Page 7 of 29
EN4.14 | Conductive and Sensorineural Hearing Loss — SDL Guide
Learning Objectives
- Classify hearing loss into conductive, sensorineural, and mixed types based on clinical and audiometric findings
- Explain the anatomy and pathophysiology underlying each type of hearing loss
- Perform and interpret tuning-fork tests (Rinne, Weber, ABC) and relate them to audiometric findings
- Describe the clinical features and management of sudden sensorineural hearing loss (SSNHL) as an emergency
- Describe the clinical features, prevention, and management of noise-induced hearing loss (NIHL)
- Outline the principles of management including hearing aids and cochlear implantation
INSTRUCTIONS
Hearing loss is the most common sensory disability worldwide, affecting over 430 million people. As a final-year student you will encounter patients with hearing loss in nearly every clinical setting — not just ENT. This SDL integrates your audiological examination skills (tuning-fork tests, audiometry interpretation) with the clinical diagnosis of specific conditions. Special emphasis is placed on SSNHL (sudden hearing loss is an otological emergency requiring same-day assessment) and NIHL (a preventable occupational condition). Competency EN4.14 requires you to describe clinical features, investigations, and management of both CHL and SNHL including SSNHL and NIHL.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 3-4 (Hearing Loss and Audiometry) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 230-231 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients present to your ENT outpatient on the same morning. Patient A is a 65-year-old retired teacher with a 5-year history of gradually worsening hearing in both ears; his wife says he turns the television up very loud. Patient B is a 40-year-old construction worker who woke up this morning with no hearing in his right ear — he is terrified. Both have hearing loss, but the urgency, aetiology, and management could not be more different. How do you approach each patient systematically, and what test would you perform first at the bedside for each?
WHY THIS MATTERS
Hearing loss is estimated to affect over 430 million people globally and is the leading sensory disability causing communication impairment and social isolation. In India, the prevalence is approximately 6.3% — nearly 63 million people — with a disproportionate burden in occupational groups (factory workers, construction workers, musicians) and the elderly. The classification of hearing loss into conductive, sensorineural, and mixed types is not merely academic: the type determines the aetiology, the investigation pathway, and critically, whether the loss is reversible or permanent. Conductive losses are often surgically correctable; sensorineural losses are generally irreversible but manageable with amplification. Two specific entities — sudden sensorineural hearing loss (SSNHL) and noise-induced hearing loss (NIHL) — require special attention: SSNHL because it is an otological emergency where delayed treatment reduces recovery, and NIHL because it is entirely preventable but affects millions of Indian workers.
RECALL
Recall the normal sound conduction pathway: sound waves → pinna (concentrates) → external auditory canal → tympanic membrane (vibrates) → ossicular chain (malleus → incus → stapes footplate) → oval window → perilymph in the vestibule → basilar membrane of the cochlea (encodes frequency tonotopically) → inner hair cells (mechanical-to-electrical transduction) → VIII cranial nerve → cochlear nuclei in brainstem → auditory cortex. Conductive hearing loss arises when anything interrupts the pathway from the pinna to the oval window (outer or middle ear). Sensorineural hearing loss arises when there is damage to the cochlear hair cells, the eighth nerve, or the central auditory pathway. Recall also: the basal turn of the cochlea encodes high frequencies (4–8 kHz); the apex encodes low frequencies (250–500 Hz). Hair cells in the human cochlea do NOT regenerate once destroyed.
Clinical Presentation: How Hearing Loss Presents
Hearing loss is experienced and reported differently depending on its type, degree, and the patient's age and social context. The clinical history is the first and most important tool — a systematic approach to the hearing loss history helps distinguish conductive from sensorineural loss before any test is done.
Taking a systematic hearing loss history requires attention to several clinical dimensions, each of which maps to a specific aetiological category. The temporal profile of the loss — sudden versus gradual — is perhaps the single most clinically decisive question, because sudden onset mandates same-day investigation while gradual onset allows an elective workup. Unilaterality or bilaterality, associated ear symptoms, occupational exposure, medication history, and family history complete the picture. The following framework structures the history and links each question to its clinical reasoning:
- Onset and progression: sudden (hours-to-days) versus gradual (months-to-years)? Sudden SNHL is an emergency; gradual bilateral loss in an elderly patient is usually presbyacusis or NIHL.
