Page 16 of 29
EN4.18 | Meniere's Disease — SDL Guide
Learning Objectives
- Describe the clinical tetrad of Meniere's disease with accurate episode duration
- Explain the pathophysiology of endolymphatic hydrops and the mechanism of acute attacks
- Interpret the investigations used in Meniere's disease, including electrocochleography
- Apply the AAO-HNS diagnostic criteria to distinguish Meniere's disease from BPPV and vestibular neuritis
- Outline the step-up management approach from dietary modification to intratympanic therapy and surgery
INSTRUCTIONS
Meniere's disease is the paradigm case for episodic audiovestibular dysfunction — a condition that simultaneously affects hearing and balance in attacks, with progressive cochlear damage over time. This SDL emphasises the clinical tetrad (which includes aural fullness, often under-tested), the precise episode duration that distinguishes Meniere's from BPPV and vestibular neuritis (an EN known-trap), the step-up management approach, and the distinction between intratympanic steroids (hearing-preserving) and intratympanic gentamicin (vestibular ablation, sacrifices hearing).
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 13 (Meniere's Disease) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 246 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old banker has been having attacks of violent spinning for the past 8 months. Each attack lasts 2–3 hours, comes on without warning, and is accompanied by a roaring noise in the left ear, muffled hearing in that ear during the attack, and a persistent feeling of pressure in the ear. Between attacks he feels mostly normal but notices his hearing in the left ear is gradually getting worse. He has seen a neurologist who says 'no stroke,' and his MRI brain was normal. What is the diagnosis, what investigation will confirm it, and what is the first-line treatment?
WHY THIS MATTERS
Meniere's disease is one of the most disabling chronic inner ear disorders, affecting an estimated 0.1–0.2% of the general population. It is important for two reasons: first, it is the paradigm case of episodic inner ear disease that damages both cochlear and vestibular function simultaneously — making it the most complex and disabling of the common vestibular disorders; and second, it is the most commonly misdiagnosed and over-diagnosed vestibular condition, with many patients labelled 'Meniere's' who actually have BPPV or vestibular migraine. The distinction between Meniere's and BPPV is one of the most commonly examined known-traps in ENT finals: Meniere's produces episodes lasting hours with hearing loss, tinnitus, and aural fullness; BPPV produces episodes lasting seconds without hearing symptoms. The condition is also important because its management is genuinely step-up — starting from inexpensive dietary modifications and escalating through medications, intratympanic injections, and finally surgery in refractory cases.
RECALL
Recall from your vestibular physiology that the inner ear is divided into two fluid compartments: the endolymph (high potassium, low sodium, filling the membranous labyrinth — scala media, utricle, saccule, semicircular canals) and the perilymph (high sodium, low potassium, filling the bony labyrinth — scala vestibuli and scala tympani). The endolymph is secreted by the stria vascularis and resorbed by the endolymphatic sac (located in a bony recess in the posterior cranial fossa). Recall also that the cochlea is tonotopically organised: the apex encodes low frequencies (250–500 Hz) and is most vulnerable to the increased pressure from endolymphatic distension, explaining why Meniere's hearing loss begins as a low-frequency SNHL — not the high-frequency loss of presbyacusis or NIHL. Finally, recall the Meniere's vs BPPV vs vestibular neuritis distinction from the vertigo SDL: episode duration is the key differentiator.
Clinical Presentation of Meniere's Disease
Meniere's disease presents with a characteristic clinical tetrad that should be stated in full — omitting the fourth feature (aural fullness) is the most common examination error. The tetrad comprises four features that occur together during an attack, and their combination is what establishes the diagnosis. Each feature has specific characteristics that distinguish Meniere's disease from other vestibular and cochlear disorders.
Each of the four tetrad features has a characteristic quality that distinguishes Meniere's disease from its common mimics, and the examiner who asks about the episode duration, the frequency characteristics of the hearing loss, and the quality of the tinnitus will correctly identify Meniere's disease in the majority of cases before any investigation is performed. The four features of the tetrad, each with their distinguishing clinical characteristics, are as follows:
- Episodic vertigo lasting 20 minutes to several hours (typically 20 minutes to 4–8 hours; most attacks last 2–4 hours). This specific duration range is the most important differentiating feature: BPPV episodes last seconds, vestibular neuritis is a single sustained attack lasting days, and migraine-associated vertigo may overlap but lacks the full audiovestibular syndrome. Attacks come on without warning, are severe and disabling, and are typically accompanied by nausea and vomiting. They resolve completely, leaving the patient exhausted but neurologically intact.
