Page 10 of 17
EN4.9 | Wax Removal Technique — SDL Guide
Learning Objectives
- State the clinical indications for wax removal and correctly identify patients in whom syringing is contraindicated
- Name the instruments used for each wax removal technique and describe the physical principles underlying each method
- Demonstrate the correct step-by-step technique for ear syringing, microsuction, and manual wax removal in a simulated environment
- Describe the expected findings and potential complications after wax removal and outline appropriate follow-up
INSTRUCTIONS
Cerumen (wax) impaction is the single most common cause of primary care ear consultations in adults, yet wax removal is also one of the most frequently performed procedures incorrectly, causing complications ranging from ear infection to tympanic membrane perforation. The NMC EN4.9 competency requires you to demonstrate the correct technique for wax removal in simulation. More importantly, it requires you to know when NOT to syringe — the contraindications to syringing are a patient safety principle that every doctor performing ear procedures must have as an automatic reflex.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat, 8th ed., Ch. 6: External Ear; Wax Removal (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat and Head-Neck Surgery, 3rd ed., Ch. 6: Wax and Foreign Body in Ear (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 3, Ch. 238: Wax and Foreign Bodies (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman visits a general practitioner complaining of gradual hearing loss in the left ear for two weeks. She reports no pain, no discharge, and no vertigo. The GP looks in the ear and sees a large brown wax plug completely occluding the left EAC. Without taking any further history, the GP fills a large syringe with tap water from the basin and syringes the ear vigorously. The patient cries out in pain; immediately after the procedure, she is dizzy and nauseated. When the GP looks in the ear with an auriscope, the wax has been removed, but there is fresh blood in the canal. On referral to ENT, a new perforation of the pars tensa is identified. The patient is upset. What two mistakes did the GP make before even picking up the syringe?
WHY THIS MATTERS
Wax impaction is the single most common cause of adult primary care ear consultations in India and globally, accounting for more ENT-related primary care visits than any other condition (Dhingra). The majority of these patients can be managed safely by a trained primary care doctor. However, ear syringing — the most commonly performed wax removal procedure — carries a well-documented complication profile when performed without proper assessment: tympanic membrane perforation (if syringing is performed in an ear with an unsuspected perforation), external otitis (from water remaining in the canal), dizziness and nausea (from caloric stimulation with non-body-temperature water), and post-procedural pain (from trauma to the EAC skin). The ENT competency EN4.9 exists specifically because safe wax removal requires both the technical skill of the procedure and the clinical judgment to know who should not have it. Both components are tested in the NMC assessment.
RECALL
Recall the anatomy of the external auditory canal: the EAC is approximately 2.5 cm long and has an S-shaped curve in the horizontal plane. The outer one-third is cartilaginous, contains ceruminous glands (modified apocrine glands producing cerumen), and is lined by thick, mobile skin. The inner two-thirds is bony, with thin periosteum-adherent skin and no glands. To straighten the natural curve of the EAC for instrument access, the pinna must be pulled posterosuperiorly in adults (upward and backward) — this straightens the cartilaginous portion by pulling the cartilage upward. In infants the traction is downward and backward (the canal curves differently in infancy). Recall also that the tympanic membrane (TM) sits at the inner end of the EAC at an oblique angle (not perpendicular) — the anterior wall of the EAC is longer than the posterior wall. The TM is best viewed with the otoscope beam directed slightly anteriorly. The handle of the malleus runs from the umbo to the lateral process, with the cone of light emanating anteroinferiorly in the normal TM.
Clinical Indication and Relevance of Wax Removal
The decision to remove wax should be based on whether the wax is causing symptoms or preventing adequate examination — not on the mere presence of wax in the canal. Cerumen serves a natural protective function: it is acidic (pH 4–5), antibacterial, antifungal, and acts as a water-repellent barrier for the delicate bony EAC skin. Removing asymptomatic wax that is not impacting function is unnecessary and potentially harmful. The clinical indication must therefore be carefully established before any wax removal procedure is initiated.
Indications for wax removal:
Wax should be removed when it causes: (1) Hearing loss — the most common presenting complaint; a large plug completely occluding the EAC can cause a 30–40 dB conductive hearing loss; (2) Otalgia — pressure from impacted wax against the bony EAC skin; (3) Tinnitus — from partial EAC occlusion; (4) Vertigo — rarely, from impacted wax pressing on the TM; (5) Obstruction of TM visualisation — in a patient requiring accurate otoscopy for clinical assessment (e.g., recurrent otitis media, otalgia, audiological assessment). When wax is asymptomatic and does not obstruct examination, leave it alone.
