Page 4 of 23
EN4.4 | Otitis Media with Effusion — SDL Guide
Learning Objectives
- Elicit a structured history in a child or adult presenting with hearing loss and identify features that distinguish OME from ASOM
- Describe the otoscopic and tympanometric findings characteristic of OME
- Explain the pathophysiological mechanism linking Eustachian tube dysfunction, adenoid hypertrophy, and middle ear effusion
- Describe the principles of management of OME including watchful waiting, hearing aids, and surgical intervention with grommets
INSTRUCTIONS
Otitis media with effusion (OME) is the most common cause of acquired hearing loss in children and a frequent reason for educational underachievement when undetected. Unlike ASOM, it is a silent disease — no fever, no pain — and is discovered only when hearing loss is noticed by a parent, teacher, or on school audiometry screening. Understanding when to act (and when to wait) is the key clinical challenge: most cases resolve spontaneously within 3 months, but persistent bilateral OME with significant hearing loss during critical periods of speech and language development requires surgical intervention.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 5 (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 8 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 5-year-old boy is brought by his mother with a 3-month history of 'not listening' and speaking loudly. His teacher has sent a note home saying he seems inattentive and mishears instructions. He watches television with the volume very high. He has never had ear pain or fever. His immunisations are up to date. On examination he is afebrile and appears well. Both tympanic membranes are dull, amber-coloured, slightly retracted, with no cone of light. There is no erythema and no perforation. Tympanometry shows bilateral Type B curves. What is the diagnosis, what is the mechanism, and what will you do — and NOT do — at this visit?
WHY THIS MATTERS
Otitis media with effusion (OME) is the most common cause of acquired hearing loss in children between 2 and 10 years of age. It affects approximately 80% of children at some point before their 10th birthday, though most episodes are brief and self-limiting. The clinical importance of OME comes from its ability to cause persistent mild to moderate conductive hearing loss during the critical years of speech, language, and reading acquisition. A child who mishears consistently is at risk of delayed language milestones, educational underachievement, and social withdrawal — none of which are immediately obvious as ear-related problems. Unlike ASOM, which is symptomatic and self-presenting, OME is frequently discovered only by a concerned parent or teacher, by school audiometry screening, or during a routine ENT review after a previous ASOM episode. For you as a clinician, OME matters because it is common, because the consequences of chronic untreated hearing loss during early childhood are significant, and because the management decision — watchful waiting versus surgery — requires weighing the natural history of resolution against the developmental risk of delay. Competency EN4.4 requires you to take a history, describe clinical features, choose investigations, and describe management principles.
RECALL
Recall the anatomy and physiology of the Eustachian tube (ET) from your earlier study. The ET connects the nasopharynx to the middle ear cleft and serves three functions: ventilation (equalising air pressure across the TM), mucociliary drainage of middle ear secretions into the nasopharynx, and protection from nasopharyngeal contamination. The ET is normally closed at rest and opens briefly during swallowing, yawning, and sneezing — this opening is driven by contraction of the tensor veli palatini muscle. In the nasopharynx, the ET orifice (Eustachian cushion) lies at the level of the inferior turbinate's posterior end, immediately behind and above the posterior choana. The adenoid (pharyngeal tonsil) is the lymphoid mass sitting in the roof and posterior wall of the nasopharynx — it lies in close proximity to the ET orifice, which is why adenoid hypertrophy is a major contributor to ET obstruction and OME. Recall also from your ASOM module that Stage 4 ASOM can leave a persistent residual effusion in the middle ear — this post-ASOM effusion is one of the most common routes into OME.
Clinical Presentation of Otitis Media with Effusion
The defining characteristic of OME's clinical presentation is its silence: unlike ASOM, there is no fever, no severe otalgia, and no dramatic acute illness. The child (or adult) appears well, and the hearing loss — usually mild to moderate — is so gradual in onset that it is often attributed to inattention, developmental delay, or behavioural problems before the ear is examined. The most typical presentation is a child aged 2–7 years who is referred by a schoolteacher or brought by a parent who noticed that the child does not respond when called, watches television with a very high volume, speaks loudly, and appears to mishear in noisy environments. The child may report a sensation of ear blockage or muffled hearing, but many children — particularly those under 4 years — cannot articulate this and simply adapt behaviourally. Adults with OME typically present with a sense of ear fullness, mild hearing loss, and autophony (hearing their own voice loudly) — often following a recent URTI or air travel that triggered Eustachian dysfunction.
The temporal pattern is diagnostically informative: OME that waxes and wanes with URTI episodes (better in summer, worse in winter) is consistent with recurring ET dysfunction, while persistent unilateral OME in an adult — particularly with associated nasal obstruction or a neck mass — raises the critical differential of a nasopharyngeal mass obstructing the ET orifice.