- Unilateral or bilateral: unilateral loss warrants greater concern for a structural cause (acoustic neuroma, SSNHL, CSOM).
- Associated symptoms: tinnitus (present in most SNHL), vertigo (Meniere's disease, acoustic neuroma), ear discharge (CSOM), pain (ASOM, otitis externa), fullness (Meniere's, Eustachian tube dysfunction).
- Occupation and noise exposure: critical for NIHL — ask specifically about factory work, farming (tractor noise), military service, and recreational noise (concerts, headphones).
- Medication history: ototoxic drugs — aminoglycosides (gentamicin, amikacin), loop diuretics (furosemide), quinine, cisplatin. Even a single course of IV gentamicin can cause irreversible cochlear damage.
- Family history: genetic SNHL (important in children and young adults); otosclerosis (familial CHL).
- Ear discharge history: chronic suppurative otitis media (CSOM) is the commonest preventable cause of CHL in developing countries.
Symptom patterns that help localise the loss:
- CHL: 'I hear better in noise' (paracusis Willisii); normal-sounding own voice (bone conduction intact); better with loud speech; low-frequency rumbling tinnitus if present.
- SNHL: 'I can hear but not understand' — speech discrimination is impaired even when volume is adequate; high-frequency tinnitus; difficulty in background noise (recruitment); own voice sounds abnormally loud or distorted (diplacusis).
Degrees of hearing loss (WHO grading, better ear, pure-tone average of 0.5, 1, 2, 4 kHz):
- Mild: 26–40 dB (difficulty with faint speech)
- Moderate: 41–60 dB (difficulty with normal speech)
- Severe: 61–80 dB (difficulty even with loud speech)
- Profound: >80 dB (only amplified or tactile sound perceived)
Anatomy and Pathophysiology of Hearing Loss
Understanding the mechanism of hearing loss requires a clear mental map of the auditory pathway and knowledge of which components are vulnerable to specific insults. The sound pathway can be divided into a mechanical transmission component (outer and middle ear) and a transduction and neural component (cochlea and beyond). Damage to each division produces a different audiometric signature, and the clinician who knows this map can predict the audiogram from the history, and conversely can localise the lesion from the audiogram. This anatomical framework underpins both site-of-lesion diagnosis and rational management planning. A conductive lesion always has a normal cochlea and normal bone conduction; a sensorineural lesion always has elevated bone conduction thresholds. Knowing where the pathway is broken predicts the audiogram with precision.