Pre-procedure assessment — mandatory before any wax removal:
Before any wax removal technique is performed, the clinician MUST take a brief but targeted history to identify contraindications. This assessment takes two to three minutes and is not optional. Ask:
1. Has the patient ever had ear surgery? (tympanoplasty, mastoidectomy, grommets/ventilation tubes) — these ears must not be syringed.
2. Has the patient ever had a perforated eardrum? — past or present perforation is a contraindication to syringing.
3. Does the patient have only one hearing ear? — syringing a single-hearing ear risks leaving the patient profoundly deaf if a complication occurs; refer to ENT for microsuction.
4. Does the patient have ear pain, discharge, or a history of cleft palate? — these suggest active ear disease or abnormal Eustachian tube function; syringe with caution or refer.
5. Has the patient had an unsuccessful previous syringe or a bad reaction? — suggests difficulty that may warrant ENT referral.
Wax that is completely dry and hard (impacted wax, often black) should be softened first with cerumenolytic drops (olive oil, 5% sodium bicarbonate drops) for 3–5 days before attempting syringing. Attempting to syringe hard, impacted wax without prior softening is ineffective and painful.
Instruments and Principles of Wax Removal
Each wax removal technique uses different instruments and operates on different physical principles. Understanding both dimensions — what the instrument is, and why it works — is what allows you to adapt your technique to the individual patient's canal anatomy and wax consistency.
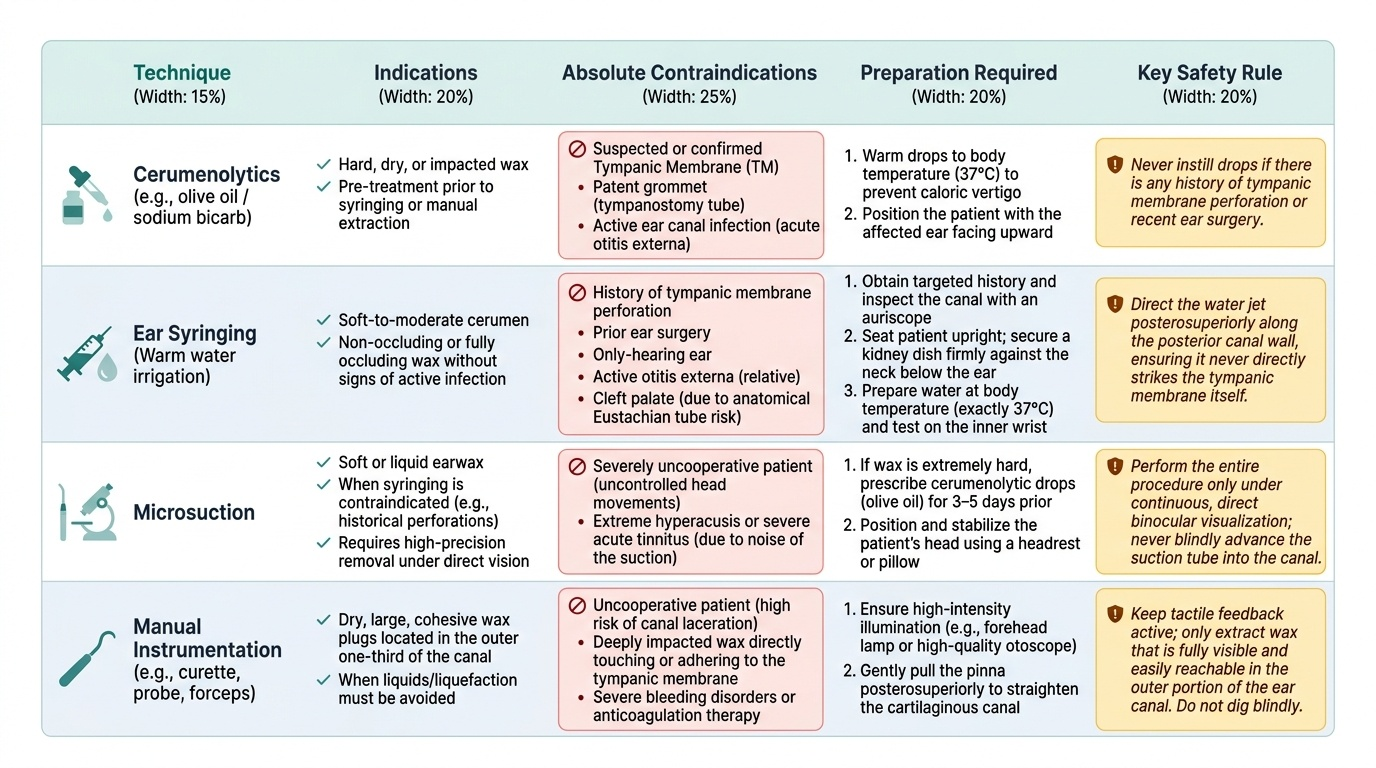
Cerumenolytics (chemical softening):
Olive oil drops are the preferred first-line cerumenolytic for most patients. They work by softening and lubricating the wax plug, allowing it to fragment and migrate laterally. The dose is 2–3 drops instilled into the EAC (with the patient lying on their side, affected ear up) twice daily for 3–5 days before syringing. Sodium bicarbonate 5% drops (available as proprietary preparations) act by breaking up wax via chemical emulsification of the fatty components of cerumen. Hydrogen peroxide 3% drops (Otex) also effervesce and soften cerumen — they are not preferred in cases of otitis externa as the peroxide may irritate inflamed skin. Cerumenolytics alone are sometimes sufficient to allow spontaneous migration of the wax plug; in some patients, this is all that is needed.
