Page 13 of 29
EN4.17 | Vertigo with Vestibular Function Assessment — SDL Guide
Learning Objectives
- Define vertigo and distinguish it from dizziness, presyncope, and disequilibrium
- Describe the clinical features of the three commonest peripheral vestibular disorders: BPPV, Meniere's disease, and vestibular neuritis
- Explain the anatomy of the vestibular labyrinth and the pathophysiology of BPPV and endolymphatic hydrops
- Perform and interpret the Dix-Hallpike test for BPPV
- Interpret caloric test results and identify the pattern of canal paresis
- Distinguish peripheral from central vertigo and identify when imaging is mandatory
- Outline the management of BPPV (Epley manoeuvre) and vestibular neuritis
INSTRUCTIONS
Vertigo is one of the most common ENT presentations in any outpatient setting and carries significant morbidity — patients often cannot stand or walk during acute episodes. The ability to rapidly distinguish the three common peripheral causes (BPPV, Meniere's disease, vestibular neuritis) from each other and from dangerous central causes (brainstem/cerebellar stroke) is a core clinical competency. EN4.17 requires you to know the clinical features, vestibular function investigations, and management of vertigo.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 14 (Vertigo and Vestibular Disorders) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 245 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old woman is brought to your clinic by her husband. She says that for the past 2 days, every time she turns over in bed or looks up, the room spins violently for about 30 seconds, then stops. She has no hearing loss, no tinnitus, and no ear symptoms. She had a similar episode 18 months ago that resolved on its own. She is terrified she is having a stroke. Is this an emergency requiring CT brain, or is it a common benign condition you can treat in the clinic in 5 minutes?
WHY THIS MATTERS
Vertigo — the illusion of movement, typically spinning, when no movement is occurring — is one of the five most common reasons for adult ENT referral worldwide and accounts for 5–10% of all primary care consultations in India. It causes significant functional disability: patients may be unable to drive, work, or perform daily activities during acute episodes. The three conditions responsible for the vast majority of cases are benign paroxysmal positional vertigo (BPPV) (the commonest cause of episodic positional vertigo, entirely treatable in one clinic visit), Meniere's disease (episodic vertigo with audiovestibular triad), and vestibular neuritis (acute continuous vertigo, usually self-limiting). The critical clinical skill — and the focus of this SDL — is to distinguish these three from each other and from central vertigo (caused by posterior fossa stroke, tumour, or demyelination), which requires emergency imaging and is potentially life-threatening. The Meniere's triad versus BPPV distinction is one of the most commonly examined EN known-traps.
RECALL
Recall from your physiology studies that the vestibular labyrinth contains two functional components: the semicircular canals (three on each side: anterior/superior, posterior, lateral/horizontal) — which detect angular acceleration — and the otolithic organs (utricle and saccule) — which detect linear acceleration and gravity. The sensory apparatus in each canal is the cupula in the ampulla; in the otolithic organs it is the macula, embedded with otoconia (calcium carbonate crystals). Neural signals from the vestibular end organs travel via the vestibular division of the VIII nerve to the vestibular nuclei in the brainstem, which coordinate eye movements (vestibulo-ocular reflex), postural tone, and conscious perception of movement. Nystagmus — rhythmic involuntary eye movement — is the cardinal sign of vestibular dysfunction and can help localise a lesion to the peripheral (labyrinth/VIII nerve) or central (brainstem/cerebellum) system.
Clinical Presentation of Vertigo
The clinical history is the most powerful diagnostic tool in vertigo. Three questions — duration of each episode, relationship to position, and presence of hearing loss or tinnitus — will correctly identify the most likely diagnosis in over 80% of cases before any test is performed.
The duration of each episode is the single most discriminating feature. Brief episodes lasting only seconds to under a minute, triggered by specific head movements, point strongly to BPPV — no other common vestibular condition produces seconds-duration positional vertigo. Episodes lasting 20 minutes to several hours (typically 20 minutes to 4 hours), recurring multiple times over months to years, accompanied by fluctuating low-frequency sensorineural hearing loss, tinnitus, and a feeling of ear fullness, are the hallmark of Meniere's disease — the endolymphatic hydrops triad. A single episode of severe, incapacitating vertigo lasting days to weeks, with nausea and vomiting, that gradually improves with time, without any hearing loss, is the presentation of vestibular neuritis. Understanding these three patterns is the clinical foundation of vertigo diagnosis.