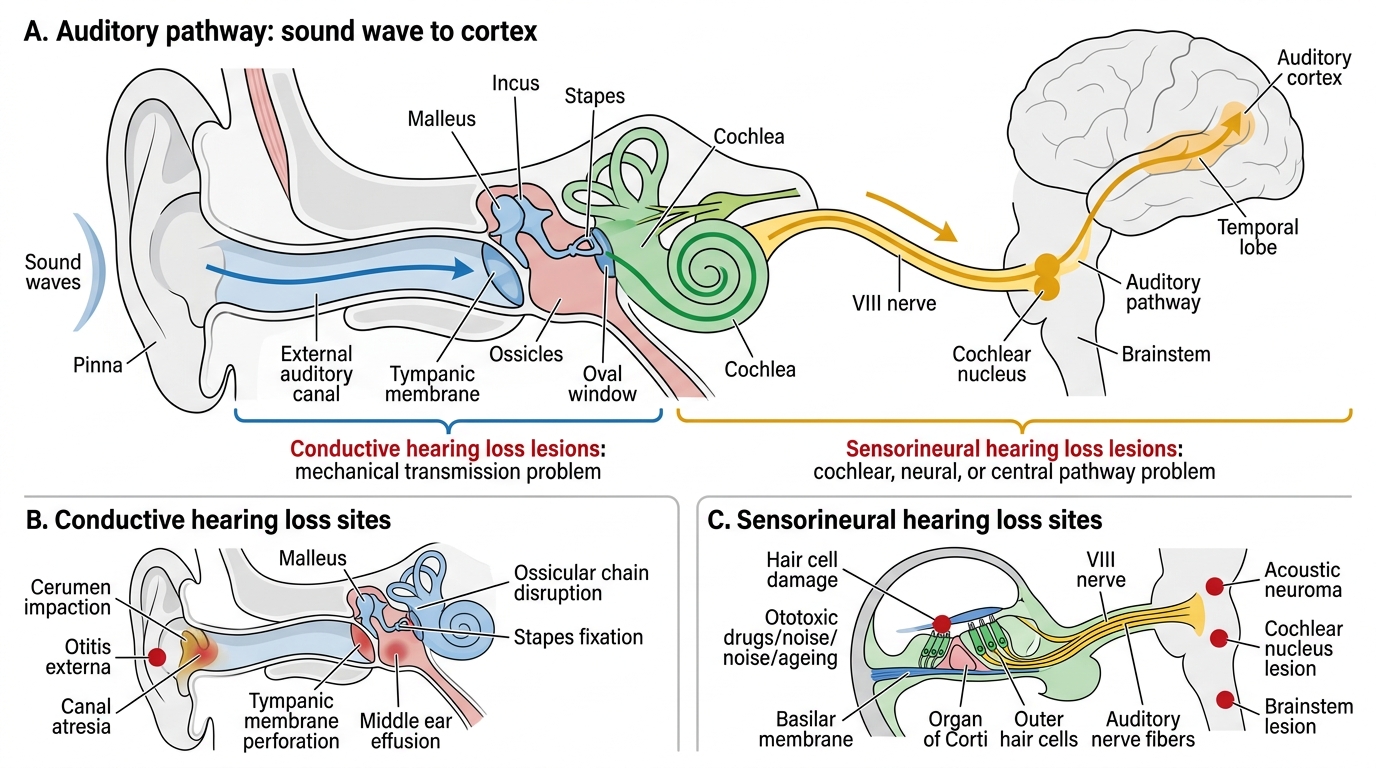
Auditory Pathway and Sites of Hearing Loss
Conductive hearing loss arises from any lesion that reduces the mechanical transmission of sound from the environment to the cochlear fluid. Common sites:
- Outer ear: wax impaction (cerumen), foreign body, otitis externa, canal atresia
- Middle ear: tympanic membrane perforation (CSOM), middle ear effusion (glue ear — commonest CHL in children), acute otitis media (ASOM), ossicular chain disruption (erosion by cholesteatoma, trauma), otosclerosis (stapes fixation)
Sensorineural hearing loss arises from dysfunction of the cochlear sensory epithelium, the eighth nerve, or central auditory pathways:
- Cochlear (sensory) SNHL: damage to the inner and outer hair cells of the organ of Corti. Hair cells are post-mitotic — they do not regenerate once destroyed. The outer hair cells are especially vulnerable (they die before inner hair cells in most pathologies). Common causes: noise, ototoxic drugs, ageing (presbyacusis), infections (viral labyrinthitis), congenital/genetic.
- Neural/retrocochlear SNHL: damage to the VIII nerve or cochlear nuclei. Causes: acoustic neuroma, brainstem strokes, MS, meningitis.
Why NIHL notches at 4 kHz: The basal cochlea (encoding 4–6 kHz) receives the most intense mechanical stimulation for sounds in the speech-frequency range because of the acoustic resonance of the ear canal (~2–4 kHz). Additionally, the blood supply to the basal turn is end-arterial with no collateral redundancy, making it the most vulnerable region to metabolic stress from noise-induced vasoconstriction and reactive oxygen species generation. This vulnerability produces the characteristic 4 kHz notch — the pathognomonic audiometric signature of noise-induced cochlear damage.
Presbyacusis is the most common form of SNHL globally. It results from gradual age-related degeneration of cochlear hair cells (most pronounced at the basal turn, hence high-frequency loss), loss of spiral ganglion neurones, and stiffening of the basilar membrane. It is bilateral, symmetric, and slowly progressive — the audiometric pattern is a gently sloping high-frequency SNHL with no air-bone gap.