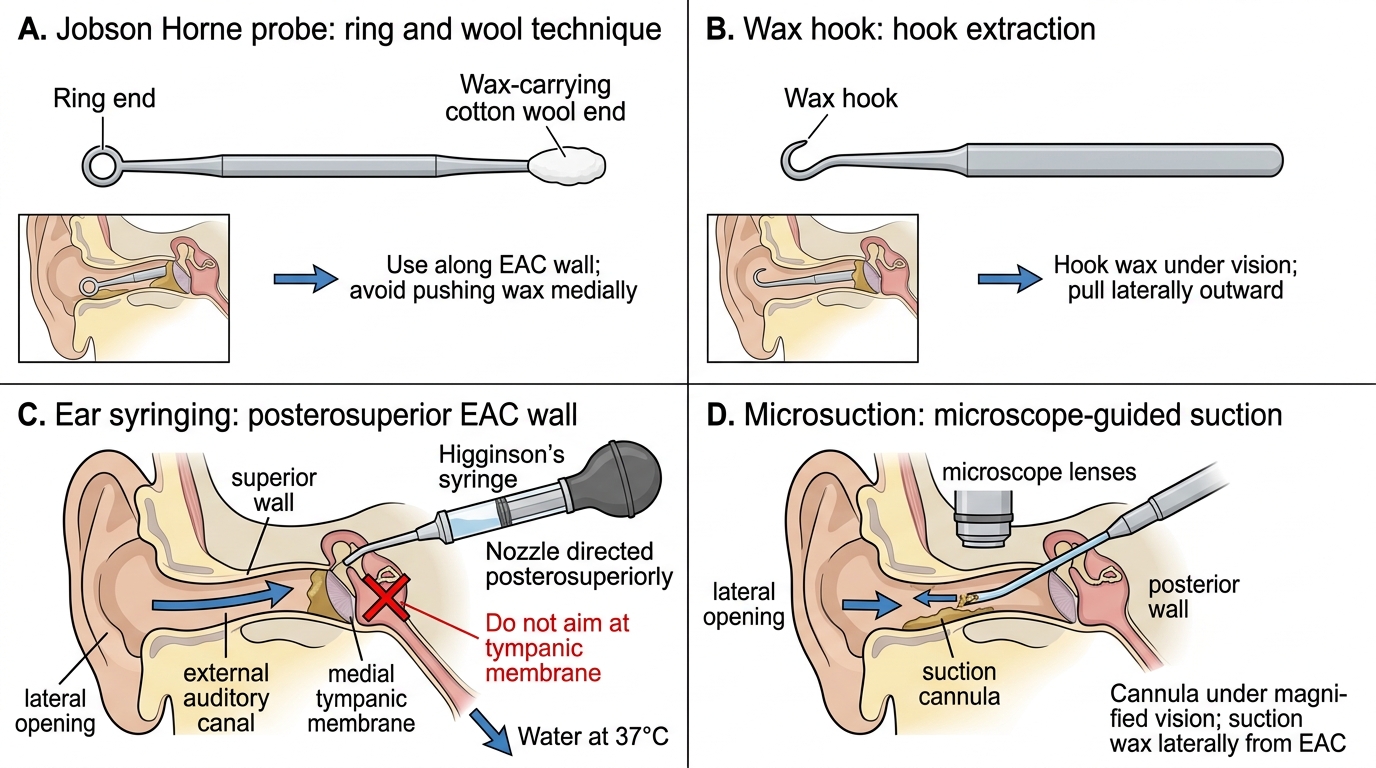
Syringing (warm water irrigation):
The standard instrument is the Higginson's syringe (a large bulb syringe) or an electronic ear irrigator. The principle is hydraulic: a stream of water directed against the posterosuperior wall of the EAC creates a jet of fluid that passes behind the wax plug and dislodges it by hydraulic pressure. The critical physical principle is water temperature: the water MUST be at body temperature (37°C). Cold water entering the EAC creates a temperature differential in the endolymph of the adjacent horizontal semicircular canal; this causes convection currents in the endolymph → stimulation of the hair cells → nystagmus and vertigo (the physiological basis of the caloric test). Hot water causes the same effect in the opposite direction. Caloric stimulation with non-body-temperature water during syringing causes sudden, severe vertigo, nausea, and potentially vomiting — a preventable complication of incorrect water temperature.
Microsuction:
Microsuction uses low-pressure suction through a fine metal cannula under direct vision via an otomicroscope or binocular loupes. It does not use water and therefore cannot cause caloric stimulation, introduce infection via water, or risk TM perforation from a water jet directed incorrectly. It is considered the gold standard and safest technique for wax removal. It requires either an otomicroscope (ENT clinic) or binocular Omni loupes (available in trained primary care). Microsuction is the technique of choice when syringing is contraindicated.
Manual instrumentation:
The Jobson Horne probe is a double-ended instrument: one end is a small blunt-edged wax hook (for engaging behind soft wax and drawing it out), and the other end is a carrier for cotton wool (for aural toilet). A wax hook or ring curette can also be used under direct vision via a headlight and auriscope. Manual instrumentation requires firm but extremely gentle manipulation to avoid trauma to the delicate bony EAC skin. It is most useful for soft, adherent, or posteriorly-placed wax that cannot be effectively irrigated.
Techniques for Ear Wax Removal
SELF-CHECK