Key history points for OME:
- Onset and duration of hearing difficulty (weeks to months — not acute)
- School performance and speech development (key indicators of functional impact)
- Previous ASOM episodes (post-ASOM residual effusion is common)
- Nasal symptoms: persistent nasal obstruction, mouth breathing, snoring (adenoid hypertrophy signs)
- Family history of ear disease or hearing loss
- Presence of cleft palate, Down syndrome, or other craniofacial anomalies (increases OME risk)
- In adults: unilateral persistent OME, especially in an adult → ALWAYS exclude nasopharyngeal carcinoma (NPC)
Functional impact to document:
- Speech and language milestones (in children <5 years)
- School performance and classroom hearing ability
- Behavioural changes: social withdrawal, frustration, apparent inattention
Anatomy and Pathophysiology of OME
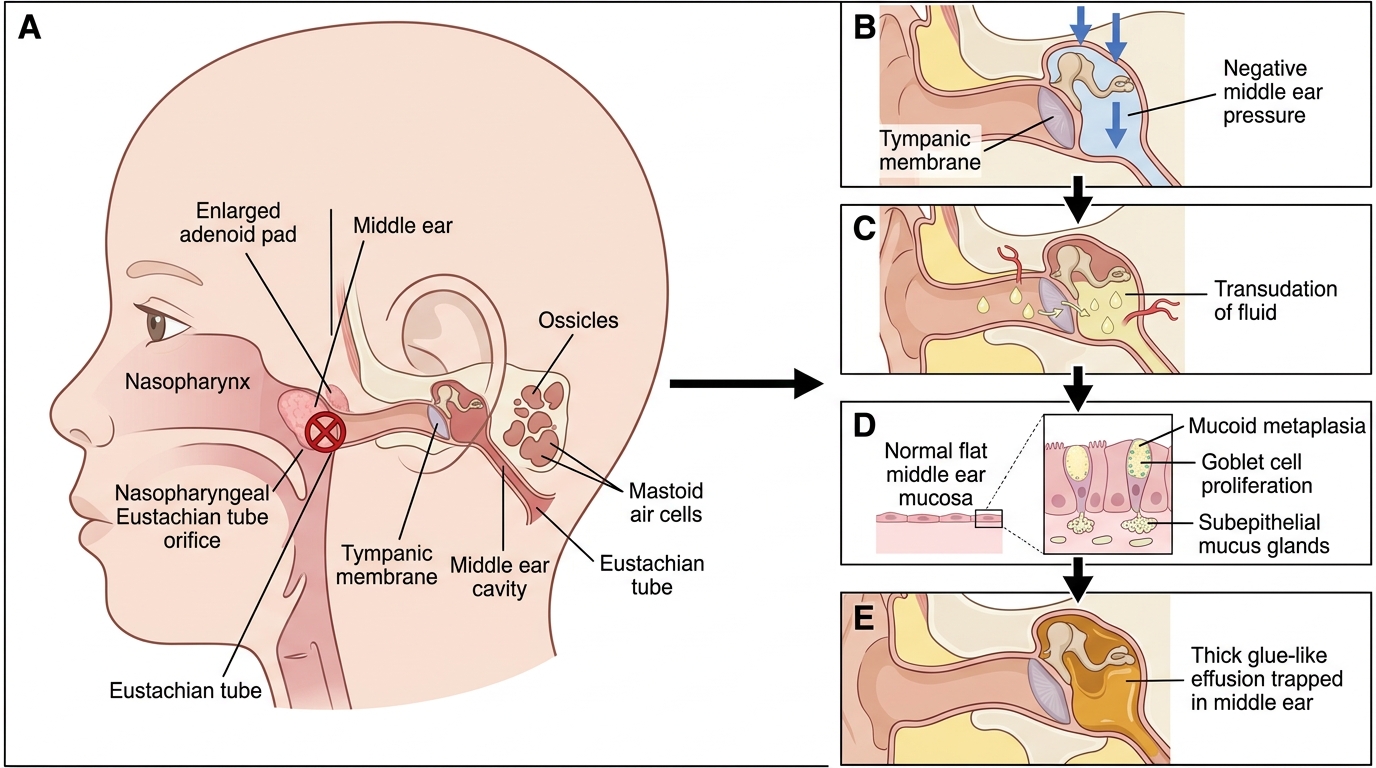
The fundamental pathophysiological event in OME is sustained negative pressure in the middle ear cleft resulting from partial or complete Eustachian tube dysfunction, which leads to transudate accumulation followed by mucoid metaplasia of the middle ear mucosa. The process begins with impaired ET ventilation: when the ET fails to open regularly during swallowing and yawning, the middle ear mucosa absorbs the existing gas, creating a negative pressure environment. Initially, this draws a watery serous transudate from the mucosal capillaries into the middle ear space — this is the serous phase of OME, characterised by a thin, straw-coloured, watery fluid. If the negative pressure and mucous membrane irritation persist, the normally flat cuboidal/columnar middle ear mucosa undergoes mucoid metaplasia — it develops goblet cells (mucus-secreting cells) and subepithelial glands not normally present in the middle ear. These cells produce a thick, viscous, mucinous secretion that accumulates in the middle ear and is unable to drain because of the same ET dysfunction that caused the initial problem. This viscous, glue-like fluid is the hallmark of chronic OME and is responsible for the colloquial name glue ear.