Ototoxicity is cochlear or vestibular damage from drugs or chemicals. The classic ototoxic drugs in clinical practice are:
- Aminoglycoside antibiotics (gentamicin, amikacin, streptomycin): preferentially damage outer hair cells at the basal turn; cochleotoxic and vestibulotoxic; risk increases with cumulative dose and in renal impairment
- Cisplatin (and other platinum-based chemotherapy): bilateral, irreversible high-frequency SNHL; dose-dependent
- Loop diuretics (furosemide in high IV doses): usually reversible if drug stopped early; synergistic toxicity with aminoglycosides
- Quinine/antimalarials: reversible tinnitus and SNHL at high doses; usually recovers on cessation
SELF-CHECK
A 55-year-old factory worker presents with bilateral hearing difficulty. Pure-tone audiometry shows a bilateral symmetric sensorineural loss with a characteristic dip at 4000 Hz bilaterally, with recovery toward normal at 8000 Hz. The most likely cause is:
A. Presbyacusis (age-related hearing loss)
B. Noise-induced hearing loss
C. Bilateral acoustic neuroma
D. Ototoxicity from aminoglycoside antibiotics
Reveal Answer
Answer: B. Noise-induced hearing loss
The 4 kHz notch — a dip at 4000 Hz with partial recovery at 8000 Hz — is the pathognomonic audiometric signature of noise-induced hearing loss. The basal cochlea (4–6 kHz) is preferentially damaged because of its resonant properties and end-arterial blood supply. Presbyacusis causes a gradually sloping high-frequency loss without a discrete notch at 4 kHz. Bilateral acoustic neuromas (NF2) are rare and would typically show asymmetry and retrocochlear audiometric features. Aminoglycoside ototoxicity begins at the basal turn but tends to produce a broader high-frequency loss without the characteristic notch-and-recovery pattern.
ENT Examination and Investigations
The examination of a patient with hearing loss begins with otoscopy and proceeds through tuning-fork tests to formal audiological assessment. Each step adds precision to the site-of-lesion localisation. The tuning-fork tests are performed first because they are immediate, bedside, cost-free, and provide the framework for interpreting formal audiometry. The key principle is that the tuning-fork test result should be predictable from the audiogram — if they disagree, one or both was performed incorrectly. Mastering the tuning-fork tests in otoscopy in this logical sequence is the foundation of ENT examination.
Provided image