A patient having ear syringing suddenly complains of severe dizziness, nausea, and nystagmus during the procedure. The most likely cause and the corrective action is:
A. The wax has been dislodged into the middle ear — stop and refer to ENT
B. The irrigation water was not at body temperature, causing caloric stimulation of the semicircular canal — stop syringing, allow patient to sit upright, ensure water is at 37°C before continuing
C. The patient has Meniere's disease that was not known before — stop permanently and refer
D. The water pressure was too high — reduce pressure and continue
Reveal Answer
Answer: B. The irrigation water was not at body temperature, causing caloric stimulation of the semicircular canal — stop syringing, allow patient to sit upright, ensure water is at 37°C before continuing
Sudden vertigo during ear syringing is the caloric effect: non-body-temperature water (too cold or too hot) creates a temperature gradient in the endolymph of the horizontal semicircular canal, inducing convection currents and vestibular stimulation — nystagmus and vertigo. The correct action is to stop syringing immediately, reassure the patient, allow symptoms to settle (usually within 2–5 minutes), check and correct the water temperature to 37°C before resuming. Wax cannot be dislodged into the middle ear via an intact TM. Pre-existing Meniere's is not the cause — the mechanism is physical (temperature), not pathological.
Procedure and Technique
The correct technique for each wax removal method is built from the anatomical principles of EAC curvature and the physical principles of each method reviewed in the previous section. These are not abstract facts but directly operational rules: the posterosuperior direction of the syringe jet follows from knowing that the TM sits at the far end of the canal and must not receive the direct water impact; the 37°C water temperature follows from understanding caloric physiology; the pinna traction posterosuperiorly follows from the shape of the cartilaginous EAC. Students who understand the reasons for each step execute the technique correctly under novel conditions; those who have memorised the steps without the reasoning make errors when anything differs from the textbook description. The sequence below presents each step with its anatomical or physical rationale, so that the procedure is understood rather than merely followed.