Key diagnostic pattern summary:
| Condition | Episode duration | Hearing loss | Tinnitus | Triggering position |
|---|---|---|---|---|
| BPPV | Seconds (<1 min) | No | No | Yes (Dix-Hallpike +) |
| Meniere's disease | 20 min – several hours | Yes (low-freq, fluctuating) | Yes | No |
| Vestibular neuritis | Days to weeks (continuous) | No | No | No |
| Labyrinthitis | Days to weeks | Yes | Possible | No |
| Central (cerebellar stroke) | Variable | Variable | Variable | No |
Red flags suggesting central (dangerous) vertigo:
Central vertigo must be excluded urgently when the following features are present: headache of sudden onset ('thunderclap') accompanying vertigo; inability to walk despite vertigo improving (cerebellar ataxia out of proportion to the dizziness); vertical or direction-changing nystagmus; diplopia or dysphagia; limb incoordination; crossed sensory/motor signs. Any of these mandates CT/MRI brain as an emergency.
The distinction between peripheral and central nystagmus at the bedside is clinically critical:
- Peripheral nystagmus: unidirectional (fast phase always the same direction), horizontal or torsional, enhanced by removing fixation, suppressed by visual fixation; associated with severe vertigo.
- Central nystagmus: direction-changing, vertical (pure vertical nystagmus is always central), not suppressed by fixation; may occur without severe vertigo.
Anatomy and Pathophysiology of Vestibular Disorders
A clear understanding of vestibular anatomy allows the pathophysiology of the three common disorders to be derived rather than memorised. The key insight is that different conditions disrupt vestibular function at different anatomical levels — BPPV at the level of the semicircular canal mechanics, Meniere's disease at the level of inner ear fluid homeostasis, and vestibular neuritis at the level of the nerve itself. The three paired semicircular canals are oriented at right angles to each other, so each canal detects rotation in a specific plane. The posterior canal is most commonly affected in BPPV because, in the normal upright position, it is oriented vertically and any dislodged otoconia from the nearby utricle will tend to settle there under gravity. The anterior and horizontal canals are less commonly affected. The membranous labyrinth, which floats within the bony labyrinth and contains endolymph, is the site of Meniere's disease pathology.
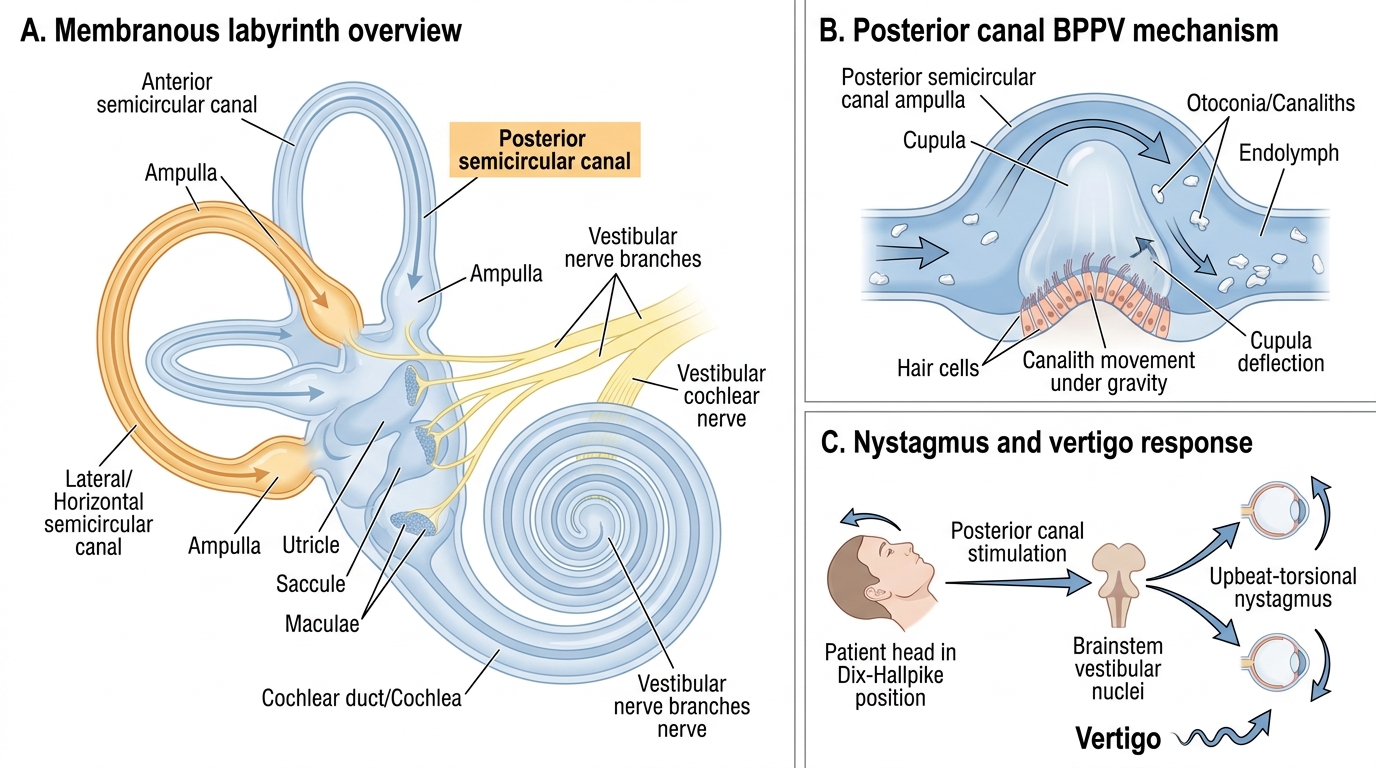
Membranous Labyrinth and Posterior Canal BPPV Mechanism
BPPV — Canalith repositioning mechanism:
The otoconia (calcium carbonate crystals) normally sit on the maculae of the utricle and saccule. In BPPV, these crystals become dislodged — often after head trauma, viral illness, or prolonged bed rest, or spontaneously — and migrate into a semicircular canal, most commonly the posterior canal (accounting for ~80% of BPPV cases). When the head moves into the provoking position, the free-floating otoconia (canalith) move within the canal under gravity, creating abnormal endolymph flow that deflects the cupula. The cupula deflection mimics a rotational stimulus to the brain, producing vertigo and nystagmus. The Dix-Hallpike manoeuvre reproduces this by rapidly moving the head into the provoking position (head turned 45 degrees toward the affected ear, rapid movement to supine with head over the edge of the table). The characteristic response — upbeat-torsional nystagmus with a 2–5 second latency and <1 minute duration that fatigues on repetition — is pathognomonic of posterior canal BPPV.
Meniere's disease — Endolymphatic hydrops:
The inner ear fluid balance is maintained by active secretion and resorption of endolymph in the membranous labyrinth, regulated by the endolymphatic sac (an absorption organ in the posterior cranial fossa). In Meniere's disease, this regulation fails — the endolymphatic sac absorbs inadequately, causing endolymphatic hydrops: distension of the endolymph-filled membranous labyrinth. The distended scala media ruptures periodically, mixing endolymph (high K⁺) with perilymph (high Na⁺), depolarising the hair cells and nerve endings in an uncontrolled manner and producing the acute attack of vertigo. The hearing loss is initially low-frequency and fluctuating (the apex of the cochlea, encoding low frequencies, is most vulnerable to the increased pressure); over years, it becomes permanent and all-frequency.
Vestibular neuritis — Unilateral peripheral deafferentation:
Vestibular neuritis is believed to result from reactivation of HSV-1 in the Scarpa's ganglion or acute viral inflammation of the superior vestibular nerve, leading to sudden unilateral loss of vestibular input. The result is an acute asymmetry of vestibular tone — the intact contralateral vestibular system generates tonic discharge unopposed, driving the eyes toward the affected (silent) side. The nystagmus is toward the intact side (fast phase away from the lesion). Over days to weeks, central compensation restores balance by downregulating the intact side's gain to match the deafferented side — this is the mechanism of spontaneous recovery.