Otoscopy: Inspect the external canal (wax, discharge, foreign body) and the tympanic membrane (intact vs perforated, any retraction pockets, effusion signs). A perforated or severely retracted TM explains a CHL without further testing. An intact, normal TM with significant CHL points to the middle ear or ossicles (effusion, otosclerosis, ossicular abnormality).
Tuning-fork tests (512 Hz standard for clinical use):
The three clinical tests:
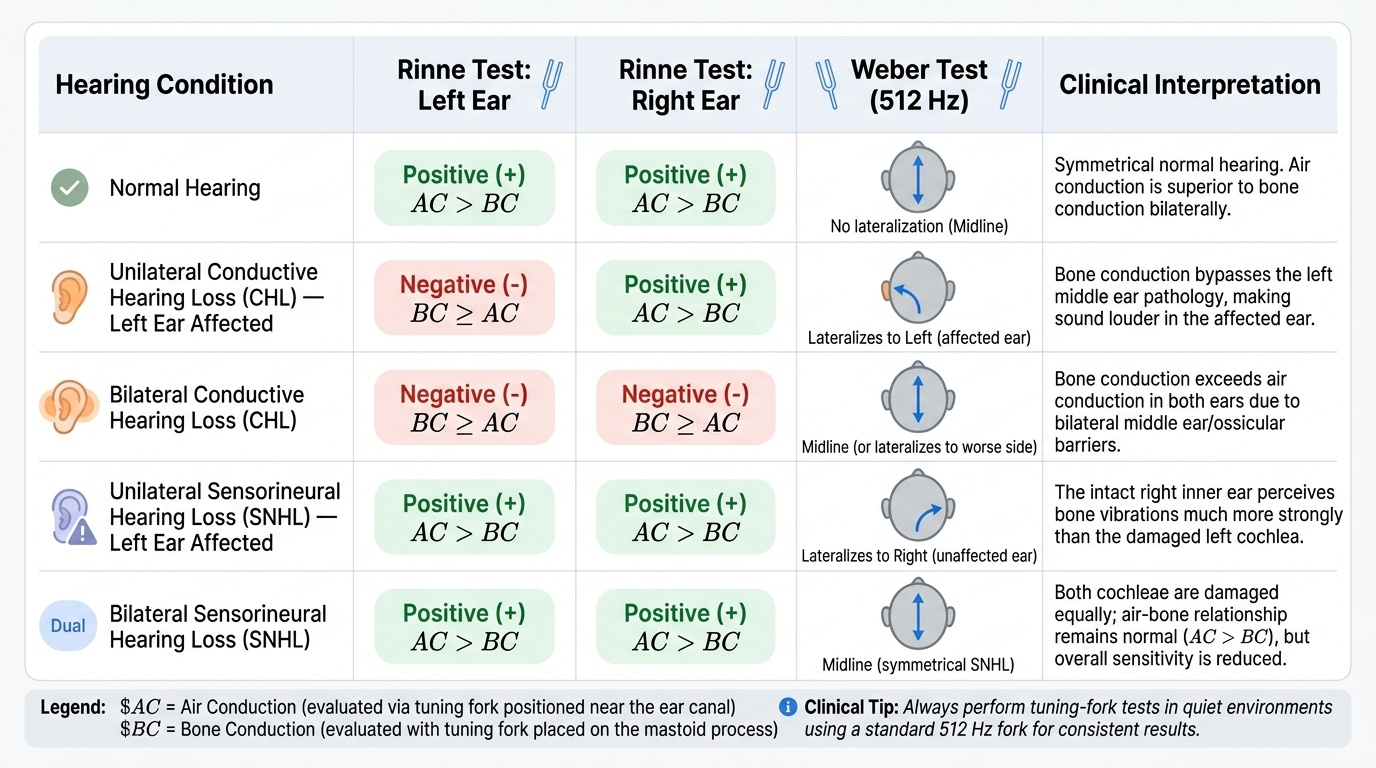
- Rinne test: Strike the tuning fork, place on mastoid (BC), then move to 1 cm from the ear canal (AC). Rinne positive = AC > BC = normal or SNHL. Rinne negative = BC > AC = CHL ≥30–35 dB. A false-negative Rinne can occur in severe unilateral SNHL (sound from BC crosses to the better cochlea via skull). Always check both ears.
- Weber test: Strike the tuning fork, place on the vertex of the skull. Normally perceived centrally. Lateralises to the affected (worse) ear in CHL. Lateralises to the better (unaffected) ear in SNHL. Do NOT invert these — this is a classic known-trap.
- Absolute Bone Conduction (ABC) test: Compare patient's BC with examiner's BC at the mastoid. BC reduced compared to examiner = SNHL (poor cochlear reserve). BC equal to examiner's BC = CHL (normal cochlea).
Pure-tone audiometry (PTA): The formal, calibrated assessment. Plots hearing threshold (dB HL) against frequency (250–8000 Hz) for both air conduction (headphones: O for right, X for left) and bone conduction (mastoid vibrator: [ for right, ] for left). Key patterns:
- CHL: air-bone gap (AC threshold elevated; BC normal)
- SNHL: no air-bone gap (both AC and BC elevated equally)
- Mixed HL: air-bone gap present AND bone conduction also elevated
Tympanometry: Measures middle ear compliance and pressure. Types: A (normal), As (stiff — otosclerosis), Ad (hypercompliant — ossicular discontinuity), B (flat — effusion/perforation), C (negative pressure — Eustachian tube dysfunction).
Otoacoustic emissions (OAEs): Generated by outer hair cells; absent when outer hair cells are damaged. Used in neonatal hearing screening (DPOAE/TEOAE) and to distinguish cochlear from retrocochlear SNHL (OAEs present = outer hair cells intact = likely retrocochlear loss).
Auditory brainstem response (ABR): Electrophysiological test of VIII nerve and brainstem auditory pathway; threshold estimation; detects retrocochlear pathology. Essential for infants and uncooperative patients.