Provided image
Pre-procedure checklist (every patient, every time):
1. Take the targeted history (contraindications — perforation, surgery, only-hearing ear, active otitis, cleft palate).
2. Inspect the EAC with an auriscope: confirm the wax is impacted and is the source of the symptoms; check that the EAC skin is not inflamed (active otitis externa — a relative contraindication to syringing).
3. If the wax is hard and dry: prescribe cerumenolytic drops (olive oil) for 3–5 days and arrange a return appointment for syringing.
Technique — ear syringing (warm water irrigation):
Step 1 — Patient position: seat the patient upright; provide a kidney dish to hold against the neck below the ear to catch water and debris.
Step 2 — Fill the syringe with warm water: prepare water at body temperature (37°C). Test it on the inner aspect of your wrist — it should feel neutral (neither warm nor cold). Fill the Higginson's syringe or electronic irrigator.
Step 3 — Pinna traction: with your non-dominant hand, pull the pinna posterosuperiorly (upward and backward in adults) to straighten the EAC. This is essential — syringing without pinna traction leaves the canal curved and the jet does not reach the wax plug effectively.
Step 4 — Direct the jet: insert the nozzle gently (not deeply) into the EAC opening. Direct the jet of water toward the posterosuperior wall of the EAC — NOT directly at the TM. This posterior direction is critical: a jet directed straight at the TM can perforate it. The posterosuperior direction sends water past the superior margin of the wax plug, allowing the returning water stream to carry the wax out.
Step 5 — Apply gentle hydraulic pressure: deliver one or two gentle pulses of water. Do not use excessive force — if the wax is well-softened, gentle pressure is sufficient. Between pulses, withdraw the nozzle and let the patient tilt their head to drain water into the kidney dish.
Step 6 — Inspect after each pulse: after 2–3 pulses, use the auriscope to check whether wax fragments have been displaced. Continue until the TM is visible or wax has been removed. If wax is not shifting after 3–4 attempts despite prior softening, do not persist — refer for microsuction.
Step 7 — Post-procedure inspection: after wax removal, inspect the TM carefully. Confirm the TM is intact. Note the TM appearance (normal, bulging, retracted, perforated). If a new perforation is seen, document it immediately and refer.
Step 8 — Dry the canal: tilt the patient's head to drain residual water; gently mop with a dry cotton wool carrier on a Jobson Horne probe. Leaving water in the bony EAC predisposes to post-syringing otitis externa — the moist, slightly traumatised skin is an ideal bacterial growth medium.
Technique — microsuction:
Seat the patient. Use binocular loupes or an otomicroscope. Select a fine-calibre suction cannula (Frazier or Baron suction tube, size 3–5 French). Apply low suction (controllable via the suction port). Under direct visualisation, engage the suction tip against the outer surface of the wax plug and draw it laterally in short, controlled strokes. Never push the suction tip deeply without direct vision of the canal floor. Do not hold suction continuously in one position — the EAC skin can be traumatised by prolonged suction contact.
Technique — manual removal with Jobson Horne probe:
Under direct vision (headlight + auriscope or loupes), introduce the blunt ring end of the probe gently along the superior wall of the EAC, past the edge of the wax plug. Rotate the ring to engage behind the wax and draw it laterally with a gentle, slow, continuous motion. Never use a sharp scraping motion against the bony EAC skin. This technique is most useful for posteriorly-placed soft wax that water jets cannot dislodge.
SELF-CHECK
A 72-year-old man presents with gradual bilateral hearing loss. He has a history of left tympanoplasty performed 8 years ago. He has wax impaction in both ears confirmed by otoscopy. Which of the following is the correct management plan?
A. Syringe both ears with warm water simultaneously
B. Syringe the right ear (no surgical history); refer the left ear for microsuction (post-tympanoplasty ear)
C. Syringe both ears after a week of olive oil softening
D. Prescribe olive oil drops for both ears only; do not remove the wax
Reveal Answer
Answer: B. Syringe the right ear (no surgical history); refer the left ear for microsuction (post-tympanoplasty ear)
The left ear has a history of tympanoplasty (TM graft surgery) — syringing is absolutely contraindicated because the water jet could disrupt the graft or perforate a thinned or vulnerable TM repair site. The correct approach is: syringe the right ear (no surgical history; intact TM assumed) after confirming otoscopic TM integrity and applying olive oil drops first for softening; and refer the left ear to ENT for microsuction, which is safe in post-surgery ears as no water is used. Syringing the left ear regardless of surgical history is a patient safety error.