalgia.
- ESR, CRP, blood count: if systemic causes (vasculitis, infectious mononucleosis) are in the differential.