Aetiological contributors to ET dysfunction in OME:
- Adenoid hypertrophy: The adenoid mass mechanically obstructs the ET orifice in the nasopharynx, prevents ET opening during swallowing, and acts as a reservoir of bacteria and biofilm that produce enzymes destroying the ET mucosal cilia
- Recurrent URTI / allergy: Repeated episodes of mucosal oedema block the ET temporarily; each episode may leave a residual effusion
- Post-ASOM residual: After ASOM resolves, the middle ear mucosa may take weeks to return to normal; residual effusion persists in a significant proportion of children
- Cleft palate: The tensor veli palatini muscle (which opens the ET) attaches abnormally in cleft palate patients — ET opening is impaired throughout life; virtually all unrepaired cleft palate patients develop OME
- Down syndrome: Hypotonia of the tensor veli palatini and abnormal ET cartilage geometry cause chronic ET dysfunction
Eustachian Tube Dysfunction Pathway in Glue Ear
SELF-CHECK
A 6-year-old with persistent bilateral OME has viscous glue-like fluid in the middle ear. Which pathological change in the middle ear mucosa is responsible for the thick consistency of this fluid?
A. Squamous metaplasia producing keratin-filled debris
B. Mucoid metaplasia with goblet cell proliferation and subepithelial gland formation
C. Fibrous replacement of the mucosal stroma by scar tissue
D. Neutrophil infiltration producing purulent exudate
Reveal Answer
Answer: B. Mucoid metaplasia with goblet cell proliferation and subepithelial gland formation
Chronic ET dysfunction leads to mucoid metaplasia of the normally flat middle ear mucosa — goblet cells and subepithelial mucus glands develop that are not normally present in the middle ear. These cells produce thick viscous mucinous secretion that creates the characteristic 'glue' of glue ear. Squamous metaplasia with keratin production is associated with cholesteatoma, not OME. Purulent exudate would indicate suppurative otitis media, not the non-inflammatory effusion of OME.
Examination and Investigations
The examination of a child with suspected OME has three components: otoscopy (the most important), tympanometry, and hearing assessment. Together, these investigations confirm the presence and type of middle ear effusion, quantify any hearing loss, and determine the functional impact. The examiner who uses only otoscopy and misses tympanometry will frequently underdiagnose OME — because the otoscopic changes in OME are subtle compared to ASOM, and a TM that does not appear overtly abnormal may still have significantly reduced compliance on tympanometry. Conversely, a single abnormal tympanogram without clinical correlation can be a false positive (transient in the day of the reading). The combination of otoscopy + tympanometry + PTA provides a robust, low-cost, non-invasive investigation platform that is sufficient for most OME diagnostic decisions in primary and secondary care.