- Fluctuating sensorineural hearing loss — characteristically low-frequency in early disease, affecting 250–1000 Hz preferentially. The loss worsens during attacks and partially or fully recovers between attacks in early stages. This fluctuation is pathognomonic — it distinguishes Meniere's from other causes of SNHL. Over time (years), the loss becomes permanent and all-frequency, with no inter-attack recovery.
- Tinnitus — typically low-pitched, often described as a 'roar,' 'rush,' or 'hum' in the affected ear, worsening before and during attacks.
- Aural fullness (pressure or 'blocked' sensation in the ear) — typically worsens before the vertigo attack begins and may serve as a prodrome. This is the fourth feature that students most often omit.
Disease stages (Shambough staging):
Early stage: reversible low-frequency SNHL, acute attacks; Middle stage: established permanent loss, reduced attack frequency; Late ('burnt-out') stage: attacks cease (vestibular damage complete), but permanent SNHL and disequilibrium persist.
Bilateral disease: occurs in 15–40% of patients over 10 years of disease, making Meniere's disease a potential cause of bilateral progressive SNHL.
Meniere's disease vs Meniere's syndrome: Meniere's disease is idiopathic endolymphatic hydrops; Meniere's syndrome refers to the same clinical picture when caused by a known aetiology (syphilis, hypothyroidism, autoimmune inner ear disease, viral labyrinthitis).
Anatomy and Pathophysiology
The pathological basis of Meniere's disease is endolymphatic hydrops — abnormal distension of the endolymph-filled membranous labyrinth. The mechanism that produces this distension is believed to be failure of endolymphatic sac function: the endolymphatic sac, which normally resorbs excess endolymph, is dysfunctional in Meniere's disease, leading to progressive accumulation of endolymph and rising pressure throughout the membranous labyrinthine system. The cause of endolymphatic sac dysfunction is not fully understood — it is idiopathic in Meniere's disease, though genetic factors, immunological mechanisms, and viral injury to the endolymphatic sac have all been proposed. Understanding the anatomy of the membranous labyrinth as a closed, pressure-sensitive system is the key to understanding why hydrops produces the specific combination of cochlear and vestibular symptoms that constitute the Meniere's tetrad, and why treatment strategies aimed at reducing endolymphatic pressure can reduce attack frequency.
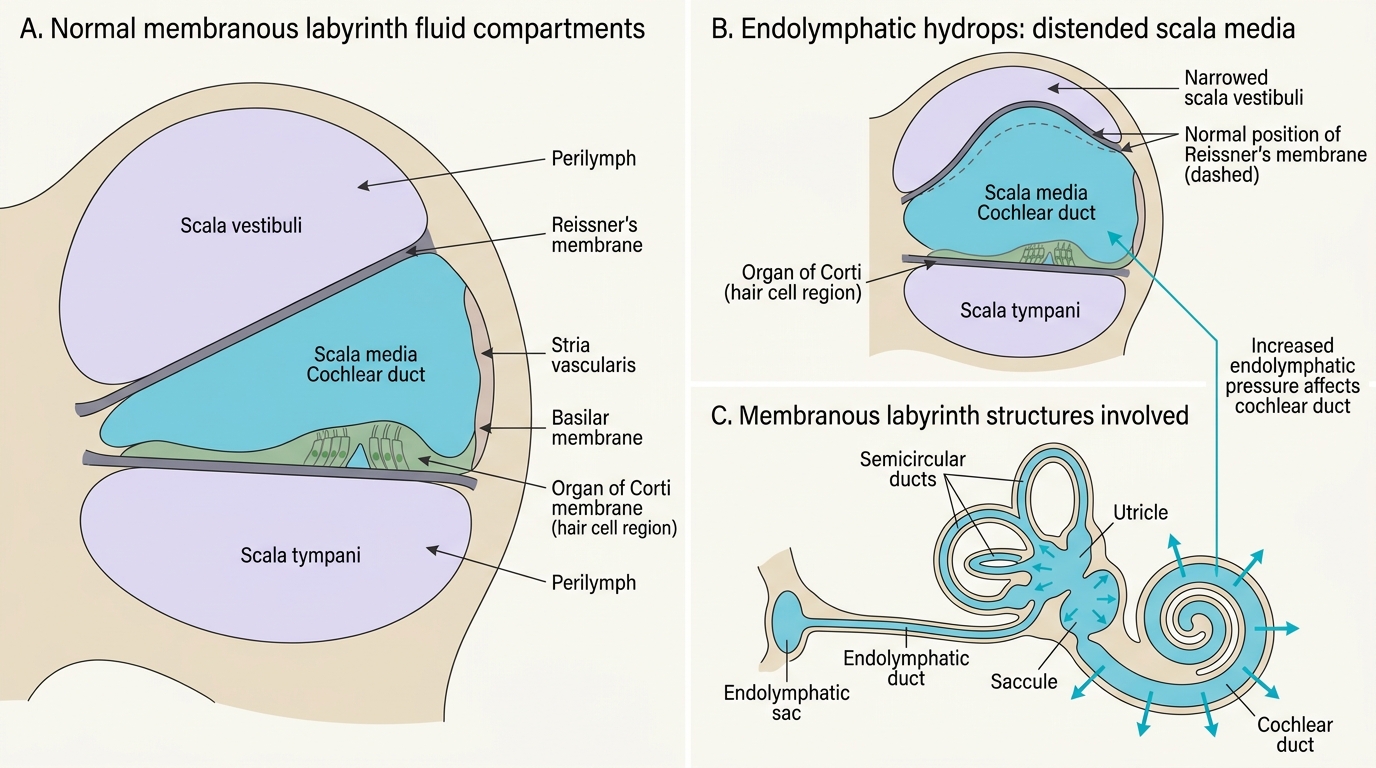