SELF-CHECK
A 65-year-old man presents with brief episodes of violent spinning lasting 20–30 seconds, triggered by turning over in bed. He has no hearing loss and no tinnitus. The Dix-Hallpike test on the right produces upbeat-torsional nystagmus after a 3-second latency; it fatigues on repeat. The most likely diagnosis is:
A. Meniere's disease — the episodic nature is typical
B. Benign paroxysmal positional vertigo (BPPV) of the right posterior canal
C. Vestibular neuritis — the sudden onset is characteristic
D. Central cerebellar pathology requiring MRI
Reveal Answer
Answer: B. Benign paroxysmal positional vertigo (BPPV) of the right posterior canal
The diagnostic combination is classic BPPV: brief positional vertigo (<1 minute), no hearing loss, no tinnitus, positive Dix-Hallpike with upbeat-torsional nystagmus, latency of a few seconds, and fatigability on repeat. Meniere's disease produces episodes lasting 20 minutes to hours with hearing loss and tinnitus. Vestibular neuritis produces days of continuous (not episodic, not positional) vertigo. Central vertigo would produce non-fatigable, direction-changing, or vertical nystagmus — not the fatigable upbeat-torsional pattern of BPPV.
Vestibular Function Assessment and Investigations
Vestibular function assessment uses a combination of bedside clinical tests, formal vestibulometric tests, audiometry, and imaging. The bedside tests (Dix-Hallpike, Romberg, head-impulse test) provide immediate diagnostic information with no equipment cost. Formal tests (caloric testing, VNG, VEMP) quantify vestibular asymmetry and are used to confirm and localise unilateral vestibular hypofunction. Understanding what each test measures and what an abnormal result means is essential for both diagnosis and examination.
1. Dix-Hallpike test:
The gold standard test for posterior canal BPPV. Technique: patient seated, head turned 45 degrees toward the test ear, rapidly moved to supine with head hanging 20–30 degrees below the table edge. A positive test: upbeat-torsional nystagmus appearing after a latency of 2–5 seconds, lasting <1 minute, and fatiguing on repeat. The nystagmus reverses direction when the patient is returned to sitting. The affected ear is the one toward which the head is rotated (the ear on the lowermost side in the supine position). A negative Dix-Hallpike in a patient with positional vertigo prompts horizontal canal BPPV testing (supine roll test).
2. Romberg test and gait testing:
Romberg test: patient stands with feet together, eyes open (stable) then eyes closed. Falls or significant sway with eyes closed = positive Romberg. In vestibular disease, the patient falls/sways toward the side of the lesion. Gait: patients with peripheral vestibular loss drift toward the affected side; in cerebellar disease, gait is wide-based and severely ataxic (cannot tandem walk).
3. Head impulse test (HIT):
Rapid, small-amplitude head rotation to one side while the patient fixates on the examiner's nose. In normal peripheral vestibular function, eyes stay fixed (vestibulo-ocular reflex intact). In unilateral vestibular hypofunction, a corrective saccade (catch-up eye movement back to fixation) is seen when the head is turned toward the affected side — this is a positive HIT, indicating peripheral vestibular loss.
4. Caloric testing:
The bedside 'gold standard' for quantifying unilateral peripheral vestibular hypofunction. Principle: irrigation of the external ear canal with warm (44°C) or cold (30°C) water creates a temperature gradient in the horizontal semicircular canal, inducing endolymph convection and nystagmus. Warm water = nystagmus toward the irrigated ear (fast phase); cold water = nystagmus away. Mnemonic: COWS (Cold Opposite, Warm Same). Canal paresis formula: asymmetry of responses between the two ears; >25% difference = significant unilateral canal paresis (reduced function on that side).
5. Vestibular evoked myogenic potentials (VEMP):
CVEMP (cervical) assesses saccular function (inferior vestibular nerve); oVEMP (ocular) assesses utricular function. Used in Meniere's disease monitoring and superior canal dehiscence assessment.
6. Audiometry:
Essential in all vertigo patients. Low-frequency SNHL in a patient with episodic vertigo = Meniere's. Normal audiogram in BPPV and vestibular neuritis. SNHL + vestibular hypofunction = labyrinthitis.
7. MRI with gadolinium:
Indicated when central vertigo is suspected (red flags), when there is unilateral SNHL with vertigo (exclude acoustic neuroma), or when BPPV treatment fails.