Otoscopic findings in OME:
- TM is dull, retracted, and lacks lustre — it appears amber, grey, or grey-blue in colour (compared to the pearl-grey translucency of a healthy TM)
- No erythema, no bulging, no perforation — these features would indicate ASOM, not OME
- Cone of light is absent or distorted
- An air-fluid level or bubbles may be visible through the TM, indicating the presence of fluid that has a gas pocket above it — this is a virtually pathognomonic finding when present
- TM mobility on pneumatic otoscopy is reduced or absent (the fluid behind immobilises the TM)
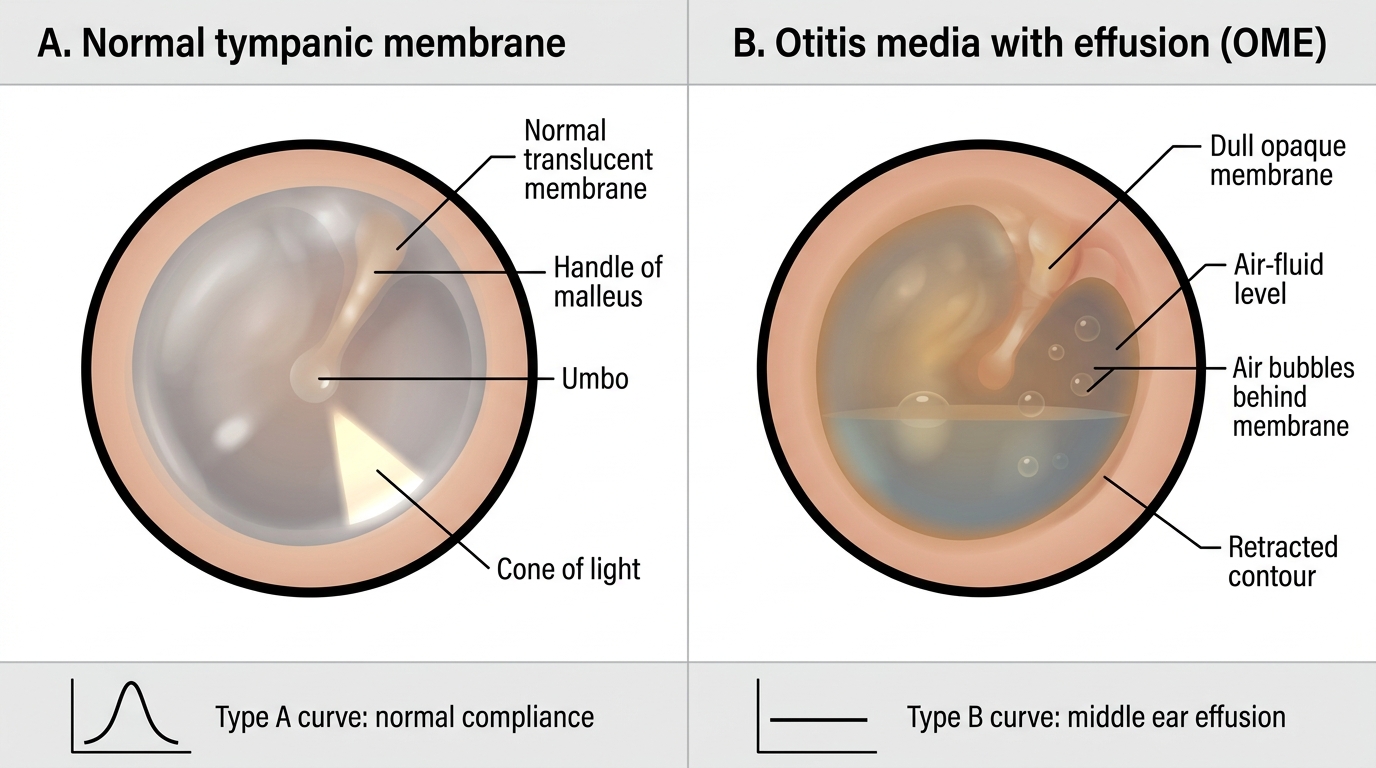
Normal Tympanic Membrane vs Otitis Media with Effusion
Tympanometry:
- Type B (flat) curve: The single most useful test for OME — indicates middle ear fluid is present (near-zero TM compliance regardless of ear canal pressure). Normal ear produces a peaked Type A curve.
- Type C curve: Indicates negative middle ear pressure without effusion — a precursor state of ET dysfunction; the TM is retracted but fluid has not accumulated yet
- Type A curve: Normal — does not exclude OME if bilateral Type B is suspected clinically, but makes it unlikely
- Tympanometry should be repeated at the follow-up visit to document resolution or persistence
Hearing assessment:
- Tuning fork tests: Rinne negative on the affected side (BC > AC); Weber lateralises to the affected ear in unilateral disease — confirming conductive hearing loss. In bilateral OME, Weber may be midline.
- Pure-tone audiometry (PTA): Typically shows a mild to moderate conductive hearing loss of 25–40 dB HL across the frequencies, with a characteristic conductive air-bone gap (normal bone conduction, raised air conduction threshold)
- Behavioural observation audiometry / visual reinforcement audiometry: For children too young for conventional PTA
Additional investigations:
- Adenoid assessment: X-ray lateral view of nasopharynx (soft tissue) or flexible nasoendoscopy to assess adenoid size and ET orifice obstruction
- Flexible nasendoscopy in adults with unilateral OME: MANDATORY to exclude nasopharyngeal carcinoma (NPC) — a nasopharyngeal mass obstructing the ET is a common early presentation of NPC and must not be missed