Normal Labyrinth Fluid Compartments and Endolymphatic Hydrops
The mechanism of an acute Meniere's attack is understood as follows: progressive build-up of endolymphatic pressure stretches the thin Reissner's membrane (separating the scala media from the scala vestibuli) and the membranous walls of the utricle and saccule. When pressure exceeds the mechanical tolerance of these membranes, they rupture. The rupture allows potassium-rich endolymph to flood into the perilymph compartment, creating a sudden surge in potassium concentration around the hair cells and vestibular nerve endings. Potassium (normally the stimulus for receptor depolarisation when released from the stereocilia tips into endolymph) now floods the perilymph in large amounts, causing uncontrolled depolarisation and then paralysis of the hair cells and vestibular nerve endings — producing the acute attack of vertigo and temporary cochlear dysfunction (hearing loss + tinnitus + fullness). After the rupture seals (spontaneously, within hours), the ionic imbalance resolves, the vestibular nerve recovers, and the attack ends.
Why low-frequency hearing loss? The apex of the cochlea (encoding low frequencies 250–500 Hz) is most vulnerable to the elevated endolymphatic pressure because the cochlear duct is widest and least rigid at the apex. The apical hair cells are thus the first to be damaged when hydrops distends the cochlear duct, explaining the characteristic low-frequency audiometric pattern in early Meniere's disease.
SELF-CHECK
A 48-year-old woman has recurring attacks of vertigo lasting 1–2 hours, accompanied by a low-pitched roaring sensation in the left ear and a feeling of pressure in that ear. Audiometry shows a low-frequency sensorineural hearing loss on the left that is worse immediately after an attack and partially recovers in between attacks. The most likely diagnosis is:
A. Benign paroxysmal positional vertigo (BPPV)
B. Meniere's disease
C. Vestibular neuritis
D. Acoustic neuroma
Reveal Answer
Answer: B. Meniere's disease
This is Meniere's disease: episodic vertigo lasting 1–2 hours (within the 20-minute to hours range), low-pitched tinnitus, aural fullness, and fluctuating low-frequency SNHL that worsens during attacks and partially recovers between attacks. The fluctuating audiometric pattern is pathognomonic. BPPV produces seconds-duration positional vertigo without hearing symptoms. Vestibular neuritis produces a single sustained episode (days) without hearing loss. Acoustic neuroma produces slowly progressive SNHL (not fluctuating) with minimal vertigo.
Investigations
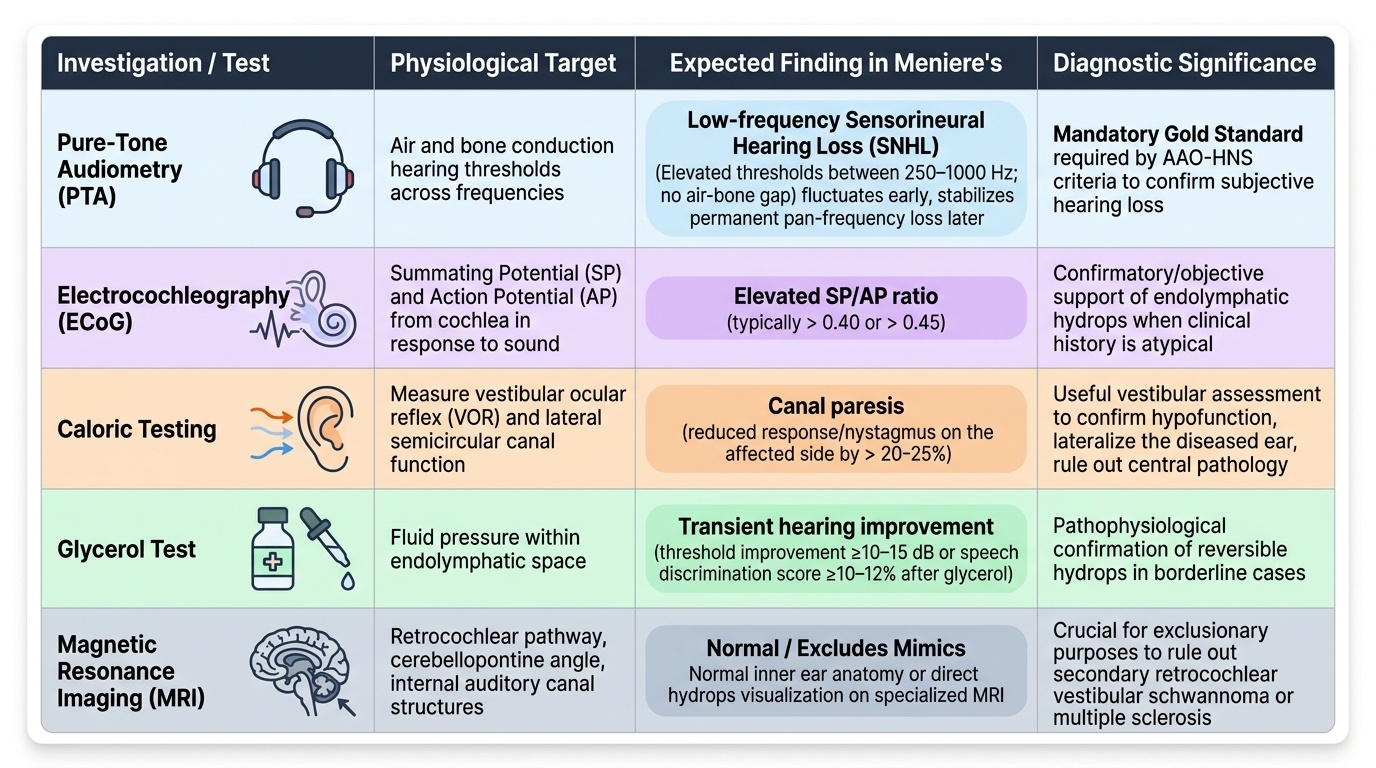
Investigations in Meniere's disease aim to confirm the diagnosis by documenting the characteristic audiometric profile, to assess vestibular function, and to exclude secondary causes. The investigations should be interpreted in the context of the clinical history — no single test has sufficient sensitivity and specificity to make the diagnosis alone, and the AAO-HNS diagnostic criteria require clinical features plus audiometric confirmation. The key audiological finding — low-frequency SNHL with fluctuation — and the electrocochleographic evidence of endolymphatic hydrops together provide the strongest objective support for the clinical diagnosis. In routine clinical practice in India, PTA and a clinical history consistent with the tetrad are sufficient to make the diagnosis and initiate treatment; ECoG and glycerol testing are used when the diagnosis is uncertain. The table below summarises each investigation in terms of what it measures, the expected finding in Meniere's disease, and its practical role in the diagnostic workup.
Provided image
1. Pure-tone audiometry (PTA):
Characteristic finding: low-frequency SNHL (250–1000 Hz preferentially elevated; AC = BC; no air-bone gap). In early stages, the audiogram may normalise between attacks. In established disease: permanent pan-frequency SNHL developing over years. Serial audiograms showing fluctuating thresholds at low frequencies are highly suggestive.
2. Electrocochleography (ECoG):
Records electrical activity of the cochlea in response to click or tone stimuli. The summating potential (SP) reflects the receptor potential of hair cells; the action potential (AP) reflects the VIII nerve compound action potential. In endolymphatic hydrops, the SP is disproportionately elevated, producing an elevated SP/AP ratio (>0.37–0.50 depending on the laboratory). An elevated SP/AP ratio is considered the most specific objective evidence of endolymphatic hydrops.
3. Glycerol dehydration test:
A dose of oral glycerol (1.5 g/kg in orange juice) is given as an osmotic agent to temporarily reduce endolymphatic volume. Improvement of ≥15 dB at ≥2 audiometric frequencies within 2 hours = positive test, supporting Meniere's disease. Useful when the diagnosis is uncertain.
4. Caloric testing (ENG/VNG):
Demonstrates canal paresis (reduced response) on the affected side in established disease, reflecting cumulative vestibular hair cell damage. In early disease, caloric response may be normal.
5. MRI with gadolinium:
Performed to exclude acoustic neuroma (which can present with SNHL and tinnitus). Endolymph MRI (3T with intratympanic gadolinium) can now visualise endolymphatic hydrops directly, but this is primarily a research tool. Standard MRI shows no abnormality in idiopathic Meniere's disease.